
Abstract
Introduction/Objectives:
House call programs provide care for homebound patients. We conducted a case-control study to compare hospitalization and/or emergency department (ED) use by patients enrolled in a primary care house call program versus ambulatory (community-dwelling) patients.
Methods:
Program enrollees (cases) were matched by age and self-reported gender to community-dwelling patients (controls). The primary exposure was the combination of hospitalization and/or ED visits for 1 year before the index date (October 1, 2024). We used unadjusted and adjusted conditional logistic regression to determine differences in health care use.
Results:
We identified 26 cases (median [range] age, 84 [66-98] years; 16 [62%] female) and 130 controls. All cases had 4 or more chronic diseases, as compared with 87 (67%) of controls (P = .003). A higher proportion of cases than controls had previous hospitalization and/or ED visits (84.6% vs 27.7%; P < .001). After adjusting for the number of chronic illnesses, no differences in previous hospitalization and/or ED use were identified between groups.
Conclusions:
Cases had more chronic illnesses and more hospitalizations and/or ED visits than community-dwelling controls. The comorbid health burden of participants in the house call program drove greater health care use and justifies a higher level of care for this medically complex patient population.
Background
As the population in the United States ages, their need for medical care increases, especially because 67% of adults older than 65 years have 2 or more chronic conditions. 1 Although the prevalence of chronic diseases increases with age, risk stratification of older individuals can be challenging. For instance, adults in long-term care facilities may have more than 6 chronic conditions, 2 and 49% have severe disability and dependency in 3 or more activities of daily living. 3 Residents of long-term care facilities are expected to be sicker and have more complex illnesses, but the disease complexity of high-risk individuals living at home is less clear. As older people live longer at home with functional debilities, a better understanding is needed about the complexity and health care needs of the homebound primary care population.
One high-risk population comprises disabled, homebound adults with functional debility or cognitive issues. They often have difficulty accessing medical care in the office context and often do not get home care services. 4 Thus, older adults with multiple medical, cognitive, and functional needs may have the highest risk of adverse health outcomes, but they often do not receive care. Our group has established a program that provides palliative care at home to older adult patients who are not enrolled in hospice. 5 These patients are typically older (mean age, 87 years), have a considerable comorbid health burden (Elder Risk Assessment 6 score of 18.2), are frail, and have palliative-minded goals. 5 We have recently expanded this care model to include homebound patients who struggle to access the clinic, even if they do not have palliative goals of care.
In the past decade, a growing number of primary care house call programs have been established in the United States. 7 Previous work on house call programs has shown that these programs serve an older population with cognitive impairment and functional debility. 8 Caring for an older population with frailty may cost 2 to 4 times more than caring for a robust population. 9 However, home-based care for older adults may yield cost savings for this potentially frail population. 10 The Independence at Home demonstration project showed some delay in long-term care placement for those enrolled in a home-based primary care practice. 11
Although some information is available about patients in house call programs, we recognized a generalized lack of information on this unique population, which may have a higher risk of hospitalization. Specifically, it is critical to determine how often these patients are hospitalized and to understand the extent of their illness burden. This important information enables us to ensure that the house call program is being used for the highest-risk individuals, and it also ensures that we are targeting the correct population for enrollment in the house call program. The primary aim of this study was to compare previous hospitalizations or emergency department (ED) visits of participants enrolled in a primary care house call program versus ambulatory (community-dwelling) participants not enrolled in the program. Our secondary aim was to determine the difference in comorbid health burden and individual health conditions between these groups.
Methods
This retrospective, case-control study was reviewed by the Mayo Clinic Institutional Review Board (protocol 24-10618) and exempted from human subject review. Only patients who authorized use of their health records for research were included in the study, in accordance with Minnesota state law. 12 We performed the study within the ethical guidelines of the Declaration of Helsinki. 13 The reporting of this study is in compliance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement for case-control studies (Supplemental Material). 14
Study Setting
We conducted this case-control study within a community-based primary care practice that provides care for 152 000 unique patients annually. The practice is part of Mayo Clinic (Rochester, Minnesota), a large academic medical center, with care teams distributed across 5 locations in the region. Primary care team members include advanced practice providers, medical residents, family medicine physicians, internal medicine physicians, and physicians specializing in other areas and procedural care. 15
House Call Program
Our house call program is designed to accommodate patients with the highest risk of functional decline. Clinicians refer patients to the program with an electronic order. Eligible patients are aged 60 years or older and have an established relationship with a primary care clinician at Mayo Clinic (Rochester or Kasson, Minnesota). Patients must live within an approximately 15-mile radius of our institution (which includes rural surrounding communities) and have difficulty getting to the clinic for medical care. Eligible patients also must require assistance with at least 2 activities of daily living. Participants typically have 2 or more chronic health conditions (eg, diabetes, dementia, heart failure, chronic obstructive pulmonary disease [COPD], and cancer); and many patients have a high Elder Risk Assessment 6 score (>15), have had hospital stays in the year preceding program enrollment, and meet frailty criteria. Individuals are ineligible if they are experiencing homelessness, enrolled in hospice, monitored by a transplant team or dialysis team, or have active psychiatric issues that could compromise cooperation in the program. The patient or responsible party is contacted to confirm interest. If the patient wishes to enroll, then an advanced practice provider completes a comprehensive geriatric assessment (medication review, advanced care planning, and functional and cognitive assessment). The enrollment process is summarized in the Figure 1.

Enrollment Process for the Primary Care House Call Program. Enrollment begins with an electronic order from the patient’s PCC. The order is reviewed by the program’s admission team to verify that eligibility criteria are met. After the patient and family agree to enrollment, an APP completes a comprehensive geriatric assessment.
Identification of Cases and Controls
We searched electronic health records (EHRs) at our institution to identify cases and controls. Cases were defined as patients enrolled in the primary care house call program as of October 1, 2024 (the index date). The study size was determined by the number of program enrollees identified. We matched each case by age and self-reported gender to exactly 5 controls, defined as community-dwelling patients with an assigned primary care clinician. We randomly manually verified enrollment for more than 50% of records in the house call program. All participants had interacted with their established primary care clinician within the 3 years before the index date (from January 1, 2022, through October 1, 2024). We excluded patients who lacked a primary care clinician or resided in a skilled nursing facility. We reduced risk of bias (referral bias) by including only cases and controls from our primary care practice.
Exposures and Outcomes
Using the EHR, we abstracted demographic characteristics, health care use, and comorbid health conditions. We identified prevalent exposures and risk factors (eg, health care use and chronic illnesses) for 1 year before the index date. Patient age as of September 30, 2024, was recorded. Gender (male or female) and race/ethnicity (non-Hispanic White vs other) were self-reported. We did not further stratify patients by race/ethnicity to maintain their privacy.
We used International Classification of Diseases, Tenth Revision codes to identify comorbid health conditions, directly treated in primary care, that can lead to hospital stays. Specifically, we sought to determine whether participants had diagnosis codes for heart failure, diabetes, chronic kidney failure, depression, anemia, and COPD. We determined the number of chronic conditions per patient by using ACG System software (version 13.01; The Johns Hopkins University) 16 and categorized patients into subgroups of 0 or 1 conditions, 2 to 3 conditions, and 4 or more conditions to reflect multimorbidity. 17 We further used an established ACG System algorithm to identify patients with frailty (ie, we searched for codes associated with frailty concepts, such as malnutrition, dementia, visual loss, pressure injury, urinary incontinence/retention, loss of weight, fecal incontinence, social support needs, walking difficulty, and falls). Chronic conditions were recorded as binary outcomes (ie, present vs absent) for each patient.
We used billing data to determine ED visits, hospitalizations, and the number of hospital days for the year before the index date. For the primary analysis, we combined ED visits and/or hospitalizations and treated it as a single, binary measure. That is, patients were categorized either as having: (1) an ED visit and/or a hospital stay in the preceding year; or (2) no ED visits and no hospital stays in the preceding year. For the secondary analysis, we reported hospitalization and ED visits separately.
Statistical Analysis
Patient demographic and clinical characteristics are summarized using descriptive statistics. Continuous variables are reported as mean (SD) or median (range), depending on the data distribution. For statistical testing, we used the Fisher exact test for categorical variables, the χ2 test for binary outcomes, and the Kruskal-Wallis test for continuous outcomes in unadjusted descriptive comparisons. Unadjusted and adjusted conditional logistic regression was used to determine differences in health care use for cases versus controls. We conducted a multivariable analysis based on chronic illness count. Odds ratios (ORs) and 95% CIs are reported for hospitalizations and ED visits. Statistical significance is inferred when P < .05.
Results
Patient Characteristics
We identified 26 patients enrolled in the house call program (cases) and 130 age- and gender-matched community-dwelling individuals (controls). The median (range) participant age was 84 (66-98) years. More than 46% of patients were older than 85 years. The cohort had more female than male participants (61.5% vs 38.5%). We did not identify any differences in race/ethnicity between cases and controls.
Demographic characteristics are summarized in Table 1. No data were missing for either cases or controls. The median number of conditions for cases was 14.5, as compared with 5 in the control group (P < .001). All cases (100%) had 4 or more conditions, as compared with 67% in controls (P = .003). A greater proportion of cases had heart failure, depression, anemia, COPD, and chronic kidney disease, as compared with the controls. Both groups had similar rates of diabetes. Among cases, 89% were frail, as compared with 35% of controls (P < .001).
Demographic and Clinical Characteristics of Patients Enrolled in a House Call Program and Age- and Gender-Matched Controls.
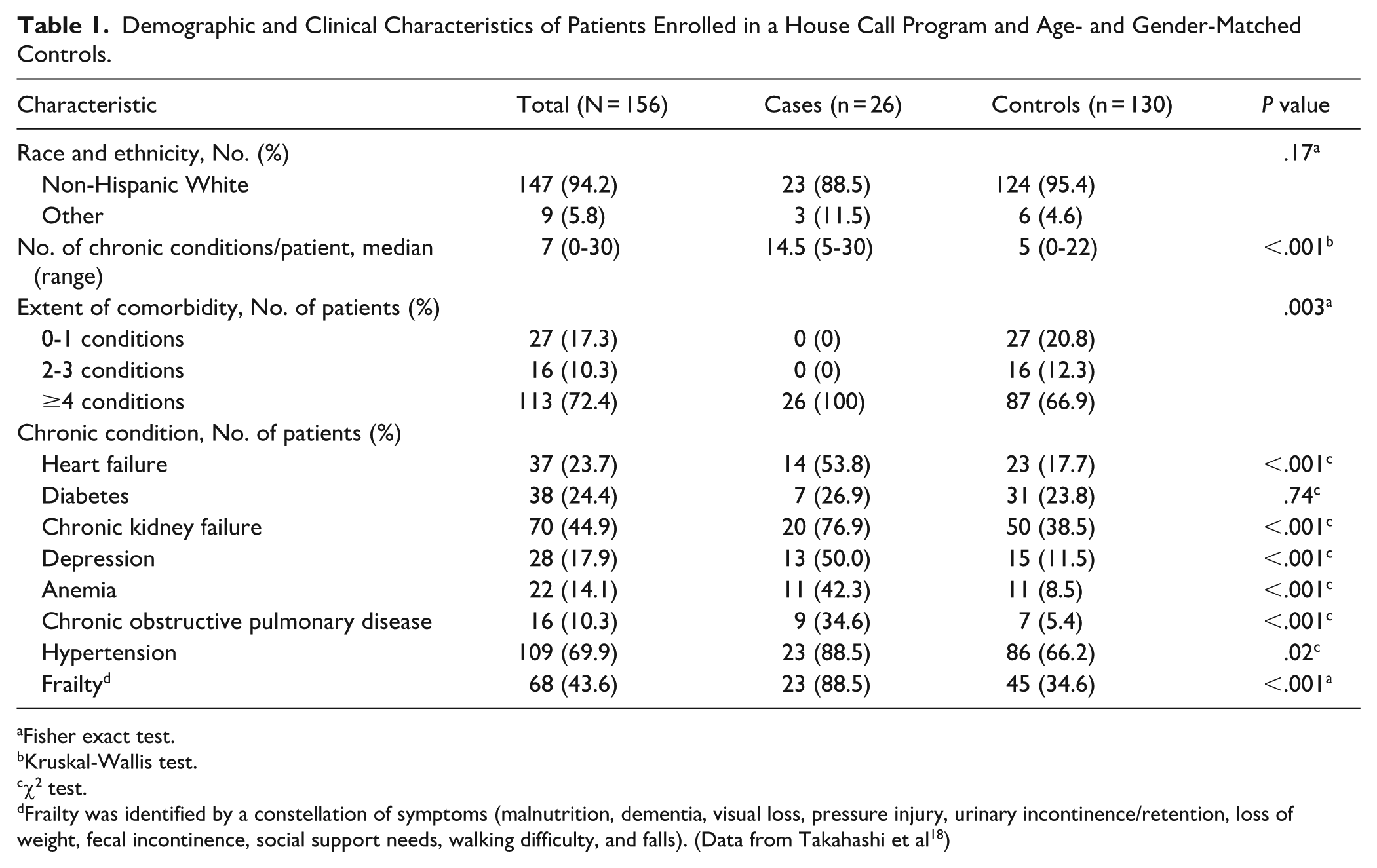
Fisher exact test.
Kruskal-Wallis test.
χ2 test.
Frailty was identified by a constellation of symptoms (malnutrition, dementia, visual loss, pressure injury, urinary incontinence/retention, loss of weight, fecal incontinence, social support needs, walking difficulty, and falls). (Data from Takahashi et al 18 )
Health Care Use
The number of hospitalizations and ED visits are summarized in Table 2. For cases, 85% had a hospital stay or ED visit in the preceding year, as compared with 28% of the control group (P < .001). Cases had more individual hospital stays and ED visits and a higher median number of hospital days, as compared with controls. Table 3 shows results of the conditional logistic regression analysis. The unadjusted odds for the combined outcome of hospitalization and/or ED visit were higher for cases (OR, 11.69 [95% CI, 3.90-35.06]). However, after adjusting for the number of chronic conditions, we observed no difference between cases and controls for hospitalization and/or ED visit (OR, 3.33 [95% CI, 0.90-12.32]).
Hospitalization and Emergency Department Visits.

Abbreviation: ED, emergency department.
Fisher exact test.
χ2 test.
Kruskal-Wallis test.
Unadjusted and Adjusted Conditional Logistic Regression for Health Care Use and Chronic Conditions. a

Abbreviations: ED, emergency department; OR, odds ratio.
Odds of the outcome for cases vs controls.
Discussion
In this study, patients enrolled in a primary care house call program (cases) differed from age- and gender-matched community-dwelling patients (controls) in important ways. Cases had much greater health care use, with a nearly 12-fold higher odds of hospitalization and/or an ED visit than controls. This difference appeared to be driven by the higher comorbid health burden among cases because the analysis that adjusted for the number of chronic conditions subsequently showed nonsignificant differences in the odds of each outcome for cases and controls.
Our findings show that patients with hospitalization and high comorbid health conditions were being enrolled in the house call program. Patient characteristics were concordant with criteria for potential enrollment in an Independence at Home model, which include hospitalization or postacute care within the previous 12 months, 2 or more chronic illnesses, and/or 2 or more impairments in activities of daily living. 19 Thus, our approach appears to be correctly targeting the appropriate population for a house call program. Health care needs often are considerable for homebound individuals. In 1 program of 179 patients, investigators reported that 61% of patients had been hospitalized before enrollment in a home visit program, as compared with 38% after enrollment (the investigators assessed equal periods before and after enrollment). 20 In a Department of Veterans Affairs study, 41% had a hospitalization in the 6 months before enrolling in a house call program. 21
All patients in our primary care house call program had multiple comorbid health conditions, and they had an approximately threefold higher median number of illnesses, as compared with controls. For specific illnesses, 54% of cases had heart failure, as compared with 18% of controls. In the unadjusted analysis, cases had greater than sevenfold odds of depression. The differences between cases and controls are consistent with findings reported previously. An assessment of patients enrolled in a Department of Veterans Affairs home-based primary care program showed a higher comorbid health burden and a higher prevalence of heart failure, as compared with those not enrolled. 22 In a Japanese study, more than half of 253 house calls were to patients with multiple comorbid conditions. 23 In a study of a Medicare Advantage cohort having home-based visits (n = 161 801), investigators noted a high burden of comorbid health conditions (Charlson Comorbidity Index score of 4.3). 24
Our findings support a specialized care model for this high-risk population with high levels of medical care use. We believe that house call programs provide patients with an opportunity for enhanced management of chronic diseases through quarterly visits with a primary care clinician. Additionally, such programs potentially can facilitate implementation of specific interventions, including goal-directed medical therapy for heart failure, depression management, and advanced care planning to better understand whether recurrent hospitalization is within a patient’s goals of care.
This study has various strengths and weaknesses. Patients were in an established house call program that actively collects robust medical information, including health outcomes and comorbid conditions. It is possible that some hospitalizations or chronic conditions were not captured, but given that program participants had physical or cognitive limitations, such outcomes are unlikely to occur outside of our institution. If some patients were not homebound, a bias could exist in which hospitalizations would be captured for cases but not necessarily for more-mobile controls, who could perhaps seek care at different hospitals; this potential bias would then show a higher hospitalization rate for cases. However, we minimized this bias by selecting cases and controls only from patients empaneled to our primary care practice because these patients typically would also get hospital and ED visit care at our institution. Our study had a small sample size and limited power, which may have reduced the ability to identify significant differences between cases and controls. We also did not adjust our analysis for other potential confounders, such as socioeconomic status or caregiver support. Our cohort comprised mostly non-Hispanic White individuals, consistent with the population of the upper midwestern United States, 25 and so these results may not generalize to other populations. The study was conducted at a US health care system and may not reflect practices in other countries.
Conclusion
Compared with age- and gender-matched ambulatory patients, homebound patients enrolled in our house call program had a higher comorbid health burden that drove greater health care use. Developing and sustaining new models of care with more intensive management will be important for these patients, who often have more negative health outcomes, such as hospitalizations and ED visits.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319261432120 – Supplemental material for Health Care Use and Outcomes Among Participants Enrolled in the Mayo Clinic Primary Care House Call Program: A Case-Control Study
Supplemental material, sj-docx-1-jpc-10.1177_21501319261432120 for Health Care Use and Outcomes Among Participants Enrolled in the Mayo Clinic Primary Care House Call Program: A Case-Control Study by Paul Y. Takahashi, Bonnie C. Sohn, Brandon P. Verdoorn, Anupam Chandra, Natalie F. Mohammad, Lindsey M. Philpot, Rachel D. Havyer, Daniel L. Roellinger, Matthew G. Johnson, Jennifer West, Gregory J. Hanson and Maria D. Mendoza De la Garza in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
June Oshiro, PhD, ELS, Mayo Clinic, substantively edited the manuscript. The Scientific Publications staff at Mayo Clinic provided proofreading, administrative, and clerical support.
Author Note
Presented as a poster at the European Geriatric Medicine Society 21st Congress; September 24 to 26, 2025; Reykjavik, Iceland. Portions of this manuscript have been published in abstract form: Takahashi P, Sohn B, Chandra A, Roellinger D, Johnson M, Hanson G. P-0920 Evaluating Health Outcomes in Housecall Program Patients: A Case-Control Study on Hospitalization and Emergency Department Visits. 2025. Available from ![]() .
.
Ethical Considerations
The study was reviewed by the Mayo Clinic Institutional Review Board (protocol 24-10618) and was determined to be exempt from human subject review.
Consent to Participate
Only patients who authorized use of their health records for research were included in the study.
Author Contributions
Paul Y. Takahashi, MD, MPH: Conceptualization, funding acquisition, investigation, methodology, project administration, supervision, writing original draft, and writing final draft and edits. Bonnie C. Sohn, MD: Conceptualization, investigation, methodology, writing original draft, and writing final draft and edits. Brandon P. Verdoorn, MD: Conceptualization, investigation, and writing final draft and edits. Anupam Chandra, MD: Conceptualization, investigation, and writing final draft and edits. Natalie F. Mohammad, APRN, CNP: Conceptualization, investigation, and writing final draft and edits. Lindsey M. Philpot, PhD, MPH: Conceptualization, investigation, methodology, and writing final draft and edits. Rachel D. Havyer, MD: Conceptualization, investigation, and writing final draft and edits. Daniel L. Roellinger: Conceptualization, formal analysis, investigation, and writing final draft and edits. Matthew G. Johnson, MPH: Conceptualization, formal analysis, investigation, writing original draft, and writing final draft and edits. Jennifer West, MPH: Conceptualization, data curation, funding acquisition, and writing final draft and edits. Gregory J. Hanson, MD: Conceptualization, funding acquisition, investigation, methodology, and writing final draft and edits. Maria D. Mendoza De la Garza, MD: Conceptualization, methodology, and writing final draft and edits.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received funding support from the Division of Community Internal Medicine, Geriatrics, and Palliative Care, Mayo Clinic.
Data Availability Statement
All relevant information is reported in the manuscript. For additional queries, please communicate with the corresponding author*.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.