
Abstract
Objectives:
The objective of this study was to assess and compare diet quality and adherence to DASH nutrient recommendations between hypertension and non-hypertensive older African American adults.
Methods:
A cross-sectional analysis was conducted using data collected between October 2021 and July 2022 from 100 African American adults aged ≥55 years. Diet was assessed using a validated food frequency questionnaire, and diet quality was quantified via the Healthy Eating Index (HEI-2015). DASH adherence was measured by comparing mean intake of sodium, potassium, magnesium, calcium, fiber, and % kcal from carbohydrates, protein, total fat, and saturated fat to DASH dietary targets. Participants self-reported hypertension status, sociodemographic, health, and food access information. Statistical analyses included t-tests and chi-square tests to compare nutrient means and adherence rates between participants with and without hypertension.
Results:
Participants had a mean age of 68.6 years; 71% were female, and 45% were classified as obese. The majority (74%) scored a grade of “fair” or “poor” on the HEI-2015. While HEI-2015 fruit and vegetable sub-scores met recommendations, those for sodium, added sugar, and saturated fat did not. Hypertensive participants consumed significantly more sodium than non-hypertensive (P < .001), with the former consuming almost double their recommended amount (2884 ± 1103 vs 1500 mg). Additionally, hypertensive patients got fewer calories from carbohydrates (−3.3% kcal, P = .032), and more from protein (+2.5% kcal, P = .004) compared to their non-hypertensive peers. Neither group met potassium, calcium, magnesium, or fiber targets, with no difference between groups. About 30% reported food insecurity, yet over 70% still reported good availability of healthy foods in their neighborhood.
Conclusion:
Findings indicate widespread nutrient inadequacies and excessive sodium intake among older African American adults, with hypertensive participants consuming particularly high levels of sodium. Despite adequate fruit and vegetable intake and reported access to healthy foods, both groups failed to meet key DASH nutrient targets. These results highlight the need for culturally tailored, community-based interventions that specifically address sodium reduction and DASH-aligned nutrient intake to reduce cardiovascular disease risk in this underserved population.
Keywords
Introduction
Hypertension continues to be one of the most common and avoidable risk factors for cardiovascular disease and death in the United States. Recent CDC data show that almost half of U.S. adults (47.7%) have hypertension, and non-Hispanic Black Americans have the highest rates of any racial/ethnic group. 1 The incidence of hypertension is estimated at 23% in adults aged 18 to 39 years, 53% in those 40 to 59 years, and over 71% among adults aged 60 years and older. 1 Moreover, African Americans tend to develop hypertension earlier and experience more severe cases and more complications than their White counterparts.2,3
Hence, diet modification is a cornerstone of hypertension prevention and management. Clinical guidelines emphasize the adoption of a heart-healthy eating pattern for all adults to reduce hypertension risk, alongside other healthy lifestyle choices. The Dietary Approaches to Stop Hypertension (DASH) diet is an evidence-based dietary pattern proven to lower risk for hypertension and reduce blood pressure and improve cardiovascular outcomes for those with hypertension. The DASH diet emphasizes high intakes of fruits, vegetables, whole grains, and low-fat dairy, with adequate lean protein (such as fish, poultry, beans, nuts, and low-fat dairy) and fiber, and recommends limiting saturated fat, added sugars. 4 High sodium intake is strongly linked to elevated blood pressure.5,6 On the other hand, low intake of potassium, which is thought to balance sodium’s effects, is also a risk factor.5,6 The DASH diet specifically recommends a limit on sodium intake of around 1500 mg/day for those who already have hypertension and provides guidelines for the intake of potassium, calcium, and magnesium. 7 Adhering to DASH can yield clinically meaningful blood pressure reductions, as reported in a meta-analyses that showed a systolic blood pressure drop of roughly 3 to 4 mm Hg on average. 8 Notably, 1 recent analysis of the DASH trial found the diet conferred particularly pronounced cardiovascular benefits for African American participants compared to Whites. 9
Despite decades of research, national surveys consistently show that most U.S. adults do not meet DASH guidelines, particularly due to high sodium intake and persistently low potassium intake.10,11 For older African American adults of low socioeconomic status, following the DASH diet faces additional challenges. These include limited knowledge about nutrition and confusion caused by conflicting or complicated advice. 12 These barriers may directly impede consistent access to DASH-aligned foods, including fresh produce, low-fat dairy, and whole grains, thereby undermining the feasibility of DASH adherence despite its proven benefits. 13
Although the disproportionate burden of hypertension among older African American adults is well documented,14 -16 less is known about how closely dietary intake in this population aligns with DASH nutrient targets and whether adherence differs by hypertension status. The objective of this study was to assess and compare diet quality and adherence to DASH nutrient recommendations between hypertension and non-hypertensive older African American adults. By identifying specific nutrient shortfalls and group-level differences, this study aims to address an important knowledge gap and inform culturally tailored, community-based dietary interventions to support improved diet quality and blood pressure control among African American seniors.
Methods
Design and Participants
This study used a cross-sectional design and analyzed data from the COVID-19, Food Insecurity, Exercise, and Dietary history (C-FED) study. 17 The C-FED study was a survey of older African American adults recruited through 2 churches in South Los Angeles. South Los Angeles is located within Service Planning Area 6 (SPA 6), a predominantly low-income and underserved region of Los Angeles County with a high burden of health disparities. Participants were eligible if they self-identified as African American and were aged 65 years or older, or aged 55 years or older and had a chronic condition. Because data were collected during the COVID-19 pandemic, the original study aimed to survey individuals at elevated risk for COVID-19. Survey data were collected between October 2021 and July 2022 via email, telephone, or in-person interviews. A total of 108 participants completed the C-FED surveys. Participants were excluded from the present analysis if they had implausible total energy intake, defined as daily caloric intake outside established physiologic ranges.18 -20 The study protocol was reviewed and approved by the Institutional Review Board at the author’s institution (IRB #1776688).
Data Collection and Measures
Measures analyzed in this study were derived from self-reported survey data collected as in the C-FED study, using validated instruments as described below.
Hypertension status: Participants self-reported physician-diagnosed chronic conditions, including hypertension. Participants were categorized as having hypertension or not based on their self-report, regardless of any additional chronic conditions they may have reported. Treatment status for hypertension was not incorporated into the present analysis.
Dietary intake and DASH nutrients: Dietary intake was assessed using the Diet History Questionnaire III (DHQ III), a validated instrument containing 135 items on foods and beverages consumed over the past year.18,19 DHQ III responses were used to calculate the Healthy Eating Index–2015 (HEI-2015), which measures adherence to the U.S. Dietary Guidelines for Americans. 20 To evaluate adherence to the Dietary Approaches to Stop Hypertension (DASH) dietary pattern, we examined key nutrient components emphasized in DASH guidelines. Specifically, intakes of sodium, potassium, calcium, magnesium, and dietary fiber were assessed relative to recommended targets or limits. In addition, the distribution of energy across macronutrients—specifically, the percentage of kilocalories from carbohydrates, protein, total fat, and saturated fat—was calculated and compared to DASH standards. These variables were used to evaluate dietary quality in relation to hypertension status.
Demographic characteristics: Age was treated as a continuous variable (mean 68.5 ± 8.7 years). Gender was categorized as male or female. Educational attainment was grouped into 5 categories: (1) no high school diploma, (2) high school diploma, (3) some college, (4) bachelor’s degree, and (5) master’s or doctoral degree. Participants also reported their perceived health literacy on a Likert scale from 1 (very good) to 5 (poor), reflecting their confidence in understanding and using health information. A higher score indicates lower perceived comprehension and communication effectiveness in healthcare settings. Responses about marital status were categorized as married or living with a companion, divorced or separated, single, never married, or widowed. Living arrangements were categorized as living alone versus not living alone. Annual household income was classified into the following categories: <$30 000, $31 000 to $70 000, and >$70 000. The original income categories were based on common U.S. survey methods, and the re-categorization aimed to distinguish levels of income. The categories chosen approximately reflect the Department of Housing and Urban Development’s cutoffs for defining low income (~$67k) and extremely low income (~$25k) in Los Angeles County at the time of data collection. 21 Participants also reported whether they had health insurance coverage (yes/no), and if yes, they reported their health insurance carrier.
Health status and lifestyle behaviors: Participants rated their general physical health as Excellent/Very Good, Good, or Fair/Poor. Body mass index (BMI) was calculated and classified as normal/underweight (<25 kg/m2), overweight/obese (≥25 kg/m2), or obese (≥30 kg/m2).
Lifestyle factors: Lifestyle factors included smoking status, alcohol consumption, and physical activity. Smoking status was assessed using standardized questions adapted from the PhenX Toolkit, asking participants whether they currently smoke cigarettes (Yes or No).22 -24 Alcohol consumption was assessed by asking participants, “How often have you drunk any alcoholic beverages, such as beer, cider, wine, spirits, or cocktails?” Responses were coded on a 5-point scale (0 = never, 1 = once a week, 2 = twice a week, 3 = 3 times a week, 4 = 4 or more times a week) and were classified according to U.S. alcohol guidelines, with women consuming ≤1 drink per day and men consuming ≤2 drinks per day considered within the recommended limits. 25 Physical activity was measured using the Yale Physical Activity Survey (YPAS), which captures the total minutes spent in moderate or vigorous activity per week. 26 Respondents were further categorized according to physical activity guidelines as engaging in <150 min/week (insufficient activity) or ≥150 min/week (adequate activity). 27
Food access: Food access was conceptualized as food insecurity and the neighborhood food environment. Food insecurity was assessed using the 6-item short form of the USDA U.S. Household Food Security Survey. 28 This measure has been previously validated as correctly classifying 97.7% of households in the U.S.29,30 Responses were computed to a dichotomized variable: “food insecure” (a score of 1 or higher) versus “not food insecure” (a score of 0). Neighborhood food environment was measured using the 3-item scale from the Multi-Ethnic Study of Atherosclerosis (MESA). Items were: Q1. 31 “The fresh fruits and vegetables in my neighborhood are of high quality”; Q2. “A large section of fresh fruits and vegetables is available in my neighborhood”; and Q3. “A large selection of low-fat products is available in my neighborhood.” Response options were strongly agree, agree, neither agree nor disagree, disagree, or strongly disagree.
Statistical analysis: Descriptive statistics were used to summarize participants’ sociodemographic, socioeconomic, health, lifestyle, and food access characteristics. Categorical variables (eg, gender, education, marital status, smoking, alcohol use, physical activity category, food insecurity, and neighborhood food environment ratings) were presented as frequencies and percentages. Continuous variables (eg, age, BMI, and minutes of physical activity per week) were summarized using means and standard deviations. Dietary intakes were evaluated relative to the DASH nutrient targets. Targets are the same for most nutrients regardless of hypertensive status, except sodium, which has a lower target for people with hypertension. Mean intakes, standard deviations, and deviations from DASH recommendations were calculated for key nutrients (sodium, potassium, calcium, magnesium, and dietary fiber) and macronutrient energy contributions (percent of calories from carbohydrates, protein, total fat, and saturated fat). Independent-samples t-tests were used to compare mean nutrient intakes between participants with and without hypertension, and non-parametric tests were used to compare HEI component scores. Results were reported as mean differences with corresponding P-values, and statistical significance was set at P < .05. All analyses were conducted using SAS 9.4 (SAS Institute, Cary, NC).
Results
Participant Characteristics and Food Environment
Table 1 presents the sociodemographic, health, lifestyle characteristics, and food access of the 100 older African American adult study participants. Mean age was 68.6 ± 8.6 years. The majority were women (71%), and nearly half (45%) met criteria for obesity (BMI ≥ 30 kg/m2), while 28% were overweight (BMI = 25-29.9 kg/m2). About 15% had no high school diploma, 24% had a high school diploma, and 61% had some college or a bachelor’s degree or higher. Thirty-seven percent were married or living with a partner.
Participant Sociodemographic Characteristics, Health, Lifestyle, and Food Access (n = 100).

Socioeconomic indicators showed that the majority (84%) had an annual income of <$70 000 (43% <below $30 000; 41% $30 000-$70 000). Approximately one-third (30%) of participants experienced food insecurity. Most participants perceived their neighborhood food environment as favorable: 69% agreed that fruits and vegetables in their neighborhoods were of high quality, 73% that a large selection of fruits and vegetables was available, and 68% that a large selection of low-fat products was accessible. Three-quarters (74%) had overall positive ratings of their neighborhood food environment.
Lifestyle patterns showed that participants engaged in an average of 286 ± 702 min of moderate-to-vigorous physical activity per week, with 69% classified as having insufficient activity (<150 min/week) and 31% meeting the recommended level (≥150 min/week). Nine percent were current smokers, and 65% did not drink any alcohol. Approximately 80% of participants reported having “good” or “very good” health literacy, while only 8% indicated “poor” or “very poor.”
Nutrient Intake and DASH Adherence
Table 2 compares mean daily nutrient intakes of participants with and without hypertension to DASH dietary targets. Overall energy intake was modest (1518 ± 624 kcal/day) and lower than standard recommendations. Participants with hypertension consuming significantly more calories than those without hypertension (1627 vs 1334 kcal/day; P = .041).
Mean Daily Nutrient Intakes Compared With DASH Dietary Targets.

Abbreviation: HTN, hypertension.
Values are mean ± SD. P values from independent-samples t-tests comparing participants with and without hypertension.
P < .05. **P < .01. ***P < .001.
Across the sample, mean sodium intake was 2656 mg/day, which is above the DASH limit of 2300 mg/day and nearly double the stricter 1500 mg/day threshold recommended for hypertensive adults. In general, participants without hypertension were under the recommended limit with an average intake of 2267 mg/day, while participants with hypertension consumed roughly 600 mg/day more sodium than their non-hypertensive peers, putting them well above both limits (Figure 1, P < .001). Other DASH nutrients were consistently below targets (Figure 1). Potassium averaged 2598 mg/day, calcium 963 mg/day, magnesium 312 mg/day, and dietary fiber 19 g/day. These values fell well below recommendations for all nutrients: potassium by approximately 2000 to 2300 mg/day (~55% of target), calcium by approximately 250 to 350 mg/day, magnesium by approximately 200 mg/day, and fiber by approximately 10 to 11 g/day. None of these nutrient intakes differed significantly by hypertension status (P > .27).

DASH nutrient differences by hypertension status.
Within the macronutrient distribution, the percentage of carbohydrate and protein contribution to total calories varied slightly from DASH recommendations among all participants (carbohydrates contributed 53% vs recommended 55%; and protein 17% vs recommended 18%) (Table 2; Figure 2). Significant group differences were found for carbohydrates and protein, where hypertensive participants derived a significantly smaller proportion of calories from carbohydrates and a greater proportion from protein (P < .05). Consumption of carbohydrates by non-hypertensive adults was above the carbohydrate target (+1.0%), while that for hypertensive adults was below (−3.3%) (P = .032). For protein, non-hypertensive participants averaged 2.6% below the target, while hypertensive adults were nearly on-target, producing a statistically significant −2.5% difference (P = .004). Total fat and saturated fat deviated the most (32% vs recommended
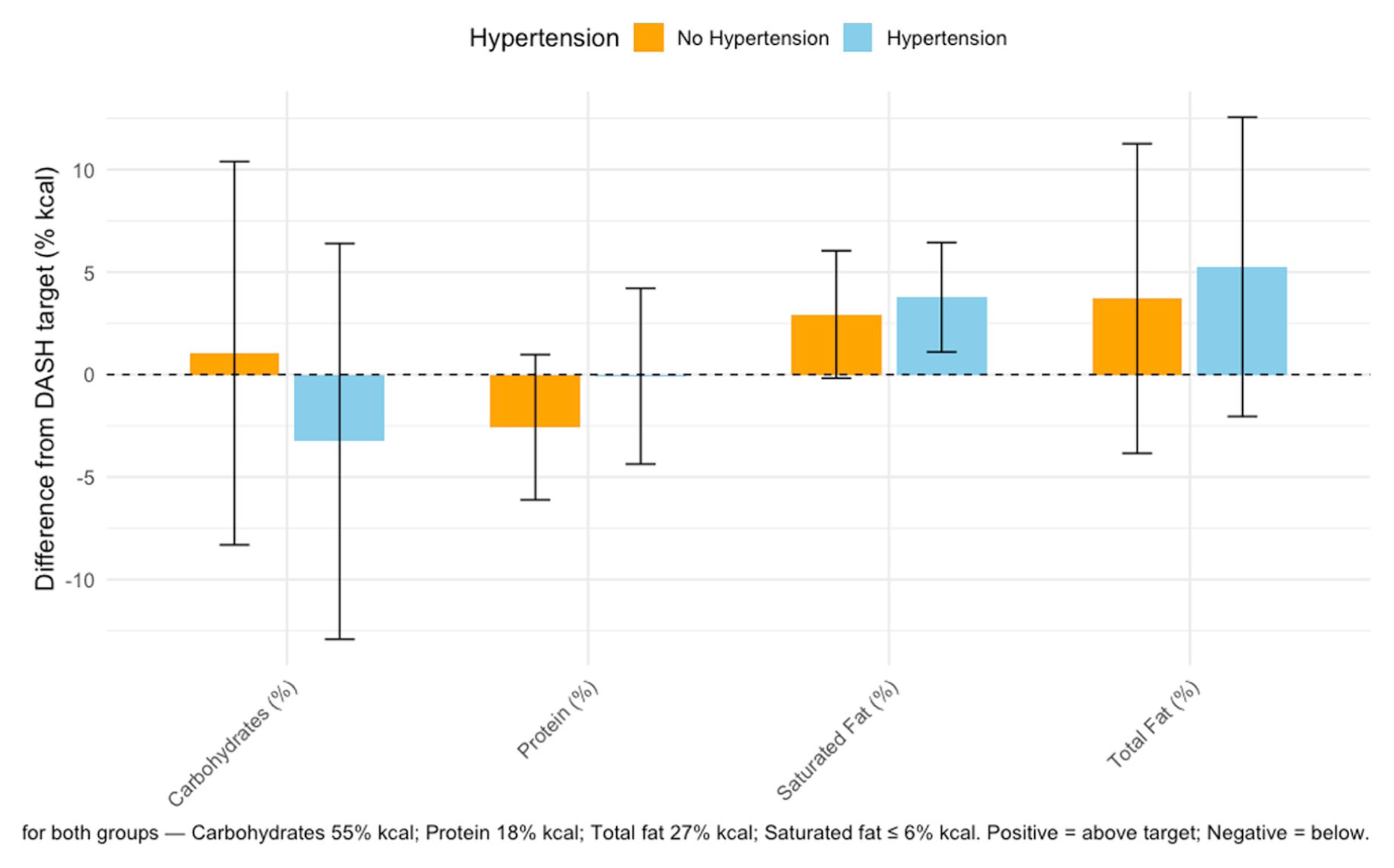
Macronutrient % of kcal—difference from target (±SD).
Healthy Eating Index (HEI-2015) Scores
The mean total Healthy Eating Index (Table 3) was 68 ± 8.7, and scores were similar across hypertension and non-hypertension groups (69.1 vs 67.4; P = .15). When classified by overall HEI-2015 grade, no participants achieved an “A” (excellent) rating, and only 7% scored within the “good” range (80-89). Most participants fell into the “fair” (41%) or “poor” (33%) categories, and nearly one-fifth (19%) had scores below 60, indicating failing adherence.
Mean Total Healthy Eating Index.
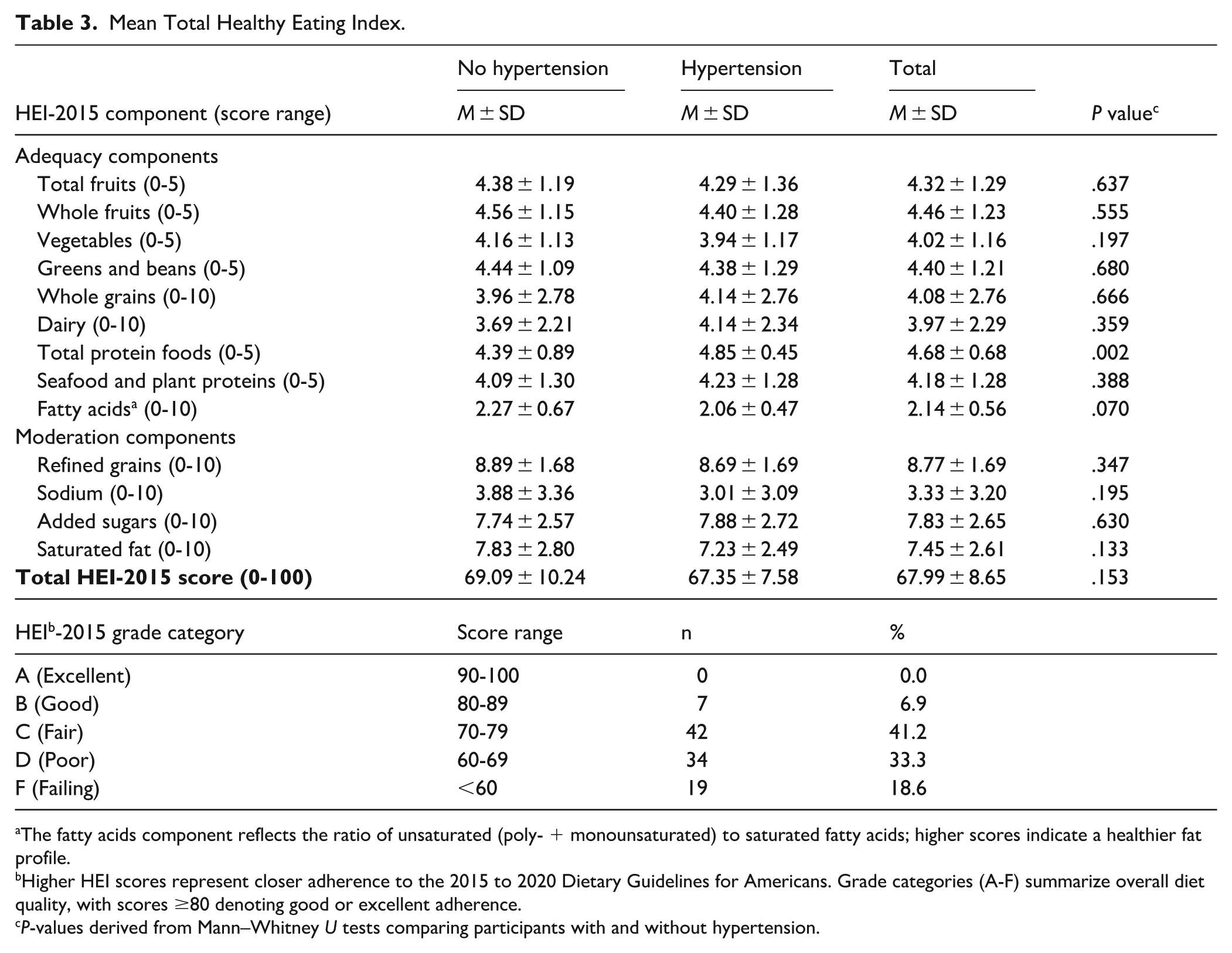
The fatty acids component reflects the ratio of unsaturated (poly- + monounsaturated) to saturated fatty acids; higher scores indicate a healthier fat profile.
Higher HEI scores represent closer adherence to the 2015 to 2020 Dietary Guidelines for Americans. Grade categories (A-F) summarize overall diet quality, with scores ≥80 denoting good or excellent adherence.
P-values derived from Mann–Whitney U tests comparing participants with and without hypertension.
Participants intakes were close to targets for adequacy components, particularly for total fruits (mean 4.3 of 5), whole fruits (mean 4.5 of 5), and total protein foods (mean 4.7 of 5). However, scores were low for whole grains (mean 4.1 of 10), dairy (mean 4.0 of 10), and the fatty acids ratio (mean 2.1 of 10), reflecting suboptimal intake of whole grains and healthy fats. Scores did not differ significantly between those with and without hypertension, except for total protein foods, where those with hypertension consumed significantly more protein than those without (4.9 vs 4.4; P = .002).
For moderation components, where lower intake earns higher scores, participant intake was close to targets for refined grains (8.8 of 10), saturated fats (7.5 of 10), and added sugars (7.8 of 10) but did not match targets for sodium (3.3 of 10), consistent with nutrient level findings. There were no statistically significant differences between the groups.
Discussion
In this study of older African American adults in an underserved community, we found that overall diet quality was “fair” or “poor” based on dietary guidelines. Our findings indicate a broad divergence from DASH dietary targets across this African American older-adult sample, with sodium intake standing out as the most concerning nutrient gap. Average sodium intake exceeded the general DASH limit of 2300 mg/day and was nearly double the stricter 1500 mg/day guideline recommended for hypertensive adults. Moreover, hypertensive participants consumed substantially more sodium than their non-hypertensive peers, a large and significant difference of nearly 617 mg/day. These findings suggest that dietary shortfalls are both pervasive at the population level and uniquely problematic among hypertensive individuals. The large standard deviations observed for sodium and potassium further highlight wide variability, suggesting that while some individuals approach recommended levels, many consume nutrients far outside guideline ranges. This pattern mirrors national data showing persistently high sodium consumption, especially in African American communities. 32 National NHANES data show that sodium intake among African American adults with hypertension increased by approximately 20% between 1999 and 2012, significantly higher than the approximately 2% increase observed among non-Hispanic White adults. Black adults also demonstrate a 16% higher risk of poor diet quality compared with White adults in large national cohorts.28,32
Beyond sodium, the diets of both hypertensive and non-hypertensive participants fell short on several DASH-promoted, hypertension-protective nutrients. The overall caloric intake was below the DASH recommendation of 1800 to 2000 calories, but was consistent with intake reported by others for similar populations. 33 Intakes of potassium, calcium, magnesium, and dietary fiber, whole grains and were consistently below recommended thresholds. In particular, the average intake of potassium barely reached half (56%) of the recommended target. Meanwhile, saturated fat, which has been linked to cardiovascular disease, was over 50% above the recommended limits, with no significant differences between groups. Further analysis of the Healthy Eating Index components indicated that most fiber intake originated from refined rather than whole-grain sources. This pattern is consistent with national data showing refined carbohydrates are the more common choice among older African Americans and those of lower socioeconomic status.14,15,26 In contrast, DASH guidelines emphasize whole grains as a primary source of soluble fiber associated with improved lipid profiles and lower blood pressure.10,12,13 Therefore, total fiber quantity alone may overstate potential cardiovascular benefits if the majority is derived from refined rather than whole-grain sources. These deficits appear to represent population-wide inadequacies rather than hypertension-specific behaviors. These findings are consistent with earlier studies that reported inadequate nutrient intake by older African Americans. 34
Notably, participants in our study scored relatively well on fruit and vegetable intake, with HEI component scores near or above 4 out of 5 for total fruits, whole fruits, total vegetables, and greens and beans. This pattern contrasts with previous research in similar populations, where up to 77% of older African Americans failed to meet USDA guidelines for fruit and vegetable consumption. 35 However, consistent with prior studies, we found no significant differences in fruit and vegetable intake between participants with and without hypertension. 35 More recent studies support this shortfall: one found that only 23% of older African Americans achieved the combined recommended fruit + vegetable servings, and African Americans consumed significantly fewer portions than other racial/ethnic groups. 36 Another population-based analysis found multiple socioeconomic and geographic variables were independently associated with poor diet quality, including fruit and vegetable intake, among Black adults. 37 While the relatively high intake observed in our cohort is encouraging, it may reflect self-report bias or health-conscious volunteer bias. Nonetheless, the findings suggest that some DASH-consistent dietary habits may already be present in this community and could serve as a foundation for further nutrition interventions.36 -38 Recent evidence supports the feasibility of such community-embedded approaches: an 8-week peer (dyadic) support intervention among older African American women with hypertension led to improved DASH diet adherence and a significant 4-mmHg reduction in systolic blood pressure. 38 These results underscore that even modest, particularly those emphasizing social accountability and peer encouragement, can enhance DASH adherence and blood pressure control in populations facing structural and cultural barriers to healthy eating. Integrating peer support with nutrition education and home-based monitoring may therefore amplify the impact of existing DASH-consistent habits within African American communities.
Food insecurity and perceived neighborhood food quality also appear to influence dietary outcomes in this cohort. Approximately one-third (30%) of participants experienced food insecurity, yet most rated their neighborhood food environment favorably, with over 70% reporting access to high-quality produce and low-fat options. This apparent disconnect mirrors prior findings showing that perceived food access does not always align with economic or logistical ability to obtain healthy foods.35,36 In our previous analysis of older African Americans during the COVID-19 pandemic, food insecurity was significantly associated with lower total diet quality and lower fruit and whole fruit intake, while neighborhood food environment scores were not directly correlated with diet quality. 36 These results are consistent with other studies showing that African Americans living in low-resource neighborhoods often face “food mirages,” where healthy options exist geographically but remain economically or socially inaccessible due to price, safety concerns, or transportation barriers.16,17,26 Moreover, food insecurity has been linked to poor diet quality, higher sodium intake, and reduced adherence to heart-healthy dietary patterns such as DASH.26,27 These findings suggest that economic and psychosocial constraints—rather than physical proximity alone—may drive dietary limitations in underserved communities. Interventions should therefore pair community-based produce access efforts with financial and educational support to ensure sustained dietary improvement.
In addition to dietary behaviors, variation in health literacy and physical activity likely contributes to the patterns observed in this study. Approximately 80% of participants reported “good” or “very good” health literacy, suggesting that most felt confident understanding health information; however, about 8% reported “poor” or “very poor.” Individuals with lower health literacy may face challenges interpreting food labels, applying DASH dietary recommendations, or managing sodium and potassium intake effectively, which could limit hypertension control.16,26 Conversely, those with stronger health literacy skills may be better equipped to adopt and maintain healthy eating habits. Similarly, only 31% of participants met physical activity guidelines (≥150 min/week), while 69% reported insufficient activity, reflecting sedentary patterns that may further compound hypertension risk and limit the benefits of dietary interventions. 21
The observed dietary patterns suggest structural and behavioral barriers to DASH adherence. Factors such as food cost, lack of education, nutrition label literacy, taste preferences, time constraints, and caregiving demands likely constrain dietary choices. 39 Recent qualitative evidence by Tyson et al 40 found that while Black adults with chronic kidney disease viewed the DASH diet as culturally compatible, reporting that many traditional foods already align with DASH principles, they still faced key barriers to adherence, including limited cooking skills, lack of knowledge about serving sizes, unsupportive family environments, and the high cost of healthy foods. Importantly, participants emphasized that “Black diets are not uniform,” suggesting that individualized, person-centered approaches to dietary counseling might be more effective than generalized cultural assumptions. Evidence from culturally adapted DASH interventions in similar populations shows measurable benefits: a senior-center–based DASH-aligned meal program serving low-income, racially diverse older adults reduced systolic blood pressure by 4.4 mmHg at 1 month and increased the proportion with controlled blood pressure by 15.7%, while a church-based intervention among African American adults increased fruit and vegetable intake by 0.7 to 1.4 servings/day at 6 months.38,40 Together, these findings underscore the need for tailored, resource-sensitive interventions that address both financial and household-level barriers to implementing DASH recommendations. While DASH nutrition education has been shown to improve diet quality and lower blood pressure.8,40 -42 Provider-level challenges, such as limited consultation time, low reimbursement for nutrition counseling, and inconsistent referral pathways to dietitians or community-based programs, may further reduce opportunities for patients to receive practical and culturally relevant dietary guidance. 42
These findings underscore that improving hypertension outcomes requires addressing multiple behavioral and educational determinants simultaneously. Enhancing health literacy may empower individuals to make informed dietary choices, while promoting physical activity can reinforce cardiovascular benefits and support weight and blood pressure management. Both factors interact closely with diet quality and should be integrated into comprehensive, culturally responsive interventions targeting hypertension reduction among older African Americans.
Overall, these findings underscore the need for multi-level strategies to improve dietary quality in African American older adults. Importantly, interventions should extend beyond traditional nutrition education to approaches that are culturally tailored, community-embedded, and structurally enabling. While sodium reduction for hypertensive patients should be prioritized given the significant intake disparities observed, multi-level strategies remain necessary to address overall diet quality among older African Americans.
Culturally relevant DASH-target education delivered through trusted community venues such as churches, senior centers, and barbershop or beauty shop health initiatives have been successful.43 -46 Replication of similar interventions could provide practical demonstrations, including taste-tested lower-sodium versions of familiar dishes, budget-friendly food swaps, and label-reading practice. For example, a feasibility trial by Groves and Browning 38 demonstrated that an 8-week peer support intervention among older African American women led to trends toward improved DASH diet adherence and lowered systolic blood pressure. Though the changes were modest, the high retention and participant satisfaction indicated that such community-driven approaches are acceptable and can be built upon. Community Health Workers and peer mentors have also successfully reinforced similar intervention efforts by delivering brief, repeated counseling sessions, paired with home blood pressure monitoring and simple sodium-tracking goals.12,40
At the clinical level, motivational interviewing in primary care, combined with digital supports such as text message or app-based nudges, could promote healthier grocery choices and reinforce adherence. Structural strategies, including produce prescriptions, food boxes, and partnerships with local grocers to increase the availability of low-sodium staples, have been shown to reduce access barriers in similar populations.47 -49 Mapping and addressing food-environment gaps will be essential to ensure sustained change.
Provider-led supports have also shown promise.50 -53 Streamlined counseling scripts, electronic medical record prompts, referrals to registered dietitians, and group visits may help integrate dietary counseling into routine care without displacing other priorities. Aligning team-based care models to ensure that sodium counseling is not “squeezed out” of brief encounters can further strengthen impact.
Overall, our study underlines that improving diet quality for older African Americans will require a comprehensive, community-engaged approach. By addressing the intertwined cultural, educational, and socioeconomic barriers to healthy eating, such interventions have the potential to reduce hypertension disparities and promote healthier aging in this vulnerable population.
Strengths and Limitations
This study offers valuable insight into the diet quality and DASH adherence of older African American adults in a real-world, underserved community setting. Strengths include the use of a validated dietary assessment tool, structured comparison to DASH nutrient targets, and attention to differences by hypertension status. The inclusion of Healthy Eating Index scoring allowed for a comprehensive assessment of overall diet quality, not just individual nutrients.
Limitations include the cross-sectional design, which precludes causal inference, and reliance on self-reported dietary intake, which is subject to recall and desirability bias. The relatively high reported fruit and vegetable intake may reflect such bias or the selection of health-conscious volunteers. The sample was drawn from a single urban community and may not be representative of all African American older adults. Additionally, hypertension status was self-reported, and blood pressure was not objectively measured, which may have introduced misclassification bias. However, the most common contributor to misclassification would be if participants were unaware of their status; since part of our aim was to determine if individuals adhered to the recommended diet for their status, their knowledge of their status is a relevant metric. Finally, the sample size was modest (n = 100), and while adequate for descriptive comparisons, it may have lacked power to detect small group differences in nutrient intake.
Future studies should consider objective dietary biomarkers, longitudinal designs, and intervention trials aimed at improving specific DASH components that remain deficient in this population.
Footnotes
Abbreviation
CDU: Charles R. Drew University of Medicine and Science
Ethical Considerations
The Institutional Review Board of Charles R. Drew University of Medicine and Science approved this study (IRB #1776688) on June 28, 2021.
Consent to Participate
Respondents gave written consent for review and signature before starting interviews.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by the AXIS Center (NIMHD/NIH U54MD007598 and S21 MD000103) and the CRECD Program (NIMHD/NIH R25MD007610) at Charles R. Drew University of Medicine and Science.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data sets used and analyzed in the current study are available from the corresponding author for collaborative studies.