
Abstract
Introduction:
Youth e-cigarette use remains a substantial public health concern in West Virginia. West Virginia’s Clear Future launched in 2023 to deliver the CATCH My Breath (CMB) vaping-prevention curriculum statewide in middle school grades 5 to 8. This evaluation assessed the first 2 years of implementation, including reach, student outcomes, and implementation lessons.
Methods:
A single-group, repeated cross-sectional pre-post evaluation was conducted among students in grades 5 to 8 during the 2023 to 2024 and 2024 to 2025 school years. Anonymous, unlinked surveys were administered before and after the 4-lesson CMB course to measure vaping-related knowledge, refusal intentions, susceptibility among never-users, ever use, and 30-day use. Evaluation was approved by the West Virginia University Institutional Review Board (Protocol 2406984259).
Results:
Across 2 years, 13 734 students participated in 94 schools across 39 counties. By Year 2, at least 1 trained educator was present in all 55 counties. Student acceptability was high (learned a lot, 87.9%; less likely to vape, 85.5%; confident in refusal skills, 82.1%). Knowledge improved: recognition that e-liquid is not mostly water increased in both years (Year 1: 41.3%-62.4%; Year 2: 36.1%-65.5%; P < .001). Among never-users, susceptibility declined in grade 8 (Year 1) and increased in grade 5 (Year 2); other grades showed no significant change. Ever-use and 30-day use showed no significant pre–post change.
Conclusions:
Statewide CMB implementation produced substantial knowledge gains, high student acceptability, and full county coverage by Year 2. Teacher feedback noted barriers related to time, technology access, and pacing, highlighting the need for offline-ready delivery and age-tailored content.
Keywords
Introduction
Since 2014, e-cigarettes have been the most commonly used tobacco product among U.S. middle and high school students. 1 In 2024, current use was 5.9% overall (7.8% among high school students; 3.5% among middle school students). 1 Among current users, 26.3% reported daily use; disposable (pre-filled, single-use) devices predominated (55.6%); and 87.6% reported flavored products. 2 Although prevalence declined from 2023, these levels remain a substantial public health concern. 1
Nicotine exposure during adolescence can disrupt brain development and increase the likelihood of addiction.3,4 During this developmental period, nicotine affects synaptic plasticity and is associated with alterations in the prefrontal cortex and other brain regions involved in executive function and impulse control.3,5-7 Adolescents who use e-cigarettes also report symptoms of nicotine dependence, including cravings and loss of control, often shortly after initiation.8,9 In addition to nicotine, e-cigarette aerosols can contain components with known or suspected toxicity, raising concerns about longer-term health effects with sustained use.3,4 Although complete substitution for cigarettes reduces toxicant exposure for adults who smoke, youth e-cigarette use is associated with an increased likelihood of subsequent experimentation with and use of combustible cigarettes.4,10 These risks underscore the importance of prevention approaches that address vaping-related knowledge, perceived norms, and refusal skills. 11
The burden of youth e-cigarette use is especially high in Appalachia and in West Virginia. Regional studies describe relatively low perceived harm from e-cigarettes and report that about 23.4% of Appalachian youth have ever used e-cigarettes. Lower perceived harm is linked to higher odds of both use and susceptibility.12,13 In West Virginia, current e-cigarette use among high school students reached 35.7% in 2019, including 16.7% reporting frequent use, and although it declined, it was still 27.5% in 2021.14,15
School-based prevention remains a key strategy for addressing youth vaping. A 2024 meta-analysis found that school-based e-cigarette prevention programs produce short-term improvements in knowledge, attitudes, and intentions, though effects on behavior were mixed and the overall certainty of evidence was low to moderate. 16 These findings support continued, structured delivery at scale with continued evaluation. CATCH My Breath (CMB) is a skills-focused vaping prevention curriculum that addresses knowledge, social norms, and refusal skills. It was selected for statewide implementation in West Virginia based on its theory-driven design, scalability for school settings, and prior evidence of feasibility and early effectiveness, including implementation in Central Appalachia.11,17,18
In August 2023, the West Virginia Department of Health and the West Virginia Department of Education launched West Virginia’s Clear Future: Don’t Let Vaping Cloud It to deliver CMB statewide in grades 5 to 8. 19 This manuscript reports on the initiative’s first 2 years, including statewide reach, trained teacher readiness and coverage, student outcomes, and teacher-reported implementation experiences. This initiative was implemented through the Appalachian Pulmonary Health Project and the American Lung Association of West Virginia, and the evaluation was conducted by the West Virginia Alliance for Creative Health Solutions, Inc.
Methods
CMB is an evidence-based, 4-lesson vaping prevention curriculum delivered by trained classroom teachers. Classroom teachers completed standardized CMB training prior to implementation and delivered the curriculum during regular class periods during the academic year, with schools determining scheduling within existing class structures. Each lesson was designed to fit within a standard class period (approximately 45 min), though pacing varied by classroom and grade level. The curriculum uses youth-centered video content and social norms messaging to address knowledge about vaping, perceived norms around use, and refusal skills. CMB is grounded in Social Cognitive Theory, which emphasizes the role of knowledge, perceived norms, self-efficacy, and skill-building in shaping health behavior and is widely recommended as a framework for health promotion interventions.20,21 Video and instructional materials are part of the CMB curriculum developed by the CATCH Global Foundation and are available through the CATCH Global Foundation website. 22 The curriculum structure and classroom delivery approach are consistent with prior descriptions of CMB implementation reported in U.S. and international settings.23,24 Classroom delivery sessions were not recorded as part of this evaluation. In West Virginia, CMB is the core educational component of West Virginia’s Clear Future: Don’t Let Vaping Cloud It.
A single-group, repeated cross-sectional pre-post evaluation was conducted among students in grades 5 to 8 during the 2023 to 2024 (Year 1) and 2024 to 2025 (Year 2) school years. In some participating schools, CMB delivery occurred alongside existing school-based health center (SBHC) services or partnerships. Engagement with SBHCs varied by school and was not standardized as part of the intervention; where present, SBHC staff could reinforce curriculum delivery.
Teachers who delivered CMB were invited to complete brief post-implementation evaluations following curriculum delivery. Teacher feedback was collected using open-ended survey items that solicited comments on strengths of delivery, challenges encountered, and suggestions for improvement. Responses were submitted electronically and were not linked to individual teachers or classrooms. Open-ended responses were reviewed and grouped into thematic categories to summarize common implementation experiences across schools and years.
Student surveys were administered before the first lesson (pre) and after the fourth lesson (post). Responses were anonymous and were not linkable at the individual level; analyses used available cases at each time point. Because surveys were anonymous and no identifiers were collected, students could not be de-duplicated within or across years. Counts of “students” and “reach’ therefore refer to unique survey records (course deliveries) rather than confirmed unique individuals, consistent with the repeated cross-sectional design.
Survey measures included vaping-related knowledge (eg, whether nicotine is harmful and whether e-liquid primarily contains water), refusal-related beliefs, behavioral intentions (response to a best friend’s offer to vape and intention to vape in the next year), susceptibility among never-users, ever use, and past 30-day use. Student and teacher survey items were adapted from instruments developed by the CATCH Global Foundation for CMB. 22 Teachers also completed brief evaluations describing delivery strengths and barriers. Teacher feedback was collected as open-ended text responses. Comments were grouped into themes using a structured content coding process. The counts in Table 7 reflect how many comments were assigned to each theme.
Descriptive statistics summarized pre- and post-survey responses by implementation year. Analyses were conducted separately by year to reflect differences in participating schools, grade distributions, and timing of implementation across academic years. The unit of analysis was the individual survey response. Because surveys were anonymous and unlinked, pre- and post-survey responses could not be matched at the individual level. Analyses therefore compared aggregate pre- and post-instruction proportions using available cases at each time point, consistent with a repeated cross-sectional design. No imputation was performed for missing responses; denominators for each analysis reflect the number of students who answered the specific item at that time point. Pre-post differences in categorical outcomes, including vaping-related knowledge items, refusal intentions, susceptibility, ever use, and past 30-day use, were assessed using Pearson chi-square tests. All tests were 2-tailed, with statistical significance defined as P < .05. Effect sizes were not calculated because the evaluation focused on direction and consistency of overall change rather than individual-level effects. Susceptibility among never-users was examined by grade level within each year to assess variation across early and later middle school grades. Analyses did not account for clustering within schools or classrooms because surveys were anonymous and unlinked, and the evaluation focused on overall statewide implementation rather than school-level effects. Analyses were conducted in JMP Pro, version 18. No identifiable data were collected. All survey instruments are provided for reference in Appendices A to C. The evaluation was approved by the West Virginia University Institutional Review Board (Protocol #2406984259).
Results
West Virginia’s Clear Future expanded rapidly across 2 years. In Year 1, 4596 student survey responses were collected across 32 schools in 22 counties, and 91.0% of students completing the pre-survey also completed the post-survey. By Year 2, reach increased to 9138 student survey responses across 72 schools in 31 counties, with 82.5% of pre-survey respondents completing the post-survey. By the end of Year 2, at least 1 trained teacher was present in all 55 counties (Table 1).
Program Reach, Participating Schools, and Survey Completion Across 2 Years of West Virginia’s Clear Future, School Years 2023 to 2024 and 2024 to 2025.

Across 2 years, the program reached 13 734 students in 94 unique schools spanning 39 counties, with post-survey completion of 91.0% in Year 1 and 82.5% in Year 2.
Knowledge improved consistently across both years (Table 2). The proportion of students correctly identifying that water is not a main part of e-liquid rose from 41.3% to 62.4% in Year 1 and from 36.1% to 65.5% in Year 2 (both P < .001). Knowledge that nicotine is addictive and harmful and that vaping is illegal for those under age 18 also increased.
Knowledge Outcomes Before and After CATCH My Breath Curriculum, School Years 2023 to 2024 and 2024 to 2025.
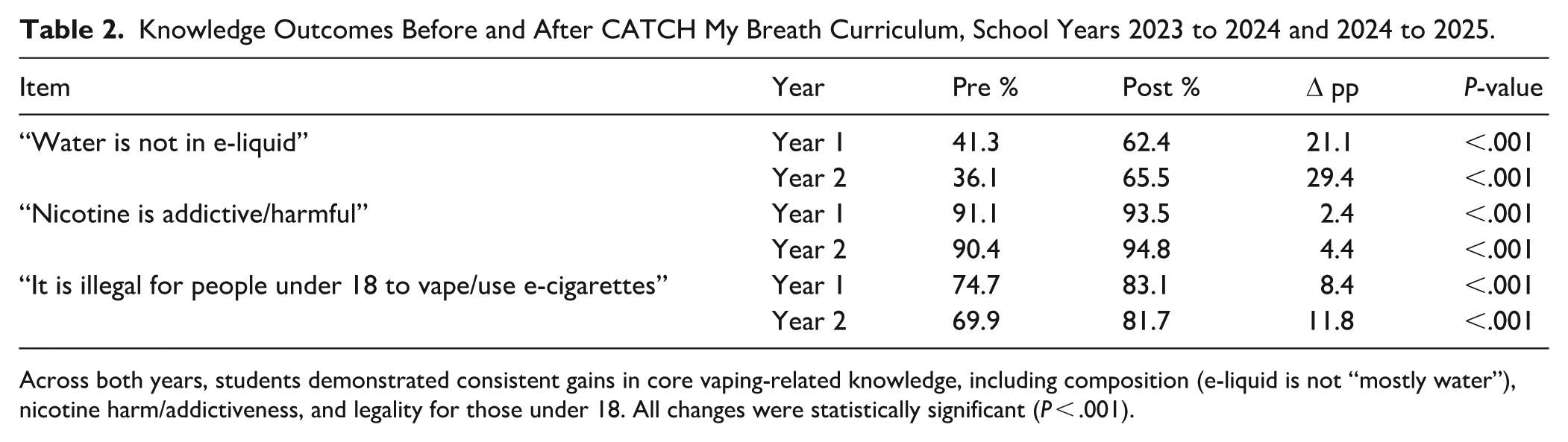
Across both years, students demonstrated consistent gains in core vaping-related knowledge, including composition (e-liquid is not “mostly water”), nicotine harm/addictiveness, and legality for those under 18. All changes were statistically significant (P < .001).
Refusal intentions remained high (Table 3). In Year 1, the proportion of students who responded that they would “definitely not” use a vape offered by their best friend increased from 71.9% to 73.9% (P = .040). In Year 2, this measure was stable, from 73.4% to 73.0% (P = .513). In addition, in Year 2, intention to vape “next year” shifted modestly; “definitely not” decreased from 77.0% to 74.7%, “probably not” increased from 18.5% to 20.7%, and endorsement of any “yes” response remained approximately 4.6% (P = .0004; Table 3).
Refusal Intentions Before and After CATCH My Breath Curriculum, School Years 2023 to 2024 and 2024 to 2025.

Refusal intentions toward a direct peer offer remained high. In Year 1, “definitely not” increased by 2.0 percentage points (P = .040). In Year 2, levels were stable (P = .513). In Year 2, intention to vape “next year” also shifted modestly.
Among never-users, susceptibility to future vaping showed grade-specific patterns (Table 4). In Year 1, susceptibility declined for eighth graders (40.40%-35.25%; P = .017). In Year 2, susceptibility increased for fifth graders (42.90%-48.80%; P = .026). All other grade-year changes were small and not statistically significant (Year 1: grades 5-7; Year 2: grades 6-8; Table 4).
Susceptibility to Future Vaping Among Never-users, by Grade.
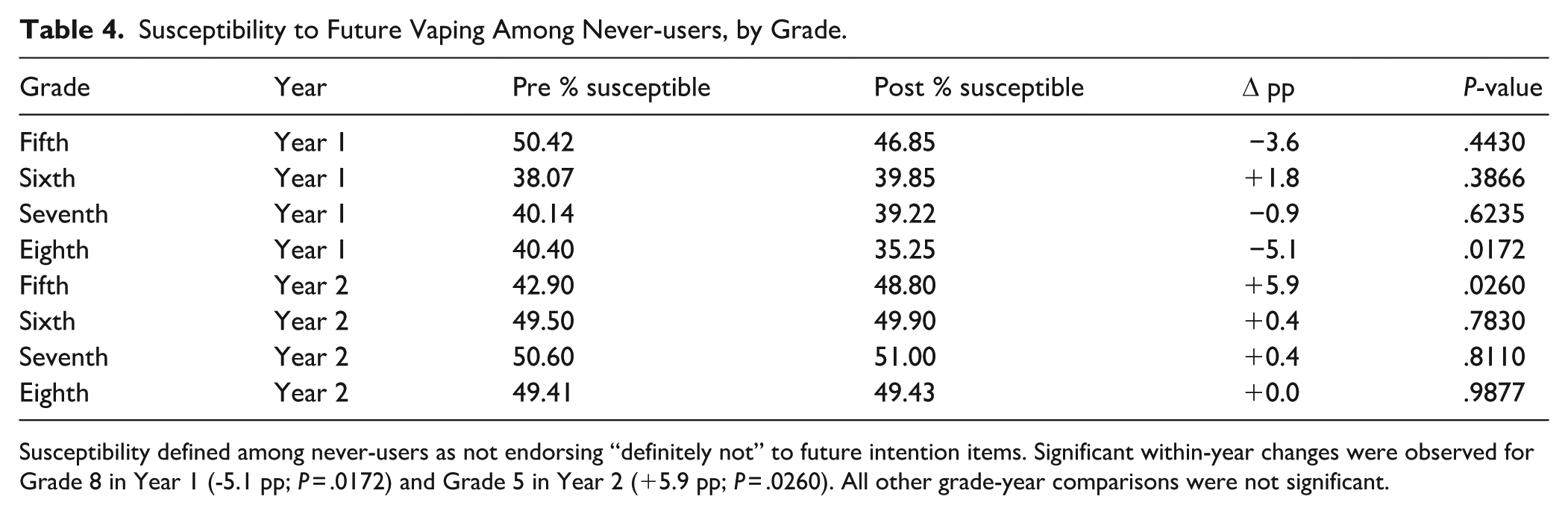
Susceptibility defined among never-users as not endorsing “definitely not” to future intention items. Significant within-year changes were observed for Grade 8 in Year 1 (-5.1 pp; P = .0172) and Grade 5 in Year 2 (+5.9 pp; P = .0260). All other grade-year comparisons were not significant.
Self-reported vaping behavior showed no statistically significant short-term change across either year (Table 5). In Year 1, ever-use was 15.3% at pre-survey and 14.5% at post-survey (P = .111), and past 30-day use was 4.5% and 4.4%, respectively (P = .842). In Year 2, ever-use was 14.6% at pre-survey and 15.2% at post-survey, and past 30-day use was 4.0% at both time points; these Year 2 differences were not statistically significant (P > .05). The absence of statistically significant pre-post change in reported behavior is consistent with expectations for a brief prevention curriculum and indicates that there was no statistically significant increase in vaping alongside the gains in knowledge and refusal intentions (Table 5).
Self-reported Vaping Behavior Before and After CATCH My Breath Curriculum, School Years 2023 to 2024 and 2024 to 2025.

“Ever-use” refers to any lifetime vaping/e-cigarette use. “30-day use” refers to any self-reported vaping in the past 30 days. No statistically significant pre–post differences were observed in either year.
Student perceptions of the curriculum, collected on post-surveys, were consistently positive (Table 6). In Year 1, 87.7% of students agreed that they “learned a lot about e-cigarettes,” and 86.8% agreed that they were “less likely to vape now”; these levels were similar in Year 2 (87.9% and 85.5%, respectively). Confidence in using a refusal skill remained stable at 82.1% in both years. Nearly 9 in 10 students agreed that “all middle and high school kids should go through the CATCH My Breath program” (89.9% in Year 1; 89.7% in Year 2), indicating sustained acceptability of program content and delivery.
Student Perceptions of CATCH My Breath (CMB), School Years 2023 to 2024 and 2024 to 2025.

Values represent the percent of students who agreed or strongly agreed on the post-survey. Perceived learning, reduced likelihood to vape, refusal skill confidence, and endorsement that CMB should be offered to all students were all high and stable across both years.
Teacher feedback from open-ended comments highlighted both strengths and implementation challenges (Table 7). Analysis included 197 evaluations in Year 1 and 206 in Year 2. Themes were consistent across years: high student engagement; usefulness of media-literacy content and refusal-skills practice; and constraints related to time and classroom technology. Teachers cited strong engagement with interactive activities, media-literacy components, refusal-skill practice, and classroom video segments (33 mentions in Year 1; 48 in Year 2), and specifically referenced advertising/media-literacy elements as effective (25 mentions in each year). Teachers also noted that students were often surprised by factual content such as “e-cigarette vapor is not mostly water.”
Teacher-reported Strengths and Implementation Challenges, West Virginia’s Clear Future (WVCF), School Years 2023 to 2024 and 2024 to 2025.

Teachers in both years described strong student engagement and endorsed the curriculum’s use of interactive media, refusal-skill practice, and industry/advertising awareness. They also identified recurring delivery barriers, including limited instructional time and technology access. By Year 2, as more schools repeated the program, teachers more frequently noted perceived repetition for students and asked for refinements such as more interactivity, locally relevant data, and pacing adjustments to fit different grades and classroom schedules.
Teachers in both years also described recurring barriers to delivery. Time and scheduling demands were cited frequently (41 mentions in Year 1; 24 in Year 2), and technology issues (eg, streaming video or accessing slides) were also common (12 mentions in Year 1; 29 in Year 2). Teachers reported needing more support with materials and preparation in Year 1 (10 mentions) and again in Year 2 (12 mentions, including requests for easier access, printed backups, and clearer pacing guidance). These requests were commonly framed in relation to practical classroom constraints, including limited instructional time and variable technology access. By Year 2, some teachers additionally noted 2 scale-up challenges: repetition for students who had seen similar content in prior years (17 mentions), and the need to tailor delivery with more interactivity, more locally relevant data, and more age-appropriate pacing (35 total suggestions). Teacher feedback points to practical supports for scale-up: locally accessible (downloadable) videos and slide decks with printed backups to avoid streaming issues, protected instructional time to complete all lessons, and grade-specific pacing and engagement adjustments, particularly for younger grades (Table 7).
Discussion and Conclusions
West Virginia’s Clear Future scaled CMB rapidly across the state, nearly doubling student reach from Year 1 to Year 2 and engaging 94 unique schools across 39 counties over 2 years, with at least 1 trained educator present in all 55 counties by the end of Year 2. This pattern of growth in a largely rural, high-burden context demonstrates that a standardized, school-delivered vaping-prevention curriculum can be implemented at broad scale through a coordinated health education partnership. These results indicate that integrating a standardized vaping-prevention curriculum into routine middle-grade instruction at statewide scale is feasible, although additional expansion is needed to reach all eligible students. CMB sustainability is supported through the development of statewide delivery capacity, enabling schools to deliver CMB locally without reliance on external facilitators. In addition to feasibility, the evaluation demonstrated consistent improvements in student knowledge and vaping-related intentions, alongside high student acceptability, and strong teacher endorsement of the curriculum’s content and classroom delivery process. These findings indicate that CMB can be implemented at statewide scale and is positively received by students and teachers.
Knowledge gains were consistent across both years on core content areas, including components of e-cigarette aerosol, the addictiveness and risks of nicotine, and the illegality of youth vaping. These topics map directly onto common misperceptions and to commercial marketing tactics. Teachers also described media and advertising content as especially influential. This is important because inaccurate beliefs (eg, that vapor is “mostly water” or that vaping is not addictive) are associated with higher odds of ever-use and susceptibility in Appalachian youth.12,13 These findings align with broader evidence that school-based nicotine prevention can shift knowledge, perceived harm, and refusal-related beliefs even when short-term behavioral change is limited. 16
Behavioral intentions and refusal-related confidence also remained high. The proportion of students who said they would “definitely not” use a vape offered by a best friend increased modestly in Year 1 and remained stable in Year 2, and most students reported feeling confident using a refusal skill and being less likely to vape after the program. These patterns suggest that the curriculum supports refusal self-efficacy and protective norms around peer offers, both of which are meaningful precursors to behavior in early adolescence. 25
Susceptibility patterns were mixed and should be interpreted cautiously. Among never-users, susceptibility decreased for older students (eighth grade in Year 1) and increased for the youngest students (fifth grade in Year 2), while grades 6 and 7 showed little change. Because surveys were anonymous and unlinked and administered immediately post-instruction, these shifts may reflect timing and awareness effects as much as true risk. The practical next step is already underway: Year 3 will continue routine susceptibility measurement across middle grades. Tracking the same indicators under steady procedures will show whether the fifth-grade increase persists, resolves, or varies by cohort, and will inform whether additional adjustments to delivery for younger students are warranted.
Self-reported ever-use and past 30-day use of e-cigarettes did not change significantly from pre- to post-survey in either year. This stability is informative for 2 reasons. First, it indicates that there was no short-term increase in reported vaping associated with curriculum delivery. Second, it is consistent with expectations for a brief, 4-lesson prevention curriculum delivered over a short instructional window. Durable behavioral change generally requires longer follow-up and/or more intensive intervention. 26 In the context of a state with high prevalence of youth e-cigarette use, stabilizing reported use while improving knowledge and refusal-related beliefs indicates substantial progress.
Teacher feedback from open-ended classroom evaluations suggested strengths and challenges (Table 7). Many teachers described high student engagement, especially with media-literacy content, industry/advertising messages, refusal-skill practice, and video segments that felt current. Teachers received the standard CMB curriculum materials as part of implementation, and feedback helped identify where additional support could make classroom delivery easier. Reported challenges included limited instructional time and occasional technology barriers (e.g., streaming video or accessing slides). In Year 2, teachers more often asked for ready-to-use materials, such as printed backups and offline media, and noted that some students had seen similar content before. Several also emphasized that repetition can help when lessons stay interactive and hands-on, keeping students engaged and deepening learning. Accordingly, remarks about repetition are treated as observations that can guide practical refinements, not as evidence that repeating content is a problem.
The statewide implementation of CMB required coordinated effort across West Virginia’s Clear Future partners and ongoing formative evaluation to support success. Partners met weekly by video conference (and continue to meet) to monitor progress, identify implementation challenges, and respond with updated tools and procedures. Lessons learned, tools developed, and weekly meeting minutes were maintained in a shared Google Drive accessible to partners and field coordinators. Tools supporting recruitment, training, implementation, and evaluation were developed, deployed, and refined iteratively based on field experience. A list of West Virginia’s Clear Future tools is provided in Appendix D.
This evaluation has limitations. The design was a single-group, repeated cross-sectional pre-post model with no comparison group. Surveys were anonymous and unlinked at the individual level, so change cannot be attributed to individual students. All outcomes were self-reported. In addition, susceptibility results by grade reflect grade-level snapshots (eg, fifth grade in Year 2 and eighth grade in Year 1), not a tracked cohort over time, and should be interpreted as patterns by grade rather than longitudinal change. Local delivery conditions (including pacing, emphasis, and workarounds for technology) varied by classroom and may differ from the intended model. Finally, the legality survey item used the program’s standard wording (“under 18”); federal minimum sales age is 21.
At the time of writing, funding for public health tobacco prevention and cessation efforts is being reduced at federal and state levels. Funding for West Virginia’s Clear Future is currently secured through the 2025 to 2026 school year. In response to the evolving policy and funding environment, partners have developed a sustainability and resiliency plan to continue CMB delivery as broadly as possible across the state. Recent randomized controlled trial findings for CMB have also been presented, further supporting the program’s evidence base. 27 A key asset supporting sustainability is the established workforce of 377 CMB-certified teachers, counselors, and community advocates distributed across all 55 counties, including 125 individuals who have delivered the curriculum at least once. Core program staff will continue to provide communication, technical assistance, and access to updated resources. In addition, “teacher champions” – defined as educators who have delivered the curriculum across multiple school years – will be identified and prioritized for linkage with available local private and governmental funding opportunities. Partner organizations, including the American Lung Association, Partners in Health Network, and the West Virginia Alliance for Creative Health Solutions, Inc., have demonstrated capacity to secure and manage these funds and will continue to support local implementation efforts. These strategies position West Virginia’s Clear Future to maintain and adapt statewide vaping prevention efforts.
This 2-year evaluation supports 3 conclusions for statewide prevention policy. First, CMB can be delivered at scale through coordinated state partnership with schools and organizations. Second, consistent knowledge gains, generally high and stable refusal intentions, and positive student perceptions indicate student-level value in this early phase of implementation. Third, recurring teacher feedback provides a roadmap for sustainability: support schools with protected instructional time; provide offline or low-tech delivery options; refresh West Virginia-specific data to maintain relevance; and tailor pacing and framing for younger grades. These findings indicate that West Virginia’s Clear Future has established an operational statewide platform for vaping prevention in a high-need setting.
Footnotes
Appendix
West Virginia’s Clear Future Partner Tools.

| Category | Tool/resource | Format | Purpose/notes |
|---|---|---|---|
| Recruitment and Training | West Virginia’s Clear Future Toolkit. Aug. 2023 | Toolkit | Core program overview and implementation supports. |
| Call to Action one-pager for certified health teachers. Apr. 2025 | Document | Recruitment and engagement for trained teachers. | |
| Master contact list for CMB-certified teachers | Spreadsheet | Contact tracking and outreach coordination. | |
| Field coordinators list and contact information | Spreadsheet | Points of contact for school support and troubleshooting. | |
| Teacher training video: evaluation procedures and required quiz | MP4; Google Form | Standardizes evaluation procedures; quiz documents completion. | |
| CMB training certificates (2-h) | PDF records | Documentation of training completion. | |
| Implementation | Step-by-step teacher instructions | Document | Quick-start guide; links to CMB site, evaluation tools, W-9, and field coordinator contacts. |
| Teacher/school stipend checklist | Document | Standardizes steps required for stipend eligibility and processing. | |
| Weekly partner meeting minutes (videoconference) | Document | Tracks decisions, lessons learned, and action items. | |
| Weekly dashboard reports of implementation progress | Presentation slides from Tableau-based dashboard | Monitors reach and delivery status; supports ongoing implementation management and evaluation tracking. | |
| Teacher/school payment tracking sheets | Spreadsheet | Tracks stipend processing and payment status. | |
| Evaluation | Anonymous student pre- and post-surveys | Online Qualtrics surveys | Standardized student outcome measurement (pre/post). |
| Teacher classroom evaluation form | Online Qualtrics survey | Captures delivery strengths, barriers, and improvement suggestions. |
Acknowledgements
The authors acknowledge the contributions of classroom teachers, school administrators, and students who participated in the delivery and evaluation of the CATCH My Breath curriculum across West Virginia. The authors thank state and community partners who supported implementation, coordination, and training activities associated with West Virginia’s Clear Future initiative. The authors also thank the Claude Worthington Benedum Foundation, the Greater Kanawha Valley Foundation, the Logan Healthcare Foundation, the Pallottine Foundation of Buckhannon, the Pallottine Foundation of Huntington, the Sisters of St. Joseph Health and Wellness Foundation (Wheeling), and the West Virginia Department of Health for their leadership, support, and encouragement throughout this initiative.
Author Note
No third-party writing or editorial assistance was used in the preparation of this manuscript.
Ethical Considerations
This evaluation was reviewed and approved by the West Virginia University Institutional Review Board and determined to qualify as Not Human Subjects Research under the Flex review process (Protocol #2406984259).
Consent to Participate
Informed consent requirements were waived because the evaluation involved anonymous survey data collected as part of routine classroom-based educational programming. Participation was voluntary, and students could skip any survey question.
Consent for Publication
Not applicable. No identifiable individual data, images, or recordings were included.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported through funding and support from the Claude Worthington Benedum Foundation, the Greater Kanawha Valley Foundation, the Logan Healthcare Foundation, the Pallottine Foundation of Buckhannon, the Pallottine Foundation of Huntington, and the Sisters of St. Joseph Health and Wellness Foundation (Wheeling).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
De-identified data supporting the findings of this study are available from the corresponding author* upon reasonable request, subject to applicable data use agreements and approvals.