
Abstract
Introduction:
Chicago, Illinois is one of the most diverse cities in the United States. Yet, its history is fraught with inequities which pervade every pillar of its modern infrastructure, from housing and education to healthcare. Established healthcare institutions, like Rush University Medical Center (RUMC), are uniquely positioned to combat historically ingrained disparities. Their physical presence, economic influence, and associated medical schools provide the opportunity and resources to support sustainable health equity strategies such as the Cardiometabolic Health Initiative (CHI).
Methods and Results:
CHI is a health equity initiative founded by Rush Medical College (RMC) students. Its mission is to provide comprehensive cardiometabolic screenings directly to West Chicago residents. Partnering with RUMC, CHI leverages its medical school cohort as well as the medical center’s resources to provide preventative care to those in need. Since its inception, CHI has screened over 300 West Chicago patients. The preliminary results emphasize the disproportionate prevalence of cardiometabolic disease in this population, and underscore the need for health equity organizations like CHI.
Conclusion:
The health inequity seen across Chicago is not unique. The same patterns of cardiometabolic disease are mirrored across American cities. CHI serves as an innovative blueprint for addressing urban health inequity. By harnessing the resources of established health systems and their affiliated medical schools, student-run initiatives, like CHI, can improve urban health nationwide.
Keywords
Introduction
A City’s Troubled Past
Chicago, Illinois is the third largest city in the United States and one of the country’s most diverse metropolitan areas. 1 Yet, hidden behind its diverse population is a history fraught with disparities. These inequities are tied to the historical origins of the city, and were further exacerbated by The Great Migration of the 20th century, which marked an influx of Black families to Chicago from southern cities. This demographic shift sparked countless racist practices, including redlining, predatory housing contracts, and blockbusting, plundering resources from growing minority neighborhoods. 2 Today, decades later, years of disenfranchisement, racial violence, and pointed resource depletion has led to deep-seated structural racism impacting Chicago’s infrastructure.
This systemic inequality has created profound disparities in access to housing, food, education, and healthcare, resulting in a dramatic, racially driven life expectancy gap across the city. In Chicago’s affluent “Loop” neighborhood, the life expectancy is 80 years old, over two years above the national average. Yet, just 5 miles west in East Garfield Park, a predominantly Black neighborhood on the West Side of Chicago, life expectancy drops to 66 years of age. 3 These neighborhoods, while close in proximity, differ dramatically in life expectancy, mirroring the life expectancy gap between the United States and most developing countries. 4 While the factors driving this discrepancy are nuanced and often interconnected, cardiovascular disease (CVD) remains the number 1 cause of death and disproportionally affects the disenfranchised populations on the West and South sides of Chicago. 3
Community-Based Health Equity Strategies
Healthcare institutions, particularly those in urban and resource depleted neighborhoods, are uniquely positioned to address the complex inequalities driving the gap in health outcomes across cities. Their physical, economic, and political influence provides the capacity to combat widespread medical mistrust, barriers to care, and engrained community disenfranchisement. Rush University Medical Center (RUMC) recognizes this responsibility, and over the last decade, has dedicated itself to improving health equity throughout its catchment area and greater Chicago.
In 2016, RUMC performed a Community Health Needs Assessment which exposed a vast life expectancy gap in the hospital system’s diverse patient population. 3 Patients from Black and brown communities were dying at disproportionately higher rates from preventable chronic conditions due to lack of access to care. These findings inspired RUMC to develop an innovative health equity strategy focused on “outstanding patient care, education, research, and community partnerships.” 5 This health equity mission pervades every facet of RUMC’s operation and expands beyond the confines of the hospital walls. These health-equity-based values are embedded in the educational experience at RUMC’s associated medical college.
Rush Medical College (RMC) actively cultivates a diverse and inclusive educational environment that reflects the population it serves. The institution supports underrepresented students in medicine through mentorship and networking. The medical school curriculum features longitudinal course work focused on health inequities, patient centered care, and social determinants of health. RMC develops “empathic physician leaders dedicated to innovation, research and health equity” with service at the core of its mission. 6 With over 36 student led Rush Community Service Initiative Programs, over 90% of RMC students volunteer within the Chicago community. This system-wide commitment to health equity defines RUMC’s approach, both in the clinical space and the classroom.
Methodology
Student-Directed Health Equity Initiatives: The Cardiometabolic Health Initiative (CHI)
RUMC’s institutional and educational emphasis on health equity serves as the foundation of the Cardiometabolic Health Initiative (CHI). CHI is a student-run, mobile, CVD screening program, founded in 2022 by 5 first-year medical students. Their efforts are led by Dr. Daniel Luger, a Rush trained cardiologist who specializes in CVD prevention. CHI was created as a direct response to the disproportionately high prevalence of cardiometabolic disease in the underserved communities of West Chicago. Its founding goal was to partner with trusted pillars of the West Side community to provide cardiometabolic screening directly in the neighborhoods most in need. Additionally, this fully student-operated clinic offers students hands-on patient care experience and real-world exposure to the social determinants of health.
Today, CHI is a robust prevention clinic providing free, monthly, and comprehensive CVD screenings at Beyond Hunger Food Pantry, Harmony Church, El Mercadito, and Marillac St. Vincent’s, 4 established West Chicago community organizations. The initiative is overseen by Dr. Luger and his executive medical student board and run by an interdisciplinary team of healthcare workers, including nurses, nurse practitioners, mental health providers, social workers, physicians, and over 50 healthcare students. As an official RMC community service initiative, CHI has a continuous pool of student volunteers from the medical, nursing, and physician assistant program that ensure its longevity. Financially, CHI is supported exclusively by grant funding. This grant funding supports the hiring of its diverse team of health care workers as well as the purchasing of point of care testing supplies. While there are many free, student-run clinics across the state, CHI represents a unique mobile model, fully run by students, and embedded within community food pantries rather than traditional brick-and-mortar clinics. 7
Screening Protocol
CHI provides monthly screenings at 4 community food pantries, Beyond Hunger, Harmony Church, El Mercadito, and Marilac St. Vincents. At each event, all attending community members are eligible for screening. Those interested provide consent and then navigate through a 5-station clinic. First, basic demographic information is collected, along with a focused medical history that includes prior medical conditions and current medications. Next, participants complete validated health questionnaires, providing information on their diet, exercise capacity, sleep quality, mental health, and social determinants of health. This step is followed by the collection of extensive anthropometric data: height, weight, waist circumference, neck circumference, and blood pressure. Finally, a point of care lipid panel and A1c are obtained. From this data, an Atherosclerotic Cardiovascular Disease (ASCVD) risk score is calculated, quantifying the individuals’ risk of developing atherosclerotic CVD within the next 10 years.
Finally, participants review their results with a cardiologist, lifestyle medicine specialist, and health coach. Their numbers are thoroughly explained, and their risk score is contextualized. They receive counseling on leading a healthy lifestyle, with an emphasis on social determinants of health, and the physical medicine and rehabilitation team provides tailored recommendations for physical activity that is suitable for their bodies and feasible for their living conditions. The onsite community health workers create EPIC profiles for each client and connect them with primary care providers within the RUMC health system. The mental health counselor provides real-time crisis counseling and follow-up appointments for individuals with psychosocial stressors. All clients are encouraged to enroll in the longitudinal follow-up program that includes ongoing lifestyle counseling, frequent blood pressure checks, and repeat blood work.
CHI’s growth and sustainability are – in large part – due to the ever-renewing body of medical students who keep the organization alive. Since CHI’s creation, medical students have been at the forefront of its design and execution, providing a continuous, cost-free, supply of talent and labor. Students, in the infancy of their careers, demonstrate an eagerness to volunteer their time in the community and interface with patients. Working with CHI equips students with practical skills, imbuing values of equity that will prepare these future physicians to take on the generational challenge of healthcare disparities. Over the last 2 years, CHI, led by its passionate students, has built 4 long-term and growing community partnerships on Chicago’s West Side. Through these partnerships, with both Beyond Hunger and Harmony Community Church, CHI has screened over 300 West Side community members.
Clinical Impressions
CHI’s Preliminary Findings
Since its inception, CHI has screened over 300 patients on Chicago’s West Side. The population screened is diverse, with 40.40% of the patient population identifying as Hispanic or Latino, 38.24% as Black or African American, 13.79% as White, 3.13% as Asian, and <1% as multiracial. Notably, the patients screened confirm the disproportionate prevalence of CVD risk factors within the population. Among participants at the clinic, the average blood pressure across every age group from 40 to 90 years old, is consistent with hypertension (systolic >129 or diastolic >79). Similarly, across the same age groups, the average A1c falls within the pre-diabetic range (5.7% to 6.4%). Analyzing patient ASCVD risk scores, in patients 50 and above, the average ASCVD risk score falls within the intermediate to high-risk category (intermediate: 7.5% to <19%, high-risk: >20%). Specifically, patients from 50 to 59 and 60 to 69 years of age have an intermediate average ACSVD risk score, at 6.25% and 13.53% respectively. In patients 70 to 79 and 80 to 89 years of age, the average ASCVD risk scores fall within the high-risk category, at 25.51% and 26.48% respectively. Investigating the PCP data of participating patients, only slightly more than half of the screened participants, 58.3%, report having a primary care physician, and over half of the screened participants, 54.23 %, report not taking any medications for CVD risk factors. (Full patient demographic data can be found in Table 1 and complete lab, vitals, and PCP data can be found in Table 2.)
Screened Participant’s Demographic Data and Past Medical History.

One patient included in the database did not provide any demographic information and thus was not included in this analysis.
Screened Participant’s Vitals, Labs, and PCP Data.
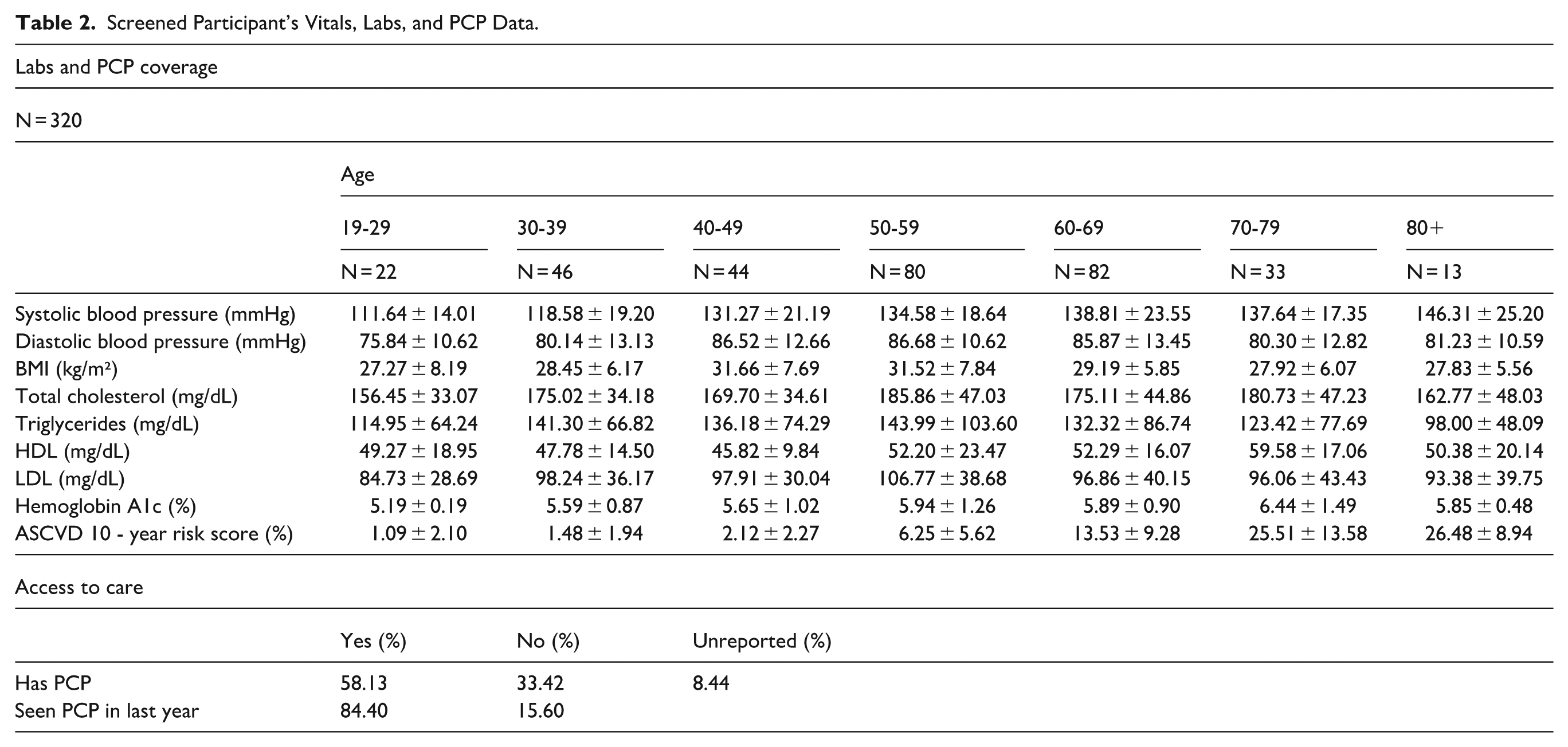
This data highlights the necessity of accessible health interventions, such as community-based organizations like CHI. CHI utilizes the resources and influence of its associated health system to address the unmet needs of its city’s residents. It empowers patients with information about their health through accessible cardiovascular screenings and it serves as a bridge to longitudinal primary care services. In doing so, it serves as a model, demonstrating to other healthcare institutions and their associated medical schools the power these community initiatives can have on their urban communities.
Conclusion
The Way Forward
Chicago is an ethnically diverse city with profound disparities in healthcare and neighborhood vitality. These inequities have deep historical roots and are ingrained in the city’s infrastructure and culture. These challenges are not unique to Chicago and are embedded in the foundation of cities across America. RUMC has established itself as an anchor institution on the West Side of Chicago, an exemplar for urban hospital systems combating local inequities. RUMC’s health equity mission informs its hiring practices, its approach to medical education, and its engagement with the community. CHI is a novel community engagement paradigm that leverages the resources of a large hospital system to empower medical students in addressing healthcare inequality. The impact of this model is twofold: CHI expands access to community-based care for underserved communities while equipping medical students with a deep understanding of the social determinants of health, encouraging lifelong engagement in community-based care.
Footnotes
Acknowledgements
The authors of this paper have no acknowledgments
Ethical Considerations
This retrospective study was approved by the institutional review board of Rush Medical Center (ORA #23020104).
Consent to Participate
The institutional review board of Rush Medical Center waived the need for informed consent given the retrospective review of data in this report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data included in this report represents clinical patient information. Thus, the data is not publicly available in order to protect patient privacy but can be reasonably requested from the corresponding author*.