
Abstract
Background:
Loneliness is increasingly recognized as a major determinant of health rather than a transient emotional experience. Extensive evidence links chronic loneliness to adverse physical and mental health outcomes and increased healthcare utilization. Despite growing policy attention, loneliness remains inconsistently identified and addressed in healthcare systems, particularly in primary care, where other social determinants of health are increasingly screened.
Objective:
This narrative synthesis aims to advance a biopsychosocial reframing of loneliness as a “vital sign” to reflect a clinically relevant, measurable, and actionable health metric that can be feasibly integrated into primary care workflows to inform whole-person care, risk stratification, and referral pathways.
Methods:
A literature search of interdisciplinary peer-reviewed manuscripts published between 2010 and 2025 across public health, psychology, gerontology, and translational health sciences. Included sources encompassed epidemiological studies, mechanistic research, and implementation science literature examining loneliness screening and integration within real-world clinical workflows.
Results:
Results are presented thematically to reflect the manuscript’s objective of reframing loneliness as a clinically actionable vital sign. Findings are organized to reflect evidence supporting loneliness as a biopsychosocial health risk; feasibility and validity of brief loneliness screening tools in primary care; and implementation determinants influencing adoption, sustainability, and equity, aligning empirical evidence. Synthesized evidence demonstrates that loneliness influences health through interconnected biopsychosocial pathways shaped by structural inequities and marginalization across the life course. Brief, validated screening tools are feasible for use in time-constrained primary care settings, particularly when embedded into existing workflows. Implementation evidence indicates that electronic health record prompts, brief clinician training, and clear referral pathways enhance feasibility and acceptability, while clinician emotional labor, time pressures, and organizational readiness are key determinants of sustainability.
Conclusions:
Conceptualizing loneliness as a vital sign offers a translational pathway to normalize assessment, reduce stigma, and integrate social connection into biopsychosocial models of care. Theory-informed implementation strategies are essential to support adoption, equity, and long-term maintenance. This reframing positions primary care as a critical site for early identification and intervention and underscores the central role of health, clinical, and community psychology in advancing whole-person, socially responsive healthcare.
Keywords
Introduction
Loneliness, defined as the distressing experience that arises from a perceived discrepancy between desired and actual social relationships, 1 is increasingly recognized as a major determinant of health rather than a transient emotional state. A robust body of epidemiological evidence links chronic loneliness to elevated risks of depression, cardiovascular disease, cognitive decline, dementia, and premature mortality, with effect sizes comparable to well-established health risks such as smoking and obesity.1-3 Longitudinal studies further demonstrate that loneliness exacerbates the progression of chronic disease, impairs immune functioning,4,5 and increases healthcare utilization, particularly through emergency services, delayed preventive care, 6 and more frequent primary care visits. 7 For conceptual clarity, this manuscript distinguishes between related but distinct constructs that are often used interchangeably in policy and clinical discourse. Loneliness refers to the subjective and distressing experience of perceived social disconnection, reflecting a discrepancy between desired and actual social relationships. 8 Social isolation refers to the objective lack or infrequency of social contact or social network ties, which may or may not be experienced as distressing. 9 Social connection is used to describe a positive relational state or outcome, characterized by meaningful, supportive, and reciprocal relationships. 10 While national policy documents frequently reference loneliness and social isolation together due to their overlapping and additive associations with morbidity and mortality,1,11 this manuscript centers loneliness as the primary construct of interest because of its subjective, patient-reported nature and its suitability for routine clinical screening and intervention within primary care settings.
Recognition of loneliness as a public health concern has reached the highest levels of policy discourse. In 2023, the U.S. Surgeon General issued a national advisory identifying social isolation and loneliness as urgent health threats requiring coordinated action across healthcare, education, and community systems. 11 Despite this growing consensus, loneliness remains inconsistently assessed within healthcare settings. While screening for social determinants of health such as food insecurity or housing instability has become increasingly routine, loneliness, often a proximal driver or amplifier of these risks, remains under-identified in clinical workflows, particularly in primary care.12,13
This persistent gap between evidence and practice suggests the need for a conceptual reframing. This paper advances the argument that loneliness should be understood and operationalized as a vital sign: a measurable, actionable, clinically relevant indicator of biopsychosocial risk that can be routinely assessed and used to guide care. While vital signs have traditionally been limited to physiological parameters (temperature, heart rate, respiratory rate, and blood pressure), contemporary clinical practice has expanded this concept to include non-physiological indicators with demonstrated relevance to health and well-being, 14 such as pain, depression, and social determinants of health. 15 These expansions reflect growing recognition that clinically meaningful risk is often biopsychosocial in nature rather than purely biological. As articulated by Holt-Lunstad and Perissinotto, loneliness and social isolation now meet criteria for medical relevance due to their consistent and independent associations with morbidity, mortality, and healthcare utilization. Loneliness meets these criteria, in that it can be reliably measured using brief, validated instruments, is independently associated with morbidity, mortality, and healthcare utilization, and is actionable within clinical care through risk stratification, referral, and evidence-informed psychosocial and community-based interventions.1,7,12 Framing loneliness as a vital sign elevates its clinical legitimacy, reduces stigma, and creates pathways for earlier identification and proportionate intervention within whole-person models of care. Accordingly, this manuscript applies these vital sign criteria to loneliness, advancing a biopsychosocial reframing that positions social disconnection as a legitimate, measurable, and actionable health indicator rather than a transient emotional state.
Aim and Rationale
This narrative synthesis aims to advance a biopsychosocial reframing of loneliness as a “vital sign” to reflect a clinically relevant, measurable, and actionable health metric that can be feasibly integrated into primary care workflows to inform whole-person care, risk stratification, and referral pathways. Conceptualizing loneliness as a vital sign emphasizes its role as a modifiable determinant of health and underscores its relevance to clinical decision-making, population health, and health equity. This reframing validates loneliness as a legitimate health concern within biopsychosocial models, encourages earlier identification through routine screening, and shifts loneliness from a private emotional experience to a shared clinical responsibility. In doing so, it aligns with national and global priorities, including the U.S. Surgeon General’s call for systemic responses to social disconnection and the United Nations Sustainable Development Goals related to health, equity, and social inclusion. 11
Methodology
This paper employs a narrative synthesis intended to integrate evidence across disciplines and advance a translational conceptual argument, rather than a systematic review designed to exhaustively identify all eligible studies. A structured literature search was conducted to identify interdisciplinary peer-reviewed literature published between 2010 and 2025 spanning public health, psychology, gerontology, and translational health sciences. Searches were conducted using key biomedical and social science databases (eg, PubMed/MEDLINE, PsycINFO, CINAHL, and Google Scholar), supplemented by citation chaining of highly relevant reviews and implementation studies. Search terms included combinations of: loneliness, social isolation, screening, primary care, electronic health record, implementation, workflow, vital sign, social determinants of health, and referral.
Included sources encompassed: (a) epidemiological studies examining health outcomes associated with loneliness; (b) mechanistic research elucidating biopsychosocial pathways; and (c) implementation science studies evaluating feasibility, acceptability, and workflow integration of loneliness screening in clinical settings. Public health advisories and policy reports were included where relevant to translational and systems-level implications. This approach prioritized conceptual integration, translational relevance, and implementation feasibility across real-world primary care contexts.
Following database searching and citation chaining, full-text articles were reviewed for relevance to the manuscript’s conceptual aims. Included studies were evaluated using a structured data extraction approach to support transparent synthesis. For each included article, the following elements were extracted: study design; sample/population; clinical setting; loneliness measure; primary outcomes (clinical, behavioral, or implementation); and key findings relevant to feasibility, acceptability, workflow integration, and equity considerations. Evidence was then synthesized using a thematic narrative approach, clustering studies into 3 analytic domains: (1) loneliness as a biopsychosocial risk factor with clinically relevant downstream outcomes; (2) clinical feasibility and measurement considerations for screening; and (3) implementation outcomes and determinants of adoption within primary care workflows. This structured approach enabled in-depth appraisal of the finally included studies while retaining the integrative purpose of narrative synthesis. While a PRISMA flow diagram was not generated due to the non-systematic design, transparency was enhanced through explicit reporting of databases, time frame, inclusion domains, and analytic strategy.
Loneliness as a Biopsychosocial Health Risk
Accumulating evidence demonstrates that loneliness is associated with approximately a 26% increase in all-cause mortality, independent of traditional risk factors.2,3 It contributes to elevated risks of cardiovascular disease, stroke, cognitive decline, and dementia, and is increasingly recognized as a contributor to Alzheimer’s disease risk and progression. 2 Loneliness also undermines effective self-management of chronic illness and is associated with higher rates of depressive symptoms, anxiety, suicidal ideation, 16 and suicide mortality. 17 At the health system level, lonely individuals are more likely to delay care, miss appointments, and rely on emergency services, reflecting both unmet needs and fragmented care pathways. 6
The health effects of loneliness are best understood through a biopsychosocial lens. Biologically, loneliness activates stress-response systems, including dysregulation of the hypothalamic–pituitary–adrenal axis, increased sympathetic nervous system activity, and elevated inflammatory markers such as C-reactive protein and interleukin-6.18,19 Chronic exposure to these pathways contributes to immune dysfunction and accelerated cellular aging, including telomere shortening. 20 Psychologically, loneliness is associated with maladaptive social cognitions, including negative self-appraisals, hypervigilance to social threat, and reduced perceived social efficacy, which reinforce withdrawal and perpetuate disconnection. 19 Socially, loneliness is patterned by structural inequities, including socioeconomic disadvantage, racial discrimination, gendered caregiving burdens, and marginalization across the life course, underscoring the need for intersectional and equity-oriented approaches.19,21
Taken together, these pathways position loneliness not as an individual failing but as a contextually embedded health risk that operates across biological systems, psychological processes, and social structures. Recognizing loneliness as a vital sign reflects this complexity and signals the need for integrated responses rather than siloed interventions.
Screening Loneliness in Clinical Care
A growing literature supports the feasibility and clinical utility of routine loneliness screening. The UCLA Loneliness Scale, 22 particularly the 3-item short form (UCLA-LS3), 23 has emerged as one of the most validated and pragmatic tools for assessing subjective loneliness in healthcare settings. The UCLA-LS3 demonstrates strong internal reliability and high correlation with the original 20-item scale, while remaining brief enough for use in time-constrained clinical environments.23,24 It has been successfully deployed in primary care, geriatrics, cardiology, and mental health settings, with predictive validity for both mental and physical health outcomes.25-27
From an implementation science perspective, the UCLA-LS3 aligns with the growing movement to integrate psychosocial and social determinants of health screening into healthcare systems. 21 Its brevity, strong evidence base, and patient-centered framing make it adaptable to existing clinical workflows, particularly when supported by technological enablers such as EHR prompts. Integrating the UCLA-LS3 into primary care visits offers an opportunity not only to identify an often-overlooked risk factor but also to catalyze meaningful conversations between providers and patients about social well-being, stress, and mental health.
Implementation studies suggest that screening is most effective when embedded within existing workflows, particularly through electronic health record (EHR)–based prompts.28,29 Pollak et al, using the RE-AIM framework, evaluated a primary care–based loneliness screening and referral protocol and found high levels of provider endorsement and patient reach when screening was automated and supported by brief training. Barriers included time constraints and uncertainty regarding EHR documentation and referral options, highlighting the importance of infrastructure and support rather than the screening tool itself. Similarly, Gunn et al integrated a loneliness and social isolation screening protocol, based on the UCLA-LS3, into EHRs within family medicine clinics. Their findings showed that screening was feasible, acceptable to providers, and facilitated referral to community-based supports, though barriers such as time limitations persisted. Tung et al reported that patients generally valued being asked about loneliness during primary care visits, perceiving it as a sign of holistic, compassionate care. However, they also highlighted variability in provider confidence and available referral pathways, underscoring the importance of readiness and infrastructure in successful implementation.
Qualitative findings from primary care–based implementation studies similarly underscore these dynamics, with clinicians describing loneliness screening as aligned with whole-person care while also highlighting the emotional labor involved in addressing positive screens and the need for adequate training, referral infrastructure, and institutional support.13,29 Concerns about compassion fatigue and emotional burden mirror broader implementation science findings, which emphasize leadership engagement, clinician well-being, emotional readiness, and workflow compatibility as critical determinants of sustainability.30-32 To synthesize these theory-informed strategies and clarify how implementation frameworks informed practical workflow design, Table 1 summarizes recommended approaches for integrating loneliness screening into primary care.
Summary of Approaches.
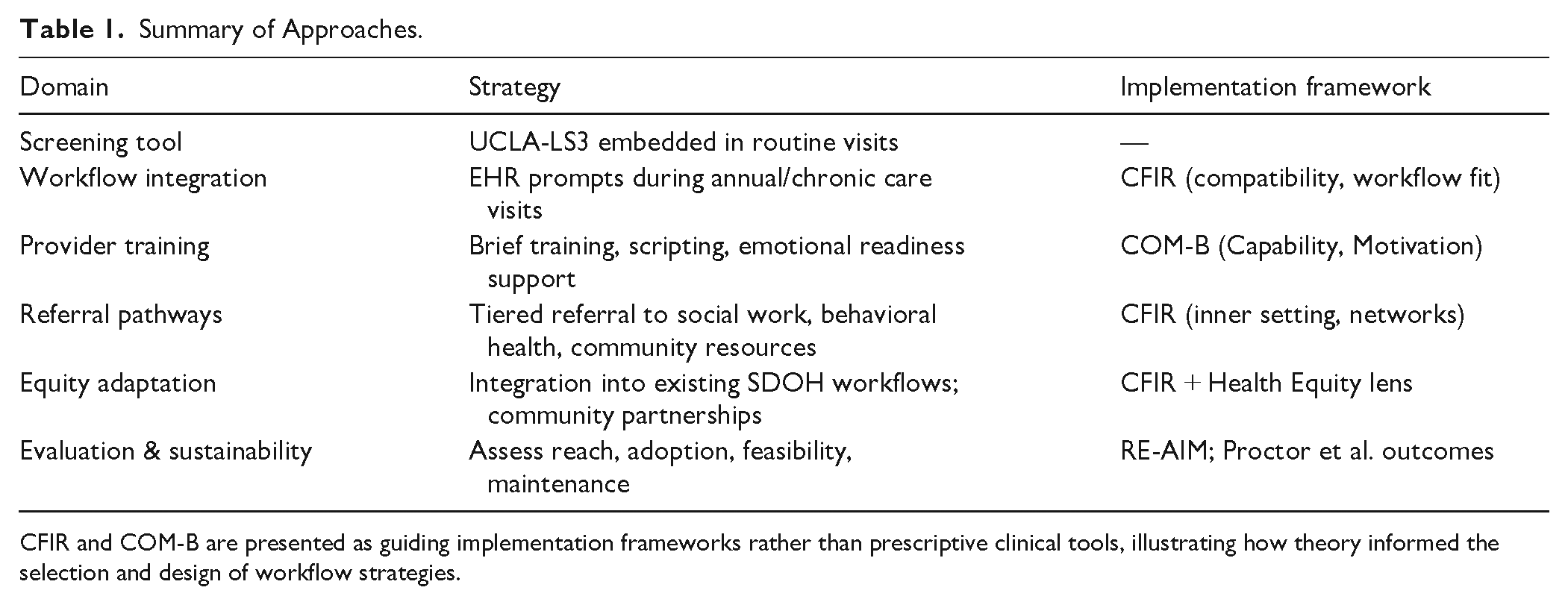
CFIR and COM-B are presented as guiding implementation frameworks rather than prescriptive clinical tools, illustrating how theory informed the selection and design of workflow strategies.
Implementation Science Frameworks and Theory-Informed Strategies Supporting Loneliness as a Vital Sign
Operationalizing loneliness as a vital sign in primary care requires more than psychometric validity; it necessitates systematic strategies to ensure that screening is feasible, acceptable, and sustainable within complex healthcare environments. Implementation science frameworks provide essential conceptual scaffolding for translating loneliness screening from evidence to routine practice by clarifying what should be evaluated, why adoption succeeds or fails, and how behavior and systems can be supported to change. 33
The Consolidated Framework for Implementation Research (CFIR 2.0) offers a comprehensive, multilevel structure for understanding determinants of implementation across intervention characteristics, inner and outer settings, characteristics of individuals, and implementation processes. 31 In the context of loneliness screening, CFIR is particularly well suited to capturing the interaction between clinic culture, workflow compatibility, leadership engagement, and provider readiness, which are factors repeatedly identified as barriers to psychosocial screening in primary care. Framing loneliness as a vital sign aligns with CFIR’s emphasis on legitimacy and compatibility: embedding loneliness screening within familiar workflows, such as electronic health record (EHR) prompts alongside depression or other social determinants of health screening, positions it as a normative component of care rather than an optional or peripheral task. CFIR thus supports the argument that loneliness screening must be understood as a system-level innovation, not merely an individual clinical behavior. Further, CFIR highlights the multiple interacting factors that shape optimal pre-implementation contexts, emphasizing both the flexibility required for successful adoption and the complexity of implementation across open and variable healthcare settings, including community-based settings. 34
While CFIR addresses contextual determinants, the COM-B model (Capability, Opportunity, Motivation–Behavior) provides a complementary behavioral theory explaining how and why clinicians adopt new practices. 35 Applying COM-B to loneliness screening highlights that provider uptake depends on clinicians’ capability, including knowledge of loneliness as a health risk and skills to discuss it sensitively; opportunity, such as sufficient time, workflow integration, EHR prompts, and referral pathways; and motivation, including belief in the clinical value and ethical relevance of addressing loneliness. Conceptualizing loneliness as a vital sign directly strengthens motivation by reframing social disconnection as a legitimate, actionable health concern rather than a purely social or emotional issue. Together, CFIR and COM-B enable a layered understanding of both structural and behavioral mechanisms required to normalize loneliness screening in primary care.
Evaluation of loneliness screening initiatives further benefits from the RE-AIM framework, which emphasizes public health impact through systematic assessment of reach, effectiveness, adoption, implementation, and maintenance. 36 RE-AIM is particularly relevant for framing loneliness as a vital sign because it foregrounds population-level reach and long-term maintenance, moving beyond pilot feasibility to questions of scalability and sustainability. Prior loneliness screening studies using RE-AIM demonstrate that while screening tools may be acceptable and clinically relevant, adoption and maintenance hinge on workflow integration, provider training, and referral infrastructure, reinforcing the need for theory-informed implementation strategies when positioning loneliness as a routine health indicator.
Finally, Proctor et al’s Implementation Outcomes Framework provides conceptual clarity around what constitutes success in early-stage implementation by distinguishing implementation outcomes, such as acceptability, feasibility, and appropriateness, from clinical or service outcomes. 37 This distinction is critical when advancing loneliness as a vital sign: before downstream health benefits can be expected, screening must first be perceived by clinicians as workable, acceptable, and appropriate within real-world practice constraints. Anchoring evaluation in Proctor’s framework ensures that loneliness screening is assessed not only for its theoretical importance but also for its practical viability as a routine component of primary care.
Together, these frameworks directly inform the selection of multilevel, theory-informed implementation strategies. Training and scripting tools enhance clinicians’ capability to address loneliness sensitively; EHR prompts and structured referral pathways create opportunities by reducing friction and standardizing workflows; and values-based messaging reinforces motivation by aligning loneliness screening with professional identity and patient-centered care. When applied in concert, CFIR and COM-B support adaptive implementation strategies that are responsive to local context while maintaining fidelity to core principles, and mixed methods evaluations enable iterative refinement over time, promoting equity, sustainability, and scalability. 38
Collectively, integrating CFIR, COM-B, RE-AIM, and Proctor’s framework strengthens the argument that conceptualizing loneliness as a vital sign is not merely a semantic shift but an implementation challenge requiring explicit attention to context, behavior, evaluation, and sustainability. This integrated approach situates loneliness screening within a robust translational pathway that links biopsychosocial theory, clinical practice, and health system change.
Translational and Policy Implications
Policy-level recognition of loneliness as a public health priority has begun to translate into concrete practice innovations. For example, the U.S. Surgeon General’s 11 call for integrating social connection into healthcare delivery is reflected in primary care–based screening and referral models that embed loneliness assessment within existing electronic health record workflows.13,28 These initiatives operationalize policy priorities at the community level by linking brief loneliness screening to community health workers, social prescribing programs, and local resource referral platforms. Similarly, health system–level efforts described by Kepper et al 21 demonstrate how national attention to social determinants of health can be enacted through clinic–community partnerships that address loneliness alongside food insecurity, housing instability, and transportation needs.
Reframing loneliness as a vital sign has significant translational implications. It operationalizes decades of research by embedding measurement into routine care, enabling population-level surveillance, early intervention, and resource allocation. It also advances health equity by making visible a risk factor that disproportionately affects marginalized populations and often remains hidden in clinical encounters. At the policy level, loneliness screening aligns with national and global initiatives emphasizing social connection as foundational to health, including the Surgeon General’s advisory and international strategies addressing social determinants of health and inequality. 11
Psychology plays a central role in this translational effort. Health psychology, geropsychology, and community psychology contribute not only measurement tools but also intervention strategies targeting social cognition, emotion regulation, and behavior change at both individual and system levels. Importantly, the act of measuring loneliness carries symbolic weight: it communicates to patients that social connection matters, that disconnection is not a personal failure, and that healthcare encompasses more than biological parameters alone.
Importantly, implementing loneliness screening in under-resourced primary care settings raises critical equity considerations. Clinics serving marginalized populations often face constrained referral infrastructure, limited time, and workforce capacity challenges, all of which can undermine the feasibility and sustainability of additional screening initiatives.21,30 Implementation science frameworks emphasize that equity-oriented adaptation, including community partnerships, task-sharing, and tiered or stepped response models, is essential to prevent unintended harms and ensure that new screening practices do not exacerbate existing disparities.34,38 Embedding loneliness screening within existing social determinants of health workflows, rather than introducing parallel processes, may reduce clinician burden while enhancing reach, normalization, and sustainability in resource-constrained settings.21,28 These community-embedded approaches illustrate that policy-driven screening initiatives are most effective when paired with local infrastructure and partnerships capable of responding to identified needs, particularly in under-resourced settings.
From an ethical standpoint, routine loneliness screening is difficult to justify when health systems lack adequate capacity, referral infrastructure, and clinician support to respond meaningfully, as identifying vulnerability without the ability to offer assistance risks distress, unmet expectations, and erosion of trust.39,40 Ensuring sufficient resources, training, and community partnerships is therefore not merely an implementation consideration but also an ethical one, particularly to avoid exacerbating inequities when screening is concentrated in under-resourced settings.21,41,42
Conclusion
Loneliness is a measurable, clinically relevant, and modifiable determinant of health with implications across physical, mental, and social domains. Conceptualizing loneliness as a vital sign does not imply overmedicalization, but rather offers a pragmatic translational pathway to normalize assessment, reduce stigma, and guide proportionate responses within primary care. When supported by theory-informed implementation strategies, routine loneliness screening can advance early identification, equity, and whole-person care. Future research should evaluate long-term outcomes, referral effectiveness, and sustainability across diverse healthcare settings.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.