
Abstract
Introduction:
Patient-provider trust is essential for effective healthcare delivery, influencing care engagement, disclosure, and adherence. Mistrust can delay diagnoses, reduce care utilization, and worsen outcomes. While cultural competence trainings aim to improve provider awareness, few studies examine how community health workers (CHWs) perceive and support trust-building in clinical care.
Purpose:
To explore strategies for building and maintaining patient-provider trust from the perspectives of CHWs.
Methods:
Using a Community-Based Participatory Research approach, 39 CHWs from 3 rural-serving health centers in California participated in semi-structured focus groups. English and Spanish sessions were co-led by University researchers and trained CHW partners. Deductive thematic analysis was conducted in Dedoose, and descriptive statistics were generated using Stata 17.
Results:
CHWs identified 3 factors that shape patient-provider trust: (1) Power dynamics, such as provider-dominated conversations and time constraints, limit trust-building; (2) Communication that fosters emotional safety, including provider attentiveness and respectful verbal and nonverbal behaviors; and (3) Cultural respect and competence, emphasizing the importance of recognizing patients’ beliefs and providing language-concordant care.
Discussion:
CHWs offer community-informed insights on trust-building that can inform culturally responsive and equity-oriented interventions, particularly in rural and underserved regions. Future efforts should explore co-developing training modules with CHWs to strengthen patient-provider trust.
Keywords
Introduction
Patient-provider trust is essential for effective healthcare delivery. Trust refers to the belief that healthcare providers will act competently, honestly, and in the best interest of their patients. 1 When trust is established, patients are more likely to engage in care, disclose sensitive health information, and adhere to medical guidance, ultimately leading to better health outcomes. 2 Conversely, mistrust can result in delayed diagnoses, underutilization of healthcare services, and increased health risks.3,4 Evidence suggests that trust is not experienced equally across populations; for example, 52% of Latino adults in the U.S. report having at least 1 negative experience with healthcare providers, often tied to feelings of not being taken seriously. 5 Rural communities, such as California’s San Joaquin Valley (SJV), face unique barriers that further undermine trust, including provider shortages, language barriers, and structural inequities such as lack of transportation.6-8 In geographically isolated areas, transportation challenges can delay care, hinder clinic access, and contribute to patient frustration, ultimately eroding trust in the healthcare system. 9
To address these trust-related disparities, many health systems have adopted provider trainings in cultural competence, especially when serving racially, ethnically, and linguistically diverse populations. A systematic review found that cultural competence training improved healthcare providers’ cultural awareness and sensitivity, including greater responsiveness to the needs of non-English-speaking patients. 10 Providers who completed medical Spanish courses also demonstrated stronger skills in collecting patient information. The review further noted an increase in patient satisfaction when care was delivered by providers who had undergone cultural competence training.
Cultural competence trainings often include modules on historical injustices (eg, discriminatory policies, forced acculturation, and colonialism), cultural belief systems (eg, familial obligations and social hierarchies), communication approaches (eg, respectful dialog and appropriate use of interpreters), and structural issues (eg, racism, institutional discrimination, and workforce diversity). 11 Despite these extensive topics, such training programs may fall short in addressing the structural and contextual barriers that shape trust, particularly in rural settings. Additionally, there is a risk of pathologizing cultural practices or attributing health concerns solely to culture, 11 which may obscure clinical needs or social determinants of health.
Few studies have examined how community health workers (CHWs), who serve as cultural and linguistic intermediaries, perceive the mechanisms of trust-building in clinical care. CHWs bring insider knowledge of both clinical systems and community contexts, positioning them to identify structural gaps and trust-building strategies that may not be visible to healthcare providers or administrators. To address this gap, this qualitative study explores CHW perspectives on how patient-provider trust is built and maintained within clinical care settings in the SJV, a rural region marked by persistent health disparities and a large population of Spanish-speaking patients. The study is guided by the following research question: From the perspective of CHWs, what strategies build and maintain patient-provider trust among patients in rural communities of the SJV?
Methods
A Community-Based Participatory Research (CBPR) approach was used to explore the barriers that interfere with patient-provider trust from the perspective of CHWs. 12 This study was approved by the University of California, Merced (UCM), Institutional Review Board (#UCM2024-2).
Study Setting
The San Joaquin Valley (SJV) is a predominantly agricultural region in Central California, often referred to as the “breadbasket of the world” due to its high food production. 13 The region is home to a majority Latino (56%) and non-Hispanic White (29%) populations, in comparison to the overall state of California (39% Latino and 35% non-Hispanic White). 14 The SJV also has a large farmworker population, many of whom experience economic hardship, limited access to healthcare, and increased exposure to occupational and environmental risks.15,16 As defined by the U.S. Census Office of Management and Budget (OMB), the SJV and health centers part of this study serve various rural and medically underserved communities across 8 SJV counties: Fresno, Kern, Kings, Madera, Merced, San Joaquin, Stanislaus, and Tulare. 17
Recruitment and Data Collection
Lead staff at each of the 3 participating health centers recruited participants for focus groups through in-person invitation and email outreach. Eligible participants were required to be 18 years or older, actively working or volunteering as a CHW at their respective health centers, and able to communicate in Spanish, English, or both.
A total of 4 in-person focus groups were conducted between April and May 2024 across 3 health centers. At each site, 1 to 2 leadership staff members—who completed a 2-h qualitative training led by the University research team and the Collaborative Institutional Training Initiative (CITI) 18 certification for ethical human subjects research—facilitated the discussions. Focus groups were conducted in English or Spanish, with support from a university researcher and a research assistant who also took field notes.
Before the focus group discussions, the research team reviewed the study purpose and obtained verbal consent to participate and record. Participants could use pseudonyms, providing consent under that name. Focus groups ranged from 32 to 80 min, averaging 65 min.
Following each session, CHWs completed a brief, self-administered demographic survey in their preferred language (English or Spanish). Paper responses were entered into a secure database. Incentives varied by each site’s policies, for example, Health Center #1 offered items such as water bottles, cooking utensils, speakers, and coffee mug warmers; Health Center #2 provided $40 gift cards; and CHWs at Health Center #3 were compensated for their time directly through the grant disbursed to the site.
Interview Guide Development
The semi-structured focus group guide (Supplemental Material) was grounded in the Health Belief Model, 19 Empowerment Theory, 20 Andersen’s Behavioral Model, 21 and the Penchansky’s and Thomas Model of Access. 22 The guide was piloted with 6 to 8 CHWs at each site before finalization. It included 13 questions on trust, provider interactions, barriers to care, and communication practices. Sample questions asked CHWs to define trust, describe provider communication, and identify barriers affecting patient trust in their provider and overall care.
Data Analysis
All focus groups were audio-recorded and transcribed. Spanish-language transcripts were translated into English and double-checked by bilingual team members to ensure accuracy and preserve meaning. All transcripts were uploaded to Dedoose for coding and analysis. 23 A team of research assistants and University researchers independently coded each transcript using a structured codebook based on the guiding frameworks.19-22 Open coding was also used to identify new concepts. Coders wrote analytic memos, which were reviewed during weekly research team meetings.
Thematic analysis was used to identify recurring patterns across the data. All coded excerpts were exported to Excel and categorized into themes and sub-themes relevant to the research questions. Rather than relying solely on saturation, all excerpts were reviewed to ensure inclusiveness of perspectives. Themes and sub-themes were reviewed by an additional team member, revised for clarity, and finalized in consultation with the senior author. Descriptive statistics summarizing participant demographics were generated using Stata/SE 18.5 (StataCorp). 24
Reflexivity Statement
The co-authors of this study have collaborated on previous studies. All co-authors are first generation Latinas who have worked on community-based research studies in the SJV and are mindful of our similarities and differences. We engaged in reflexivity to uncover unconscious biases that may nuance our work and we externalize our assumptions to try to minimize them. For example, the senior author grew up in the SJV and brings a longstanding record of collaborative research projects in the region with CHWs. Thus, she remained attentive to potential power dynamics throughout the study. To mitigate power imbalances and potential bias, CHWs contributed to the development of the interview guide, participated in data collection, and provided feedback on the final themes. This reflexive approach ensures that our analysis is representative of CHWs’ lived experiences.
Results
A total of 39 CHWs participated in the focus groups. The majority were female (76.9%) and identified as Hispanic/Latina (82.1%). Spanish was the most commonly reported primary language (48.7%), followed by English (23.1%) and bilingual proficiency in English and Spanish (17.9%). Regarding educational attainment, the most common level was a high school diploma (38.5%) followed by a bachelor’s degree (25.6%). Most participants reported CHW as their primary employment (76.9%), while a smaller proportion served in a volunteer capacity (15.4%). Table 1 provides a full summary of participant characteristics.
Characteristics of Community Health Worker (CHW) Focus Group Participants by Health Center (N = 39).
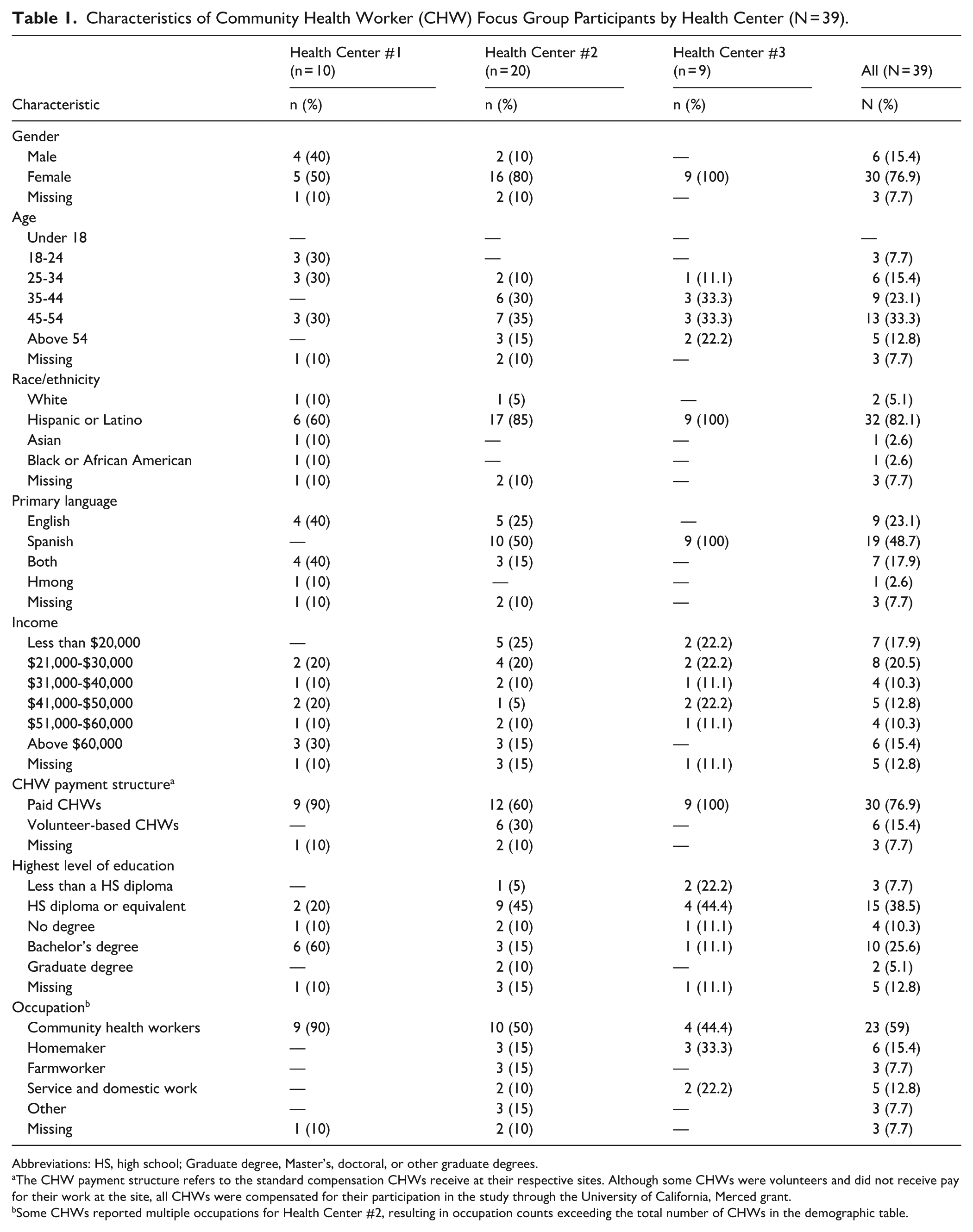
Abbreviations: HS, high school; Graduate degree, Master’s, doctoral, or other graduate degrees.
The CHW payment structure refers to the standard compensation CHWs receive at their respective sites. Although some CHWs were volunteers and did not receive pay for their work at the site, all CHWs were compensated for their participation in the study through the University of California, Merced grant.
Some CHWs reported multiple occupations for Health Center #2, resulting in occupation counts exceeding the total number of CHWs in the demographic table.
Factors Contributing to Building and Maintaining Patient-Provider Trust
This study identified 3 key factors that contribute to building and maintaining patient-provider trust in rural communities of the SJV. First, CHWs described how trust can be hindered through power dynamics and rushed clinical encounters. In contrast, they emphasized that trust can be strengthened through communication that fosters emotional safety. Similarly, culturally respectful and language-concordant care were seen as essential to cultivating trust. Across all themes, CHWs emerged as vital partners who helped bridge structural and relational gaps, drawing from their own unique roles and lived experiences.
Power Dynamics and Time Constraints Limit Trust-Building
CHWs described how rushed visits and provider control over conversations often discouraged patients from disclosing personal or health-related concerns. When patients feel restricted, dismissed, or unable to ask questions, they may disengage or lose trust in the healthcare system. These practices reinforce hierarchical power dynamics within clinical encounters and reduce opportunities to build meaningful, trusting patient-provider relationships.
CHWs recounted instances where providers limited the scope of conversations or dismissed patients’ concerns: I don’t feel too trusting because you can’t openly ask them what your doubts are about your health problems because then they cut off the conversation [. . .]. If you go [for]the flu, you can only ask about the flu. [. . .] They don’t open up the possibility for you to ask about anything else. -Health Center #3
Time constraints were also seen as a major barrier to trust. One CHW emphasized that spending time with patients signaled respect and care, which helped build trust: One of the things is to take your time and dedicate a few minutes to that person, more personal, so that they can feel more trusted. -Health Center #2
Communication That Fosters Emotional Safety Strengthens Trust
CHWs emphasized the importance of relational behaviors that help patients feel heard, respected, and emotionally safe. These included being addressed by their name, maintaining eye contact, and allowing patients to speak freely without interruption. Such gestures, though simple, can challenge hierarchical norms and support disclosure and openness.
One CHW reflected on how provider attentiveness shaped trust: I don’t know how he [the doctor] did it because I know he had a lot of work, but he had the patience to talk to us and ask, ‘How are you doing? What else can I help you with?’ -Health Center #2
Another CHW underscored how feeling heard deepens personal connection and mutual trust: As long as the provider is able to build that connection with their patient and provide them with the help that they need, and give them all the tools that they need to improve their health, we’ll build that trust within both of them [patient and provider]. -Health Center #1
Eye contact was also identified as an important behavior of respect and attention. One CHW explained how the lack of this basic gesture could undermine trust: Sometimes you feel like you’re being ignored because you’re asking the question, you want them to be attentive. [. . .] we as Latinos always want to be looked in the eye, that you can have that dialogue with the person. But in this case when you go to the doctor, the doctor is always writing. They are not there; it’s like they are not there taking care of you. So the person cannot open up, cannot have that trust from doctor, to doctor. -Health Center #3
Even small gestures, such as calling patients by their name, were seen as meaningful acts that strengthened trust: When they call you by your name. [. . .] You feel like they know you. -Health Center #2
CHWs themselves often helped foster emotional safety by drawing on empathy and shared experience. One CHW described supporting a patient with mental health stigma by sharing her own experience: I said, ‘Look, I struggle with depression myself’ [. . .] You saw like a light came to her face. It took me like a year and a half to convince her to finally get ahold of a therapist [. . .]. Until today, she still requires that little push [. . .], she’s doing great. Attending to all her appointments [. . .] But then four weeks later, [. . .] when I look at her chart, I see that she started missing appointments. And it’s when you got to reinforce that, ‘Hey, you can do this.’ So it would be, again, the trust. [. . .] being at the same level they are. I’ve been there, I understand where you are coming from.
Cultural Respect and Competence Are Essential to Trust-Building
CHWs also emphasized that cultural respect and language-concordant care are fundamental to patient-provider trust. When providers recognize and affirm patients’ cultural beliefs, rather than dismissing them, patients feel seen and respected. As trusted cultural and linguistic liaisons, CHWs often fill gaps in communication and understanding.
For example, one CHW described how providers often shut down conversations around traditional remedies, eroding patient trust: Being like the Hispanic culture, there’s a lot of different beliefs, traditions, or things like natural remedies [that are] shut down right away. Like, ‘Nope, that doesn’t work.’ -Health Center #2
Rather than dismissing such beliefs, CHWs take a bridging approach. One CHW described validating cultural practices while also helping patients access appropriate care: Instead [of] me trying to make them [the patient] understand that going to the doctor is important, I need to inform myself first, [. . .] give them an opportunity [to] still do the culture portion of it and then we can work together with the health system. -Health Center #2
Language-concordant care also served as a trust-building mechanism. One CHW reflected on how language goes beyond translation as it reflects cultural understanding: You have to [. . .] grow in language. [. . .] The language implies that you understand cultures. It really, [. . .] implies that you’ll be able to speak to a lawyer the same as to a farmer. -Health Center #1
Another CHW emphasized how shared language strengthened rapport: I’m able to use [Spanish] for the benefit of the community and the patient when we’re speaking. –Health Center #1
Discussion
This study offers insight into strategies for building and maintaining patient-provider trust in rural communities of the SJV, drawn from the perspectives of CHWs. Positioned at the intersection of healthcare systems and community experiences, CHWs provide a unique advantage on the conditions that either foster or hinder trust. Through their experiences as patients and their direct work with patients, CHWs identified power dynamics, communication practices, and cultural respect as core factors influencing patient-provider trust.
This study highlights how power dynamics and time constraints can discourage patients from disclosing personal or health-related concerns. Rushed clinical visits and provider-dominated conversations were seen as common deterrents to patient openness. These findings align with prior research indicating that patients are less likely to share concerns when they feel dismissed or interrupted by providers. 25 In rural contexts, where provider shortages are common, these dynamics may be intensified due to additional time constraints, further marginalizing patients who already face structural barriers to care.6,7 These findings underscore the need for structural interventions that increase provider capacity and allow time for relationship-building with patients, particularly in underserved and rural communities.
Findings also emphasize the importance of communication that fosters emotional safety. CHWs discussed how trust was strengthened when patients felt heard, respected, and personally acknowledged, such as being addressed by name, offered eye contact, and allowed time to speak without interruption. These relational behaviors not only reduce patients’ fear of judgment but also create the conditions for openness and long-term engagement. Prior studies similarly highlight that emotional safety and rapport-building contribute to patient-provider trust, particularly when providers demonstrate attentiveness and cultural sensitivity.26,27
In this study, CHWs’ ability to relate through shared experiences and empathy further promoted patient engagement and comfort, underscoring their role as trusted relational figures within care teams. 28 Prior research shows that providers who approach illness from the patient’s perspective foster greater trust and patient-centered communication. 29 More intentional integration of CHWs into care delivery may help offset provider shortages in rural regions like the SJV6,7 by allowing for a more personalized care for patients. Policy efforts that support reimbursements for CHW-led visits or warm hand-offs between providers and CHWs could help institutionalize their role in building trust and improving care continuity.
CHWs in this study also emphasized that cultural respect and competence are essential to trust-building, especially in diverse populations. Language-concordant care was identified as a key facilitator that fosters rapport and encourages patient openness, echoing literature suggesting that shared language can strengthen patient-provider relationships and support follow-up adherence and patient-initiated communication, though findings are mixed across specific health behaviors. 30 Beyond language concordance, CHWs stressed the value of cultural humility, particularly providers’ willingness to acknowledge and engage with patients’ beliefs without judgment. This aligns with prior studies noting that trust is strengthened when providers reflect on their own biases and engage patients’ cultural contexts. 26
However, cultural competence trainings may fall short if they overlook broader contextual factors of rural, farmworking regions such as social determinants of health, historical discrimination, and structural inequities. To be effective, such trainings should be tailored not only to patients’ linguistic and cultural identities but also to the specific lived experiences. 11 In regions like the SJV, this includes developing content specific to rural, farmworking populations, and incorporating trauma-informed, equity-focused frameworks. Future researchers should engage CHWs in co-designing and co-facilitating these trainings, drawing on their firsthand insights to improve communication and trust-building practices among healthcare staff.
Strengths and Limitations
This study provides several notable strengths. First, it draws on the perspectives of 39 CHWs across 3 health centers serving diverse rural communities in the SJV. As trusted members of the communities they serve, CHWs often share cultural, linguistic, and lived experiences with patients, allowing them to provide insights that might not be captured through insights from health professionals. Their unique position, as community members and clinic staff, provides a holistic understanding of both patients’ needs and organizational dynamics. Additionally, this study was grounded in a CBPR approach. Lead CHWs at each site contributed to the development of the interview guide and were actively involved in recruitment and facilitation of the focus groups, strengthening cultural relevance, rapport, and the validity of the data.
Several limitations should also be considered. CHWs’ responses were self-reported and may be subject to recall bias or social desirability bias, particularly given the interpersonal nature of trust-building strategies. The findings also reflect the experiences of CHWs from 3 health centers within the SJV and may not be generalizable to other rural regions in California or nationally. Additionally, because CHWs facilitated the focus groups at their own health sites, power dynamics or collegial relationships may have influenced how openly some participants shared their perspectives.
Conclusion
The perspectives of CHWs in this study align with existing literature, reinforcing that their role in building patient-provider trust goes beyond cultural and linguistic mediation. CHWs offer a holistic understanding of how to effectively communicate with and support rural patients in the SJV, drawing from both lived experiences and professional practice. Given the mixed evidence in existing research, future studies should focus on co-developing and evaluating tailored training interventions, particularly those that integrate CHW insights, to strengthen the trust in rural healthcare settings.
Supplemental Material
sj-doc-1-jpc-10.1177_21501319261425544 – Supplemental material for Community Health Worker Perspectives on Building Patient-Provider Trust in Rural Communities of the San Joaquin Valley, California: A Qualitative Study
Supplemental material, sj-doc-1-jpc-10.1177_21501319261425544 for Community Health Worker Perspectives on Building Patient-Provider Trust in Rural Communities of the San Joaquin Valley, California: A Qualitative Study by Kimberly D. Sánchez, Micaela Velasco Sandoval and Rosa D. Manzo in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We are grateful to our community partners, community health workers, students, and university research team for their support in the project. Funding was provided by Genentech Foundation, a member of the Roche Group.
Ethical Considerations
This study was approved by the University of California, Merced Institutional Review Board (#UCM2024-2) on January 8, 2024.
Consent to Participate
Informed consent was obtained verbally before participation. The consent was audio-recorded in the presence of research team witnesses, and all data was anonymized.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Genentech Foundation, a member of the Roche Group [grant number FR-012660].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available upon request from the corresponding author*. The data are not publicly available due to privacy restrictions.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.