
Abstract
Research:
Telehealth increased substantially during the COVID-19 pandemic. There is evidence that telehealth can improve access to care. Little is known about the use of patients’ telehealth prenatal care prevalence by race and ethnicity, especially in CHCs. To assess patient usage of telehealth prenatal visits by race and ethnicity between 2019 and 2023, we included EHR data from pregnant non-Hispanic, Latina, White and Black patients and measured the proportion of telehealth prenatal visits. Adjusted estimated marginal means were calculated and described using a generalized beta mixed effects model to account for clinic clustering.
Findings:
The proportion of prenatal telehealth visits increased rapidly for all groups until 2021, when they slowly began to decline and level off. In 2019, White Latinas had the lowest percent (11.3%, 95% CI = 11.0, 11.6) and non-Hispanic Black patients had the highest percent (13.7%, 95% CI = 13.2, 14.2). By 2023, non-Hispanic White patients had the highest percentage (25.0% 95% CI = 24.4, 25.6) and Black Latinas had the lowest percentage (18.2%, 95% CI = 17.1, 19.4).
Conclusions:
While all racial and ethnic groups exhibited similar trends in telehealth usage, the shifts in percentages highlight important disparities. This research lays the groundwork to evaluate prenatal outcomes related to virtual care and help clinics prioritize effective strategies in telehealth services for prenatal care.
Introduction
The prevalence of telehealth visits (i.e., scheduled and synchronous healthcare delivered remotely by phone or audiovisual technology) increased substantially during the COVID-19 pandemic and telehealth is still in wide use among community health centers (CHCs).1,2 There is evidence that telehealth visits can improve access to care for patients, such as those who live in rural areas or those without time to travel to and from an appointment. 3 Telehealth may support ongoing management of various health conditions through virtual consultation, therapy and remote monitoring and screening.4,5 Some providers find telehealth useful as it reduces overhead costs. 6 In the context of prenatal care, telehealth visits have been associated with comparable patient satisfaction and comparable pregnancy outcomes, while also offering benefits such as cost savings, reduced clinic wait times and fewer appointment cancellations.7-12 These benefits highlight the potential of telehealth visits for prenatal care to advance health equity, particularly when implemented in settings that serve vulnerable populations. However, little is known about the use of patients’ telehealth prenatal care prevalence over time and by race and ethnicity, especially in CHCs. CHCs are adept at providing care to underinsured populations and marginalized groups like Black and Latina patients, and provide a large volume of prenatal care to underserved communities.13-18 Understanding these patterns could help identify disparities in access to telehealth prenatal care, inform equitable telehealth implementation strategies and guide clinical priorities to ensure that telehealth services effectively reach those who may benefit most.
To fill this gap, we assess patient usage of telehealth prenatal visits by race and ethnicity from 2019 to 2023 among patients in a multi-state network of CHCs across 46 states.
Methods
We analyzed data from OCHIN Inc., a linked multistate electronic health record (EHR) network of CHCs across the United States. OCHIN Inc. (not an acromyn) is a nonprofit health information technology organization which provides a single, patient-linked instance of the Epic® EHR. The EHR were obtained from the Accelerating Data Value Across a National Community Health Center Network (ADVANCE) Clinical Research Network (CRN), a member of PCORnet®. ADVANCE is a multicenter collaborative led by OCHIN.
We extracted data from structured EHR fields for patients across 603 community-based primary care clinics live on the OCHIN network for years 2019-2023 in 46 states. We chose this time-period to illustrate changes over time and through the COVID-19 pandemic. The data used in this study were collected during routine primary care and consent from patients to use data in research was obtained from clinics when care was initiated. This study was approved by the Oregon Health & Sciences University Institutional Review Board (Supplemental Table 1).
Our study population included non-Hispanic White, non-Hispanic Black, Latina White and Latina Black women aged 18 years and older between April 2019 and December 2023, with at least 1 prenatal visit (in person or telehealth) to an OCHIN clinic during the study period. Clinics were only included if they provided both in-person and telehealth prenatal care during the study period to eliminate clinic policy bias (not providing the option of telehealth) and focus on visit type selection. Only clinics that offered both in-person and telehealth prenatal care during the study period were included in the study. This criteria was elected to minimize bias originating from clinic policies that do not offer telehealth, thereby allowing the analysis to focus more accurately on patient choice regarding visit type.
The primary dependent variable of interest was the proportion of prenatal visits that were delivered via telehealth each year in the study period among patients in each racial-ethnic group. Consistent with previous literature assessing prenatal care from the EHR, prenatal visits in this study are defined using International Classification of Disease codes (Appendix I). 18
The primary independent variable was a combined categorization of race and ethnicity. We classified individuals into 4 groups: (1) non-Hispanic White, (2) non-Hispanic Black (3) White Latina, (4) Black Latina. While we use the term Latina because it is more often preferred among our study population, the actual variable collected in the EHR is “Hispanic” and “non-Hispanic.” Other race and ethnicity groups (e.g., Asian, American Indian/Alaska Native, or multiracial) were not included in this analysis due to the small sample size.
Covariates included patient age at first prenatal visit (18+), US geographic region (West, Northeast, South, Midwest), family income as a percent of the federal poverty level (FPL) (always ≥138%, above and below 138%, always <138%, never documented), insurance status throughout the study period (always insured, sometimes insured, never insured), primary clinic urban/rural status (Urban, Rural), diagnosis of gestational diabetes (Yes/No), and Charlson Comorbidity Index score. By including these covariates, we aim to address residual differences among patients with similar socioeconomic and clinical profiles.
First, we described the overall sample and examined characteristics by race and ethnicity. Next, we described the sample characteristics by race and ethnicity by start year, 2019 and end year, 2023. Then, we described the sample baseline characteristics aggregated by race and ethnicity and those who had any telehealth prenatal visits and those with only in-person visits. Finally, we used a generalized beta mixed effects model for proportional data to estimate the proportion of telehealth prenatal visits accounting for all covariates. Standard errors were clustered on patients’ primary clinic to account for within-clinic correlation. We report unadjusted and adjusted proportions of prenatal telehealth visits. Two-sided statistical significance was set at P < .05 and analyses were conducted using RStudio version 4.2.1.
Results
The study population consisted of 104 282 women aged 18+ with at least 1 prenatal visit (Table 1). The average age at first prenatal visit was 29 years old. Latinas had the highest incidence of gestational diabetes, and 7% of White Latinas and 4% of Black Latinas had a diagnosis during pregnancy compared to almost 3% for both non-Hispanic White and non-Hispanic Black women. Over time, the percent of women at or below 138% FPL increased for all groups even though Black Latinas increased the most, from 69% to 86%. Most women had insurance at some point in the study period but the percent of women who were always insured during their prenatal visits decreased among all race and ethnicity groups between 2019 and 2023.
Characteristics of Patients with Prenatal Visits by Race-Ethnicity Groups.
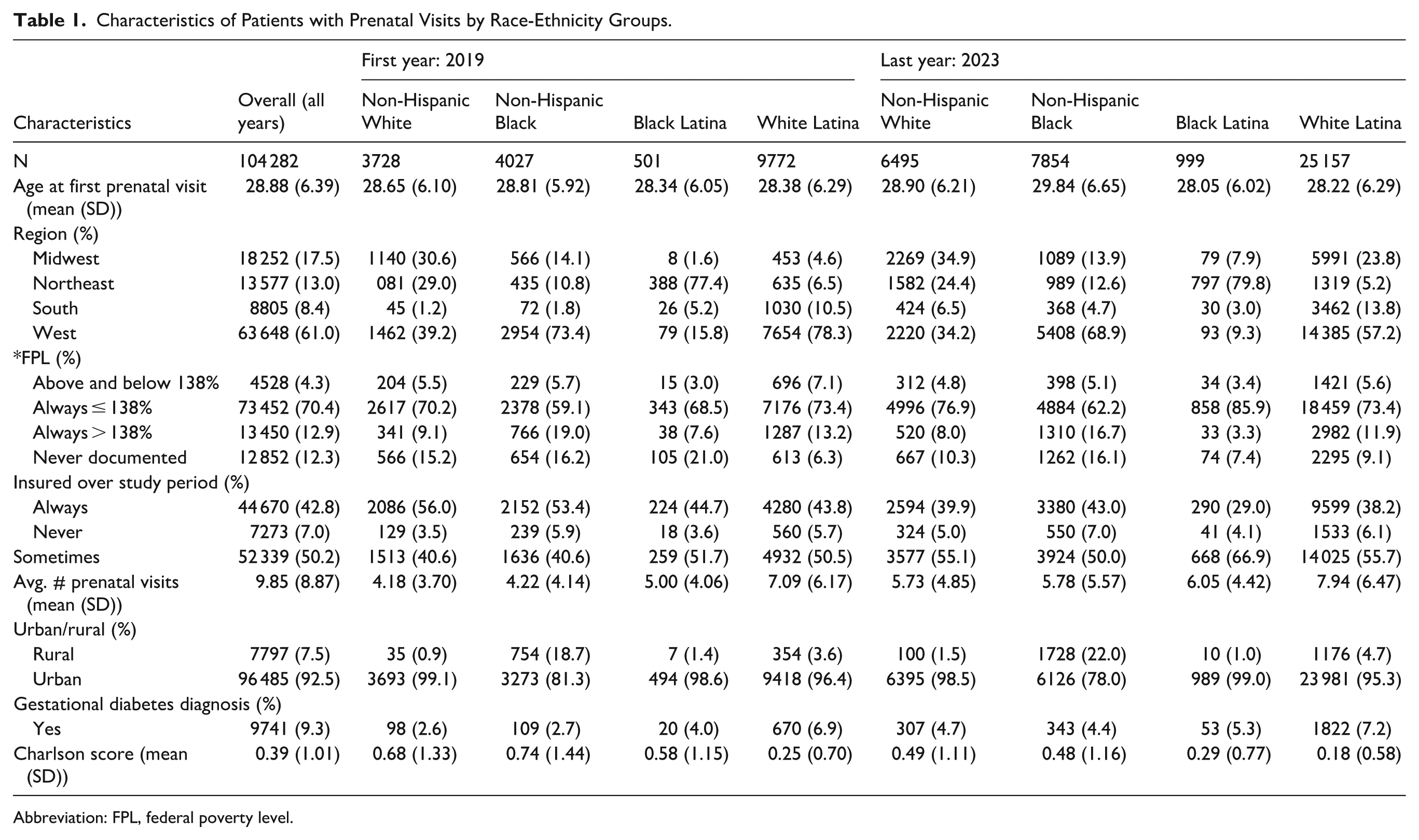
Abbreviation: FPL, federal poverty level.
Table 2 describes the sample baseline characteristics aggregated by race and ethnicity and those who had any telehealth prenatal visits and those with only in-person visits. Those with any telehealth prenatal care visits were more likely from the West region and had more prenatal visits overall. Those with only in-person visits had higher percentages of being always insured.
Patient Baseline Characteristics by Any Telehealth Prenatal Care or All In-Person Visits.

Adjusted proportions showed that White Latina women had the lowest percent of telehealth prenatal visits in 2019, 11.3% (95% CI = 11.0, 11.6) (Figure 1, Appendix II). The proportions in 2019 ranged from 11.3 to 13.7 per 100 visits. After 2019, all groups followed a similar trend throughout the study period. Each group rapidly increased in prenatal telehealth proportions until 2021 with a range from 20.5 to 28.5 per 100 visits. In 2023, 25.0% (95% CI = 24.4, 25.6) of non-Hispanic White patients’ prenatal visits were telehealth, whereas for non-Hispanic Black patients it was 20.0% (95% CI = 19.4, 20.5), for Black Latina patients, 18.2% (95% CI = 17.1, 19.4), and White Latina patients, 19.0% (95% CI = 18.9, 19.4). From 2020 through 2023, non-Hispanic White women had higher proportions compared to Latina women and higher than all groups in 2021 to 2023. Non-Hispanic Black women had lower rates than non-Hispanic White women but remained higher than Latina women from 2020 to 2023. In 2019 and 2020, White Latina women had the lowest rates. Unadjusted rates are reported in Appendix III.

Yearly covariate adjusted percent of prenatal visits which were telehealth.
Discussion
While the percentage of prenatal visits delivered using telehealth increased across all racial/ethnic groups in CHCs, non-Hispanic White women had the largest and most rapid increase from 2021 to 2023 followed by non-Hispanic Black women. These results indicate there are still disparities between all racial/ethnic groups. Due to the COVID-19 pandemic, prenatal telehealth visits increased for all groups until 2021, then began to decline. By 2023, telehealth visits were still >5% higher than in 2019. Therefore, while not used as frequently as during the pandemic, telehealth visits were still utilized to access prenatal care more than pre-pandemic rates. Adequate prenatal care can help reduce maternal mortality and morbidity, which is why evaluating these telehealth prenatal care trends is important, especially in racial and ethnic minority populations. 19
Telehealth visits have been shown to increase access to care while reducing both the cost and time associated with appointments.7,10 At the same time, several studies have shown similar, if not better obstetric outcomes.11,12 Given that telehealth may have fewer barriers than in-person visits, new issues may emerge in prenatal telehealth care delivery such as lack of broadband or technology access and digital literacy issues, especially in underserved populations.3,20 These barriers might indicate why non-Hispanic White women had higher percentages of telehealth visits during the pandemic. While we believe this manuscript is novel, our findings do add to the body of literature that indicates non-Hispanic White patients are receiving more telemedicine visits overall when adjusting to demographic factors. 21 It would be an important next step to not only understand overall access to care but also to understand if specific prenatal services (e.g., gestational diabetes screening) are positively or negatively associated with telehealth usage, and whether these associations may result in different outcomes.
Many states and counties have protocols around what type of visits can be conducted via telehealth. 22 The COVID-19 pandemic led to many changes in CHC protocols that led to an increase on visit types that could be conducted via telehealth. The overall increase in prenatal telehealth visit proportions by 2023 could indicate the utility of these visits post-pandemic, as they appear to provide another avenue to access to some aspects of prenatal care. These visits might have fewer barriers than in-person visits (e.g., commuting time, travel costs). 10 CHCs provided telehealth prenatal care consistently between race and ethnicity groups. Future work will help us understand if telehealth prenatal care has uniform effectiveness in all groups, benefiting pregnancy outcomes across many groups.
Limitations
The most significant limitation was the potential for incomplete documentation of prenatal care within a single EHR system. Patients who received care across multiple systems outside the OCHIN network may have had visits that were not captured in the dataset. We may not have identified all “prenatal” visits, as we were limited to ICD codes to define the prenatal part of the visit. Prenatal care can be delivered in other primary care visits (for other chronic conditions or acute illness/injury), and we may not have captured that care. We additionally did not know if the visits were telephone or video, or if patients were required to switch to telehealth by the clinic or provider, or if they made the choice themselves. There may be a stigma against telehealth care if patients believe the quality not equivalent to that of an in person visit. 23 Quality of care for telehealth visits may be limited by technological barriers (e.g., unreliable internet connection for video-based care) or lack of technology literacy. The focus on non-Hispanic White, non-Hispanic Black, and Latina patients provides important insights but does not capture the full spectrum of diversity in CHCs. We did not account for contextual factors such as broadband access and language barriers which may influence telehealth adoption and could explain some observed differences. As an observational study, these findings cannot establish causality between telehealth use and prenatal outcomes.
Conclusion
This study examined trends in telehealth prenatal visits across racial and ethnic groups in a multistate network of CHCs in the US. The study found that while usage increased, notable differences in prevalence persisted among groups. This research emphasizes the critical role of telehealth as a mode of care delivery in ensuring equitable access to prenatal care. Future research should investigate the underlying causes of disparities and assess the impact of telehealth on maternal and neonatal outcomes. By recognizing these differences, CHCs can develop targeted interventions to promote high-quality, effective prenatal care for all populations.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319261422871 – Supplemental material for Trends in Prenatal Telehealth Visits by Race and Ethnicity in U.S. Community Health Centers, 2019 to 2023
Supplemental material, sj-docx-1-jpc-10.1177_21501319261422871 for Trends in Prenatal Telehealth Visits by Race and Ethnicity in U.S. Community Health Centers, 2019 to 2023 by Tahlia Hodes, Jennifer A. Lucas, Brigit Hatch, Gretchen Mertes, John Heintzman and Miguel Marino in Journal of Primary Care & Community Health
Footnotes
Appendix I: Prenatal ICD Codes Used to Identify Prenatal Visits
Supervision of High Risk Pregnancy (O09)
Supervision of Pregnancy with History of Infertility (O09.0)
O09.00, O09.01, O09.02, O09.03
Supervision of Pregnancy with History of Ectopic Pregnancy (O09.1)
O09.10, O09.11, O09.12, O09.13, O09.211
Supervision of Pregnancy with Other Poor Reproductive or Obstetric History (O09.2)
O09.212, O09.213, O09.219, O09.291, O09.292, O09.293, O09.299
Supervision of Pregnancy with Insufficient Antenatal Care (O09.3)
O09.30, O09.31, O09.32, O09.33
Supervision of Pregnancy with Grand Multiparity (O09.4)
O09.40, O09.41, O09.42, O09.43
Supervision of Elderly Primigravida and Multigravida (O09.5)
O09.511, O09.512, O09.513, O09.519, O09.521, O09.522, O09.523, O09.529
Supervision of Young Primigravida and Multigravida (O09.6)
O09.611, O09.612, O09.613, O09.619, O09.621, O09.622, O09.623, O09.629
Supervision of High Risk Pregnancy Due to Social Problems (O09.7)
O09.70, O09.71, O09.72, O09.73
Supervision of Other High Risk Pregnancies (O09.8)
O09.811, O09.812, O09.813, O09.819, O09.821, O09.891, O09.892, O09.893, O09.899
Supervision of Pregnancy with History of Molar Pregnancy (O09/9)
O09.90, O09.91, O09.92, O09.93Encounter For Supervision of Normal Pregnancy (Z34)
Encounter for Supervision of Normal First Pregnancy (Z34.0)
Z34.00, Z34.01, Z34.02, Z34.03
Encounter for Supervision of Other Normal Pregnancy (Z34.8)
Z34.80, Z34.81, Z34.82, Z34.83
Encounter for Supervision of Normal Pregnancy, Unspecified
Z34.90, Z34.91, Z34.92, Z34.93
Acknowledgements
The research reported in this work was powered by PCORnet®. PCORnet has been developed with funding from the Patient-Centered Outcomes Research Institute® (PCORI®) and conducted with the Accelerating Data Value Across a National Community Health Center Network (ADVANCE) Clinical Research Network (CRN). ADVANCE is a Clinical Research Network in PCORnet® led by OCHIN in partnership with Fenway Health, Health Choice Network, Oregon Health & Science University, and University of Washington. ADVANCE’s participation in PCORnet® is funded through the PCORI Award RI-OCHIN-01-MC.
Abbreviations in abstract
CHCs – community health centers
EHR – electronic health record
Ethical Considerations
This study was approved by the Oregon Health and Science University Review Board.
Consent to Participate
This study was approved by the Oregon Health and Science University Review Board, Number: 00025824.
Consent for Publication
Not applicable.
Author Contributions
Tahlia Hodes, designed the study, wrote the paper, conducted the analysis,
Jennifer A Lucas, conception, interpretation, review, proofreading,
Brigit Hatch, conception, interpretation, review, proofreading,
Gretchen Mertes, data acquisition, review, proofreading,
John Heintzman, interpretation, review, proofreading and acquisition of funding,
Miguel Marino, interpretation, review, proofreading,
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institute of Diabetes and Digestive and Kidney Diseases, Grant number: R01DK134514, Recipient: Miguel Marino.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this manuscript were collected as part of routine primary care and consent to use data in research was obtained by the clinics at care initiation. Raw data underlying this article were generated from multiple health systems across the OCHIN network; restrictions apply to the availability and re-release of data under organizational agreements.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.