
Abstract
Background:
The first 2 years of life are a critical period for a child’s development. Early developmental surveillance in motor, language, social-emotional, and emerging cognitive domains plays an essential role in timely intervention and long-term outcomes. Children living in disadvantaged conditions or with acute illness are at higher risk for developmental delays, yet early detection in Vietnam remains limited. A national plan for comprehensive early childhood development has recently emphasized the role of primary healthcare and early interaction guidance.
Objective:
To determine the prevalence and characteristics of developmental delays among hospitalized children aged 2 to 24 months at a tertiary pediatric hospital in Southern Vietnam using the standardized developmental surveillance checklist issued by the Ministry of Health in 2023.
Methods:
We conducted a descriptive cross-sectional study in which clinically stable inpatients were evaluated prior to discharge. Developmental surveillance was performed using the Ministry of Health 2023 developmental surveillance checklist, which covers 4 domains (gross motor, fine motor, language-communication, and social-emotional development) at ages 2-4-6 months, 9 to 12 months, and 15 to 24 months. Children who did not achieve one or more age-appropriate milestones were classified as having suspected developmental abnormalities.
Results:
A total of 939 children aged 2 to 24 months were evaluated. The prevalence and pattern of suspected developmental abnormalities varied by age group. Gross motor and language–communication delays were the most frequent findings. Age-specific inspection revealed that developmental vulnerability was most pronounced at 6 months of age, particularly in gross motor, language–communication, and social–emotional domains, coinciding with a critical period of nutritional and biological transition; at 12 months, 76% could say at least 3 words, and by 18 months, 80.1% could say ≥20 single words. Some 24‑month‑old children had not yet achieved expected motor skills. Anemia and stunting were common, particularly in the 9- to 12‑month group.
Conclusion:
Integrating standardized developmental surveillance into inpatient pediatric care is both feasible and essential. Hospital-based developmental surveillance provides an important opportunity for early detection and referral, and highlights the need to expand screening and follow-up to primary care and community settings in Vietnam.
Introduction
Early detection of developmental disorders plays a vital role in safeguarding the health and future of children as well as the well‑being of their families. It is one of the core responsibilities of pediatricians in daily clinical practice.1-3 When a child shows signs of developmental delay or deviates from the expected developmental trajectory for their age, they are at increased risk for future behavioral and complex neurodevelopmental disorders. Timely identification through routine developmental surveillance allows for effective interventions that can improve long‑term outcomes.4-6
International estimates suggest that approximately 15% of young children experience developmental delays; however, higher rates are expected in low‑ and middle‑income countries where nutritional deficiencies, limited early stimulation, and socioeconomic disparities are common. In Southern Vietnam, particularly in Ho Chi Minh City, no comprehensive study has been conducted over the past decade to evaluate early childhood development in either community or hospital settings. In light of this gap, we conducted the present study to assess physical growth and development among children under 5 years old admitted to Children Hospital.7-9 The findings not only provide necessary data on developmental status but also emphasize the importance of integrating developmental surveillance into pediatric care—an aspect still underemphasized in the current healthcare system.10-12
Methods
Study Subjects
Based on Singh et al, 13 the estimated prevalence of developmental delay in young children is approximately 20%. Sample size was calculated using the formula for estimating a population proportion:

where:
α = 0.05 (type I error)
Z₁ – α/2 = 1.96
P = 0.2 (P = 0.20 was selected based on Singh et al 13 and other studies conducted in low- and middle-income countries, where the prevalence of developmental delay is typically higher than the 15% reported in high-income settings. Given the higher burden of anemia, stunting, acute illness, and socioeconomic disparities in the Vietnamese pediatric population, a prevalence estimate of 20% was considered more appropriate for sample size determination.)
d = 0.05 (margin of error)
Thus, each age group required approximately 246 subjects:
2-4-6 months
9 to 12 months
15 to 24 months
Total N = 738 children (final collected = 939).
Results
General Characteristics
Table 1 summarizes the demographic characteristics of 939 participating children across 3 age groups (2-6 months, 9-12 months, and 15-24 months). Males predominated in all groups (approximately 60%-63%). Most participants were from provinces outside Ho Chi Minh City. Parents’ education was generally at high school level or above, though a minority had low educational attainment. Exclusive breastfeeding rates decreased with age, whereas dietary diversity and use of formula increased.
General Characteristics of the Study Population (N = 939).

Admission Diagnoses
Figure 1 presents the primary admission diagnoses. Pneumonia and bronchiolitis were the most common among infants under 1 year of age (27%-39%), whereas older children were more frequently admitted for asthma or acute diarrhea.

Admission diagnoses by age group.
Health Issues
As shown in Figure 2, anemia was the most prevalent health issue (41% in children aged 9-12 months), followed by dental caries (up to 21.8% in the 15- to 24-month group). Visual and auditory problems were less common but warrant attention during comprehensive pediatric examinations.

Common health problems by age group.
Physical Growth Characteristics
Figure 3 illustrates the nutritional and growth characteristics across age groups. Normal physical development was observed in 55% to 63% of cases. Stunting, indicating chronic undernutrition, ranged from 17% to 32%, highest among children aged 9 to 12 months. Overweight and obesity appeared in 5.3% of participants, reflecting early nutritional transition trends.

Physical growth status by age group.
Developmental Development Characteristics
Table 2 details developmental milestones in infants aged 2 to 6 months. Most achieved visual tracking and social smiling at 2 to 4 months; however, only 58% to 63% could turn toward sound or sit with support at 6 months, suggesting emerging gross motor delays.
Developmental Development in 2-4-6 Months.

Although reported within a combined age cluster, milestone achievement declined progressively with age, with the lowest attainment consistently observed at 6 months. Only 58% to 63% of infants achieved key gross motor, language-communication, and social-emotional milestones at this age, suggesting that 6 months represents a period of heightened developmental vulnerability.
Table 3 summarizes developmental achievements at 9 to 12 months. Nearly all 9-month-olds demonstrated interactive play, object permanence, and babbling. At 12 months, only 76% could say at least 3 words, and 79.8% understood simple phrases early indicators of potential language delay.
Developmental Development in 9- to 12-month-Olds.

As shown in Table 4, at 18 months, 80.1% of children could say at least 20 single words and 95.6% could pronounce 4 consonants. By 24 months, 95% combined 2 words and performed sequential tasks; however, 6% had not yet achieved key motor skills such as running or walking backward.
Developmental Development in 15- to 24-month-Olds.

Screening for Developmental Abnormalities
Table 5 presents the proportion of suspected developmental abnormalities across 4 domains. Fine motor and language-communication delays were most prevalent, especially in the 15- to 24-month group (5.8% and 7.2%, respectively).
Suspected Developmental Abnormalities by Domain.

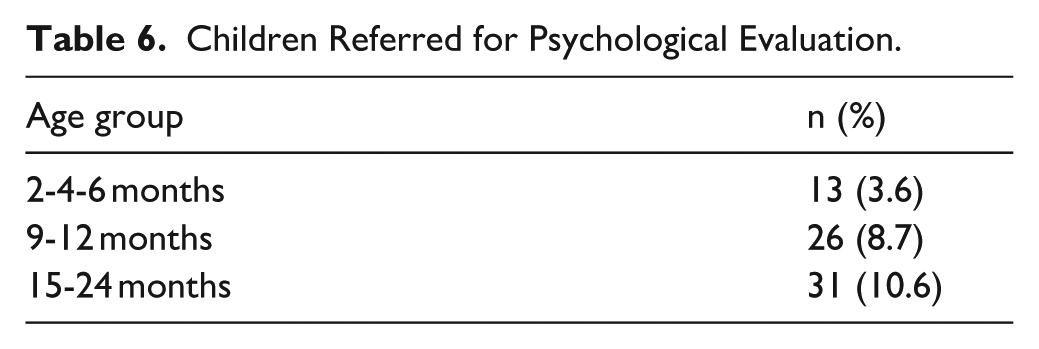
As summarized in Table 6, the need for referral to psychological evaluation increased with age: 3.6% among 2- to 6-month-olds, 8.7% in 9 to 12 months, and 10.6% in 15 to 24 months highlighting the rising detectability of behavioral and communication issues during toddlerhood.
Children Referred for Psychological Evaluation.
Caregiver Interaction and Stimulation Practices
Table 7 outlines observed caregiver-child interactions supporting cognitive development. While affection and appropriate discipline exceeded 95% in all age groups, interactive activities such as talking, playing, and humor markedly decreased among caregivers of 15- to 24-month-olds the most critical stage for language and social development.
Observed Caregiver Practices Supporting Cognitive Development.

Discussion
Notably, 6 months of age emerged as a critical developmental inflection point in this cohort. Although developmental milestones were reported within a combined 2-4-6-month age cluster, age-specific inspection revealed that developmental vulnerability was most pronounced at 6 months, particularly in gross motor, language-communication, and social-emotional domains. Early developmental surveillance in this inpatient cohort identified delays across all domains of development. Delays in language-communication and fine motor skills were particularly prominent, especially among toddlers aged 15 to 24 months. At 6 months, only around 60% of infants achieved key gross motor and social milestones, and at 12 and 18 months, the proportions of children who met expected expressive language milestones were lower than reference values from middle‑ and high‑income settings. These findings support global evidence that hospitalized and medically vulnerable children are at heightened risk of developmental delay.
Our results must be considered in the context of the tool used. The Ministry of Health 2023 developmental surveillance checklist was designed for routine use in Vietnamese primary care and hospital settings. 11 It covers gross motor, fine motor, language-communication, and social-emotional domains, similar to widely used instruments such as the Ages and Stages Questionnaire (ASQ). 9 However, unlike the ASQ, the MoH checklist does not contain a discrete cognitive domain. This is an important limitation, as cognition is a core component of early development. Some items within the language, fine motor, and social-emotional domains—for example, object permanence, problem solving behaviors, imitation, and following commands—indirectly reflect cognitive skills, but they do not replace a structured cognitive scale. Future research should explore concurrent administration of the MoH checklist with validated tools such as ASQ or Bayley Scales to establish sensitivity, specificity, and optimal cut‑offs for Vietnamese children.1,2,9,10
The study population consisted entirely of hospitalized children, which introduces selection bias. Children admitted with acute illnesses, anemia, malnutrition, or chronic conditions are more likely to have developmental vulnerabilities than children in the general community. Moreover, we did not exclude children with prematurity or those admitted to specialty units such as cardiology or neonatology, where the baseline risk of developmental delay is known to be higher. These factors may partly explain why the estimated prevalence in our cohort approaches or exceeds the 15% rate commonly cited in high‑income countries. At the same time, this inpatient focus is clinically important: hospitalization provides a unique opportunity to conduct developmental surveillance and initiate referrals at a time when families are already engaged with healthcare services.3,5,6,8
Nutritional and health indicators in this study further support the link between biological risk factors and development. This period coincides with several important biological and environmental transitions, including depletion of prenatal iron stores, initiation of complementary feeding, and increased susceptibility to infection. Early nutritional vulnerability, particularly iron deficiency, likely represents a central mechanism underlying the developmental delays observed around 6 months of age. Anemia was extremely common among 9- to 12‑month‑olds (41%) (Figure 2), and stunting affected up to one‑third of children in some age groups, mirroring national nutrition survey data. Both conditions have been associated with poorer cognitive, motor, and socioemotional outcomes in previous research. Although our analyses were primarily descriptive, developmental delays were more frequently observed in children with anemia and stunting, suggesting that integrated programs combining nutritional interventions with developmental surveillance and caregiver education are needed.
Caregiver practices observed in this cohort highlight both strengths and areas for improvement. Most caregivers showed warmth, affection, and appropriate discipline; however, interactive behaviors such as talking, playing, and teaching decreased markedly in the second year of life the most critical period for language and socioemotional growth. These findings are consistent with models of early childhood development that emphasize responsive caregiving and rich language input as key drivers of developmental outcomes. In practice, developmental surveillance should be coupled with brief, structured counseling sessions that provide parents and caregivers with concrete strategies to play, communicate, and respond sensitively to their child. Importantly, many children demonstrated developmental catch-up by 24 months of age, suggesting that early delays are not necessarily permanent and may be responsive to timely nutritional support, caregiver education, and early intervention strategies. Where possible, families should be linked to community nurses or early childhood services for follow‑up after discharge.7,9
This study has several limitations. First, its descriptive cross‑sectional design precludes causal inference and does not allow us to determine whether early delays persist, resolve, or progress over time. Second, the inpatient sample is not representative of the general population of Vietnamese children and likely overestimates the prevalence of developmental delay. Third, although the MoH developmental surveillance checklist and caregiver interaction checklist are nationally recommended, they have not yet undergone formal psychometric validation against gold‑standard developmental assessments. Finally, systematic follow‑up after hospital discharge was not available for all children, so we could not fully document referral completion or subsequent interventions. Future studies should incorporate community‑based sampling frames, validated developmental and cognitive tools, and longitudinal follow‑up to clarify trajectories and intervention effects.
Conclusion
Developmental delays were observed across gross motor, fine motor, language-communication, and socioemotional domains among hospitalized children aged 2 to 24 months, in the context of high rates of anemia, stunting, and suboptimal caregiver stimulation. Integrating standardized developmental surveillance into pediatric inpatient care proved feasible and provided an important first step toward early detection and referral. The identification of 6 months as a critical developmental transition point underscores the need for early, proactive developmental surveillance rather than delayed wait-and-see approaches. This study contributes new evidence on early childhood development in Vietnam and underscores the need to extend developmental surveillance and family‑centred interventions to primary care and community settings to improve long‑term outcomes.
Footnotes
Acknowledgements
The authors are grateful to the University of Health Sciences, Vietnam National University Ho Chi Minh City, for providing institutional and time support for this study.
We also thank Children’s Hospital 1 in Ho Chi Minh City, Vietnam, for clinical collaboration and data collection support.
Ethical Considerations
The study was approved by the Institutional Ethics Committee of Children’s Hospital 1, Ho Chi Minh City, Vietnam.
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and national research committees.
Consent to Participate
Written informed consent was obtained from the parents or legal guardians of all patients included in this study.
Author Contributions
Ho Quang Minh Phuc contributed to study design, data analysis, and manuscript revision.
Nguyen Tan Thinh and Tran Thanh Minh participated in data collection, data verification, and clinical supervision.
Nguyen Thanh Hung, Quan Thuy Tien, and Nguyen Hoang Thien Huong contributed to clinical data collection, patient management.
All authors read and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Vietnam National University Ho Chi Minh City (VNU-HCM) under grant number C2024-44-03.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Trial Registration
Not applicable.