
Abstract
Financial incentives are a promising strategy to promote physical activity. While randomized trials in Western countries have demonstrated short-term effectiveness, evidence from non-Western settings remains limited. This rapid review synthesized evidence from Japan on financial incentive-based interventions considering both individual-level behavioral responses and their use as policy tools implemented by administrative organizations. A systematic search of 4 databases (CiNii Articles, PubMed, Google Scholar, and Ichushi Web) was conducted between May and June 2025, covering English and Japanese studies. Intervention characteristics were described using the TIDieR checklist and step count changes were extracted. Where necessary, healthcare cost savings and return on investment (ROI) were also estimated. Fourteen studies (11 peer-reviewed and 3 gray literature) were included. Most interventions used redeemable points or gift certificates as incentives, with daily values ranging from ¥11 to ¥100. On average, interventions increased daily step counts by 997 steps and reduced annual medical expenditures by ¥28 425, yielding an average ROI of 5.67. Effects were consistent across population subgroups and incentive types. Only 1 study reported post-intervention sustainability, which concluded that step increases were not maintained after receiving the incentive. Low-cost financial incentives have the potential to increase physical activity and reduce healthcare costs in Japan. Further long-term and cost-effectiveness studies are warranted to support sustainable health policy design.
Introduction
Physical inactivity is a leading risk factor for noncommunicable diseases (NCDs), such as heart disease, stroke, type 2 diabetes, and colonic cancers, which imposes a considerable economic burden through increased healthcare expenditures and productivity losses. According to the World Health Organization (WHO), sedentarism accounted for an estimated INT$54 billion in global healthcare costs in 2013, along with an additional INT$14 billion in productivity losses. 1 Despite growing awareness of its health benefits, physical activity levels remain insufficient worldwide. As of 2010, 23% of adults and 81% of adolescents did not meet WHO recommendations for physical activity. 1 In Japan, the number of daily steps has significantly declined over the past decade, averaging 6628 steps per day for men and 5659 for women in 2023. 2 Among various forms of physical activity, walking is a particularly accessible and safe behavior that can be readily incorporated into daily life.
Public health strategies have increasingly turned to the field of behavioral economics. One promising approach involves the use of financial incentives to encourage healthier choices. 3 Previous randomized controlled trials and meta-analyses conducted primarily in Western settings have demonstrated that monetary incentives can increase physical activity, although effects are often modest and short-term. For example, a meta-analysis of 23 randomized controlled trials reported an average increase of 607 steps per day associated with financial incentive interventions. 4
However, key challenges remain. The long-term sustainability of incentive-driven behavior change is still unclear, and existing studies offer limited evidence on the durability of physical activity once the incentives are withdrawn. 5 Moreover, most prior studies has been conducted in controlled trial settings, with relatively little evidence from real-world implementations. 5 In addition, evidence from non-Western settings remains scarce.
Japan presents a compelling case for further investigation. A growing number of local governments have introduced financial incentive programs to encourage walking. However, these initiatives are poorly included in international meta-analyses, due to language bias and the prevalence of gray literature sources. 5
The aim of this rapid review was to examine the use of financial incentive-based interventions for walking promotion in Japan, considering both individual-level behavioral responses and their use as policy tools implemented by administrative organizations. To our knowledge, it is the first review to synthesize domestic evidence, including both peer-reviewed and gray literature. By applying the GRADE framework 6 and using the TIDieR checklist, 7 we sought to evaluate the reproducibility and public health significance of these programs.
Methods
Search Strategy
Study Design
This study was conducted as a rapid review to provide a timely, policy-relevant synthesis of evidence on financial incentive–based physical activity interventions in Japan, where relevant data are dispersed across peer-reviewed publications and gray literature and have not been systematically integrated.
Unlike scoping reviews, which are primarily exploratory, this review applied predefined eligibility criteria, structured data extraction, outcome harmonization, and formal certainty-of-evidence assessment using the GRADE framework, enabling interpretation of intervention effectiveness and potential cost implications.
In accordance with rapid review methodology, screening was conducted by a single reviewer with independent verification, and findings were synthesized narratively without meta-analysis.
We conducted a rapid review to identify intervention studies conducted in Japan that utilized financial incentives to promote physical activity, particularly walking. The literature search was carried out between May 7 and June 1, 2025, using multiple databases and sources, including CiNii Articles, PubMed, Google Scholar, and Ichushi Web. For the search, we used a combination of English and Japanese keywords. The English search terms included: (“Japan”) AND (“Financial Incentive” OR “Reward”) AND (“Physical Activity” OR “Walking” OR “Step Count”). The Japanese keywords used were: (日本) AND (金銭的インセンティブ OR ポイント OR 報酬) AND (健康行動 OR 歩行 OR 身体活動). Additionally, we used broader terms in Google Scholar searches, such as “Japan incentive health behavior walking” and “日本 金銭的インセンティブ 身体活動 歩行.”
In addition to peer-reviewed publications which were screened by their titles, gray literature was also considered. Gray literature was identified through reference chaining and a structured web search targeting Japanese municipal and governmental sources, including official local government websites and publicly available program reports. Searches were conducted using predefined Japanese keywords described above and retrieved documents were screened using the same eligibility criteria as peer-reviewed studies.
Due to resource constraints, the screening of articles was conducted by 1 reviewer, while a second reviewer independently verified the eligibility and data extraction of the included studies.
Inclusion and Exclusion Criteria
We applied specific inclusion and exclusion criteria to identify relevant studies. Studies were included if they were conducted in Japan and involved interventions that provided financial incentives, such as cash, points, or gift cards. To be eligible, studies needed to report objective and quantitative outcomes related to physical activity, such as step count, walking time, or healthcare cost reduction. We included both single-arm studies that compared outcomes before and after the intervention within a treatment group, as well as controlled studies that compared intervention and control groups. Additionally, we considered studies based on primary data, including posters or reports, as long as they contained usable data.
Studies were excluded if they were conducted outside of Japan or if the interventions did not involve financial incentives. For example, studies based solely on education or gamification were excluded. We also excluded studies that did not report outcomes related to physical activity, or that lacked extractable quantitative outcomes, namely studies that only reported self-reported satisfaction or preference-based results. Finally, studies were excluded if the incentive conditions could not be meaningfully compared, such as when financial incentives were provided to both the intervention and control groups.
Data Extraction
We extracted several variables from each included source. These included the author and year of publication, the study design, and whether a control group was present. We also recorded the total sample size, as well as the sizes of the intervention and control groups separately. Additional information collected included the duration of the study, participant age, and baseline activity levels. We noted the type of financial incentive used, such as cash, points, or gift cards, as well as the size and structure of the incentive. Furthermore, we identified whether the reward was lottery-based or guaranteed, the timing of the incentive delivery (ie, whether it was provided immediately or with a delay), and the outcomes reported by each study.
Evidence Assessment (GRADE)
Each study was evaluated using the GRADE framework across 5 domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. An overall rating (High, Moderate, Low, or Very Low) was assigned for each study based on the overall assessment.
Outcomes and Analytical Approach
The primary outcomes of interest were changes in daily step count and the impact on healthcare expenditures. To analyze these outcomes, we employed several methods. First, we calculated the daily monetary value of incentives provided in each intervention. We then conducted a descriptive synthesis of changes in step count reported across studies. In cases where physical activity changes were reported using ordinal self-reports rather than precise counts, we converted these into continuous step estimates as follows: a reported decrease was interpreted as −500 steps; no change was recorded as 0 steps; an increase of 0 to 1000 steps was estimated as 500 steps; an increase of 1000 to 2000 steps as 1500 steps; and an increase of more than 2000 steps as 2500 steps. When walking time rather than step count was reported, we converted it to steps using a rate of 100 steps per minute, following the method described by Fujihara et al. This method is also consistent with prior cadence-based studies indicating that approximately 100 steps per minute corresponds to average-paced or moderate-intensity walking in adults. 8
These conversions were used to facilitate descriptive comparison across heterogeneous studies rather than to derive precise estimates of physical activity. Assigned step-count values represent conservative midpoint approximations within reported categories and were applied consistently across studies in the absence of standardized outcome reporting.
To estimate medical cost savings, we applied a conversion rate of ¥0.0685 per step, based on a document from the Ministry of Land, Infrastructure, Transport, and Tourism. 9 The healthcare cost reduction estimates represent reductions in insurer-level healthcare expenditures based on population-average medical costs, rather than directly observed changes in individual out-of-pocket spending.
Return on investment (ROI) was defined as the ratio of daily medical cost savings to the daily incentive amount. We also calculated the number of steps gained per ¥1000 in incentives to evaluate cost-effectiveness. In addition, cost-effectiveness was assessed by calculating the number of steps gained per ¥1000 of incentives provided.
We also conducted a descriptive subgroup analysis to explore potential differences in intervention effects according to the type or implementation of financial incentives. Due to the heterogeneity and limited number of studies, we did not perform formal statistical testing. Each intervention was also systematically described using the Template for Intervention Description and Replication (TIDieR) checklist.
Results
Study Selection
A total of 1538 records were identified through database searches: CiNii Articles (Japanese) yielded 15 records, CiNii Articles (English) 611 records, PubMed 40 records, and Google Scholar 872 records (443 in English and 429 in Japanese). Following title and abstract screening, 43 records were identified and after removing 7 duplicates, 36 articles underwent full-text eligibility assessment. In addition, 2 peer-reviewed articles and 3 gray literature sources were identified by hand-searching. Ultimately, 14 studies were included in the final analysis (Figure 1).
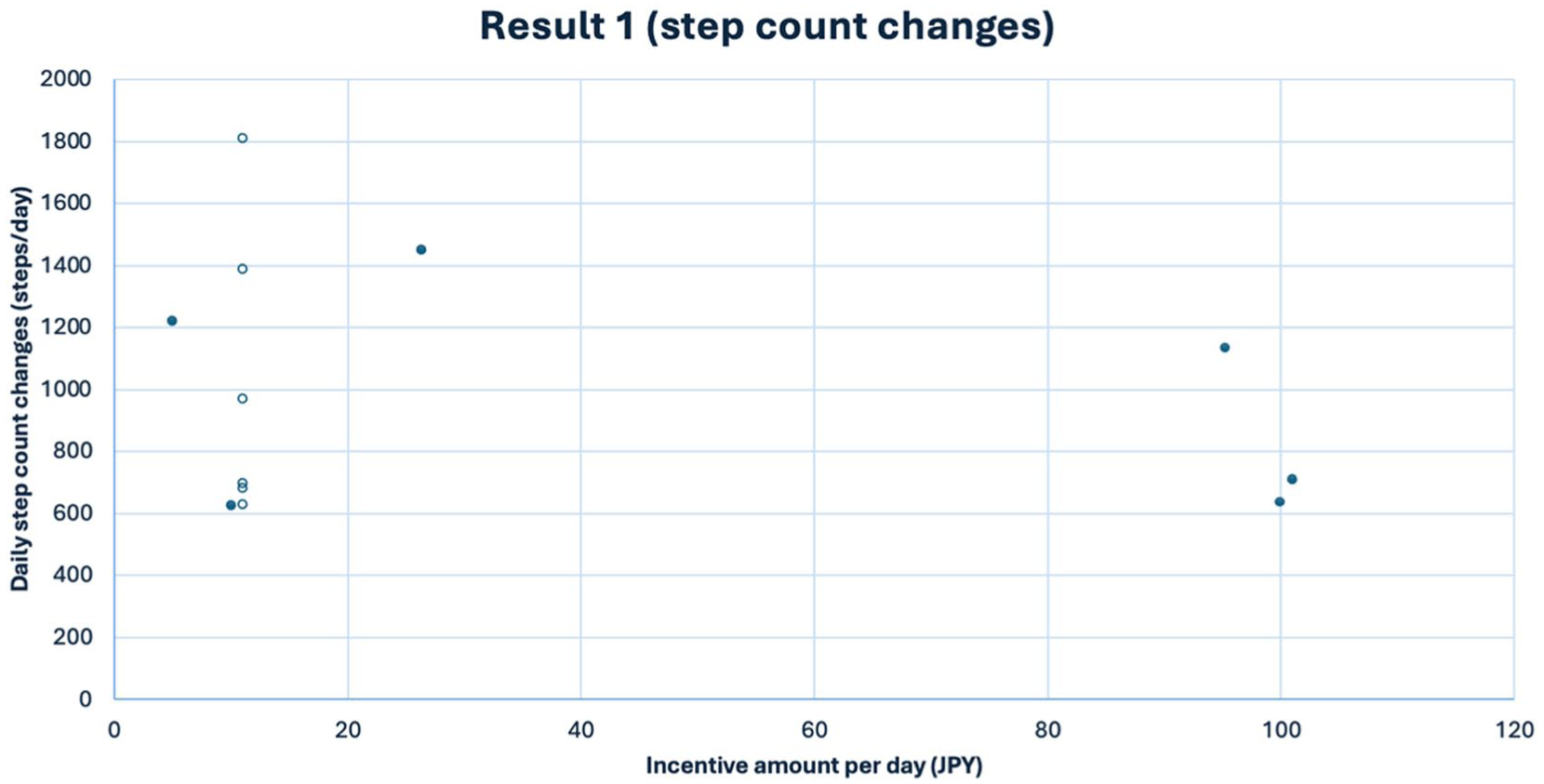
Relationship between incentive amount per day and daily step count changes. Each point represents an intervention study. Open circles indicate programs from the Yokohama Walking Point project, and filled circles indicate other programs.
Characteristics of Included Studies
Among the 14 included studies, 11 were peer-reviewed publications, and 3 were gray literature reports issued by municipal or governmental organizations. The study designs varied, comprising 2 randomized controlled trials, 11 non-randomized intervention studies including a control group and 1 pre-post analysis (Table 1).
Overview of Study Characteristics.
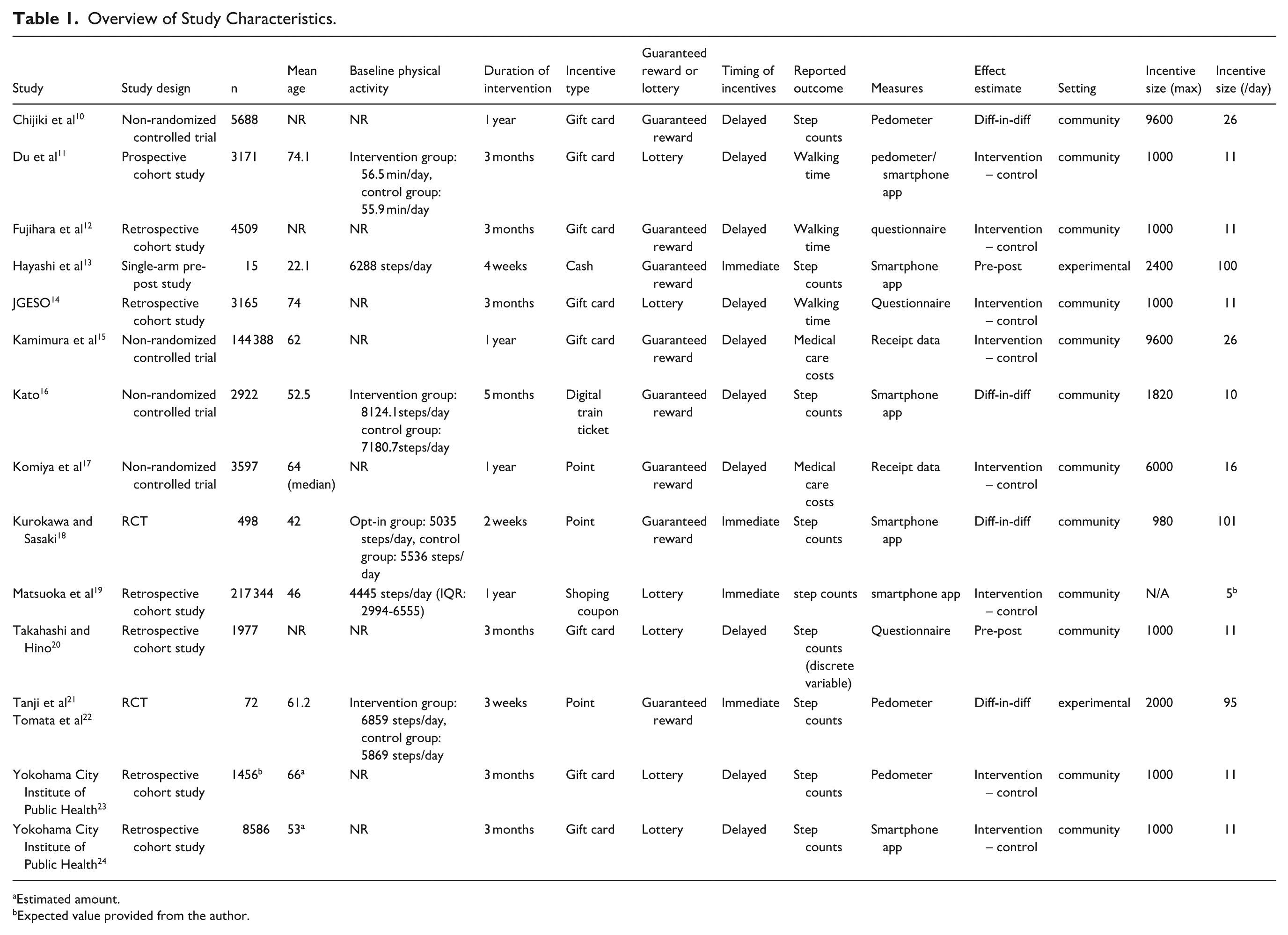
Estimated amount.
Expected value provided from the author.
Characteristics of Interventions
Using the TIDieR framework, we summarized key features of the financial incentive interventions (Supplemental Table 1). The form of incentives included point-based rewards redeemable for goods or services (n = 3), direct cash incentives (n = 1), shopping coupons (n = 1), and gift certificates (n = 8). Daily incentive values ranged from approximately ¥10 to ¥100 per participant. All interventions utilized step count data, primarily obtained through pedometers or smartphone applications. In 6 studies, incentives were awarded proportionally based on step counts, while 4 used pre-defined goals as criteria. In 1 study, incentive criteria were not clearly stated.
Effects on Step Count Outcomes
Of the 14 studies, 12 reported outcomes related to step count or walking time. Among these, 11 showed a statistically significant increase in physical activity. When available, difference-in-difference estimates were prioritized; otherwise, pre-post changes or group comparisons were used.
Across studies, the average increase in step count was 997 steps per day. The average reduction in annual medical expenditure was ¥28 425, and the return on investment (ROI) was 5.67. On average, each ¥1000 of total financial incentive during the intervention period was associated with an increase of 748 steps. Detailed quantitative outcomes are presented in Supplemental Table 2 and Figure 1. There was no consistent correlation observed between the monetary value of incentives and the magnitude of behavioral change.
Healthcare Cost Outcomes
Two studies examined healthcare expenditures using administrative data. One study reported a significant reduction in total annual medical expenses. The other study observed significant reductions only in specific subgroups; older adults and female participants. Notably, these 2 studies estimated higher cost-saving effects compared to studies that inferred cost reductions from physical activity metrics.
Quality of Evidence (GRADE)
Based on the GRADE assessment, 2 studies were rated as “high” quality, 5 as “low,” and 7 as “very low.” The most frequently downgraded domain was indirectness (n = 5), primarily due to variations in intervention components or unclear outcome attribution (Supplemental Table 3).
Subgroup Analysis
We conducted a descriptive subgroup analysis to explore potential differences in intervention effects (Supplemental Table 4). Among studies targeting older adults (n = 9), the average increase in daily steps was 998 steps per day, compared to 1000 steps per day in studies targeting the general population (n = 5). Difference-in-differences studies (n = 4) reported a mean increase of 980 steps per day, whereas studies using pre-post or between-group comparisons (n = 10) reported a slightly higher increase of 1004 steps per day. Short-term interventions (n = 4) were associated with a lower average increase of 827 steps per day, compared to 1053 steps per day in mid- to long-term interventions (n = 10). Interventions that provided immediate incentives (n = 4) resulted in a mean increase of 925 steps per day, while those that delivered incentives with a delay (n = 10) led to an average increase of 1032 steps per day. Studies that used pedometers or smartphone applications to monitor physical activity (n = 8) reported a mean increase of 962 steps per day, whereas those relying on questionnaire-based self-reports (n = 6) reported a slightly higher increase of 1030 steps per day. Estimated annual healthcare cost reductions based on step counts (n = 9) amounted to ¥24 915 per year, whereas studies using actual healthcare expenditure data from insurance receipts (n = 2) reported a higher estimated reduction of ¥49 489 per year. Finally, university-based studies (n = 2) reported a mean step increase of 886 steps per day, compared to 1019 steps per day in community-based studies (n = 12).
Additional Observations
Some gray literature reports from the Ministry of Health, Labour and Welfare described healthcare cost reductions from 5 incentive programs; however, due to insufficient information on intervention details, these studies were excluded from the analysis. Only 1 study recorded step count changes after incentives were removed.
Discussion
Summary of Key Findings
Across the 14 studies, average increases in daily steps amounted to 997 steps per day, with a mean of 748 steps per ¥1000 incentive provided during the whole intervention period. This observed effect is somewhat higher than the pooled mean difference reported in previous meta-analyses conducted in Western contexts, which reported a mean increase of 607.1 steps per day (95% CI, 422.1-792.1) during the intervention period. 4 However, most of the studies were not randomized trials, and participants opted in to the incentive schemes, which may have caused selection bias and contributed to the larger effect sizes observed in our review.
Interestingly, the amount of financial incentives within the observed range of ¥10 to ¥100/day did not correlate with the magnitude of step count increases. Several interventions demonstrated sustained effects over the medium to long term (around 1 year). The interventions targeted diverse populations across multiple regions of Japan, and subgroup analyses generally showed consistent effects across population sub-groups.
These findings align with existing literature, reinforcing evidence that financial incentives have the potential to increase physical activity. This review also contributes important new evidence regarding the effectiveness of longer-term interventions, which have been scarce in prior research. Some programs, such as Yokohama Walking Program, included gamification elements and community-based health events, 12 which may have helped sustain engagement and contributed to long-term effectiveness. Given Japan’s aging population and rising healthcare costs, these findings underscore the feasibility and policy relevance of financial incentive programs in reducing healthcare expenditures.
Comparison With Prior Research
Overall, this review uniquely captures Japanese-language and gray literature, filling a gap in global evidence. Unlike previous systematic reviews and meta-analyses, which focused primarily on RCTs, this review included observational studies and gray literature, enabling the inclusion of municipality-led and longer-term interventions. While prior studies suggested that higher incentive amounts increase adherence to activity goals, 25 our findings indicate that step count increases were not significantly associated with incentive size within the range offered in the Japanese studies (between $0.07-0.7/day). We hypothesize that the mere offer of an incentive, rather than its value, may be the primary driver of behavior since many interventions did not specify daily incentive amounts when recruiting participants.
Short-term increases in step counts following financial incentives have also been reported in Western contexts and our results align with those findings. 4 In addition, the present review suggests that increased physical activity can be maintained during longer incentive periods, with several programs demonstrating sustained step-count increases while incentives remained in place for up to 1 year. In contrast, evidence regarding behavioral maintenance after incentive withdrawal is very limited as only 1 study in this review assessed post-intervention step counts.
Previous studies have emphasized the importance of incentive size and intervention duration and have recommended incentives of about $1/day.4,26 In contrast, our review suggests that incentives as low as ¥10/day (~$0.07) can still yield meaningful increases in physical activity in Japan.
Concerns have also been raised about the cost-effectiveness of such programs, noting that the cost per MET-hour gained may exceed the estimated healthcare cost savings. 5 However, in Japan, multiple municipalities report that their incentive-based programs with relatively lower per-person incentive costs still succeeded in achieving reductions in healthcare spending that exceeded the cost of the intervention. These claims warrant further investigation through a formal cost-effectiveness analysis.
Most interventions used redeemable points rather than cash, but no clear difference in effectiveness was observed. One intervention did not find significant step increases 13 ; this may be because its incentive targeted moderate-to-vigorous physical activity, not walking specifically.
Implications for Practice and Policy
These findings offer practical guidance for municipalities, employers, and health ministries. Daily incentives as small as ¥10 may be sufficient to increase walking and reduce medical costs. Since some lottery-based programs achieved comparable results, expected incentive value could be reduced further. Programs offering ¥100/day did not produce proportionally greater effects, implying similar returns at higher amounts.
One included study suggested that financial incentives may also promote other health-related behaviors, and that integrating gamification elements could support longer-term engagement. 27 The widespread adoption of smartphones has also lowered technical barriers to program delivery, including real-time reward distribution which was shown to enhance effectiveness but was previously difficult.
Return on investment (ROI) analyses from most included studies exceeded 1. Notably, the few studies with ROI below 1 tended to use large incentive amounts, suggesting that cost-effective design is achievable by adjusting reward levels.
Strengths and Limitations
This review has several strengths: it incorporates Japanese-language publications, applies TIDieR and GRADE frameworks to evaluate intervention fidelity and evidence quality, and includes observational studies and gray literature. However, there are some limitations. First, the majority of studies received a “fair” or “poor” quality grade; many included studies were not RCTs, and risk of bias could not be formally assessed. Second, due to inconsistent outcome reporting (eg, pre-post vs control-intervention comparisons) and inadequate data extracted (standard deviations and confidence intervals), a quantitative analysis was not feasible. Moreover, 6 of the 14 studies were based on Yokohama Walking Program, a municipal project in Yokohama City, Kanagawa Prefecture, in which participants were entered into a lottery for gift cards based on their daily step counts. Some involved post-hoc comparisons based on lottery wins. Lastly, some studies also included incentives for activities other than walking (eg, participation in health promotion events), making it difficult to isolate the effects of step-based incentives alone, making it difficult to isolate the effects of step-based incentives alone. In addition, the literature screening was primarily conducted by a single reviewer, which may have introduced selection bias despite subsequent verification of the extracted studies by another reviewer.
Future research should include cost-effectiveness analyses and implementation studies, particularly those leveraging real-world data from municipalities. While RCTs have been extensively conducted in other countries, Japan would benefit from greater transparency and publication of anonymized walking and healthcare data. More long-term follow-up studies are also needed to evaluate sustained effects after incentive programs end. Additionally, estimates of expected value and variance (eg, in lottery-based interventions) are lacking and merit further policy implications.
Conclusion
This rapid review suggests that financial incentive programs conducted in Japan were associated with increased physical activity and may contribute to reducing healthcare expenditures. Even low-cost interventions may yield meaningful behavioral changes, particularly when integrated with gamification or community-based health activities.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319261415805 – Supplemental material for Financial Incentives to Promote Physical Activity in Japan: A Rapid Review
Supplemental material, sj-docx-1-jpc-10.1177_21501319261415805 for Financial Incentives to Promote Physical Activity in Japan: A Rapid Review by Koki Aoki and Ichiro Kawachi in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors would like to thank colleagues who provided helpful comments on the conceptualization of this review. No professional writing assistance was used.
Ethical Considerations
Not applicable. This study is a rapid review of publicly available literature and did not involve human participants, human data, or human tissue.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Not applicable. This study is based on previously published literature and does not include new dataset.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.