
Abstract
Introduction:
Uncontrolled hypertension is a leading global public health concern, contributing significantly to cardiovascular disease burden and premature mortality. Crucially, insufficient patient health literacy often underlies poor blood pressure management. Enhancing health literacy therefore offers substantial potential to empower patients, foster beneficial health behaviors, and ultimately achieve effective blood pressure control.
Objective:
To evaluate the effects of a health literacy promotion program on health behaviors and systolic and diastolic blood pressure levels in patients with uncontrolled hypertension.
Methods:
This quasi-experimental study employed a 2-group pretest-posttest design with 50 patients diagnosed with uncontrolled hypertension. It was conducted at a subdistrict health promoting hospital in Phayao Province, Thailand. Participants were randomly assigned to either an experimental or a control group, with 25 individuals in each. The control group received usual care, while the experimental group participated in a 12-week health literacy promotion program. This intervention comprised small-group activities incorporating the Teach-back method, Ask Me 3, and motivational interviewing, supplemented by home-based phone calls. The program aimed to develop 6 key health literacy skills. Data were analyzed using descriptive statistics, chi-square test, Fisher’s exact test, Mann-Whitney U test, paired t-test, independent t-test, and ANCOVA.
Results:
The experimental group showed a significant increase in health behavior scores by 8.72 points post-program (95% CI: 6.61, 10.82; P < .001). This increase was 9.52 points greater than that observed in the control group (95% CI: 6.46, 12.58; P < .001; Cohen d = 1.77). Systolic blood pressure decreased by 14.00 mmHg post-program (95% CI: −17.82, −10.18; P < .001). The between-group difference in reduction was −6.97 mmHg (95% CI: −13.33, −0.60; P = .033, Partial η2 = 0.094), indicating a significantly larger reduction in the experimental group. Although diastolic blood pressure decreased by 10.24 mmHg post-program (95% CI: −13.72, −6.76; P < .001), this change did not significantly differ from the control group (P = .387).
Conclusions:
The health literacy promotion program significantly improved health behaviors and reduced systolic blood pressure, suggesting its feasibility for implementation in primary care settings. Future research should employ larger sample sizes and extended follow-up periods to thoroughly examine the program’s long-term effectiveness across diverse populations.
Keywords
Introduction
Hypertension is a chronic non-communicable disease and a major global public health concern. In 2024, approximately 1.4 billion adults aged 30 to 79 years worldwide were living with hypertension; however, only 320 million (23%) had their condition controlled. 1 In Thailand, hypertension control remains a significant challenge, with a study from 2004 to 2020 revealing that only 22.72% of patients achieved target blood pressure control, 2 reflecting a substantial gap in disease management. To address this, the World Health Organization (WHO) set a goal to reduce the prevalence of uncontrolled hypertension by 25% between 2010 and 2025. 1 Further highlighting its importance, improved hypertension control between 2023 and 2050 could prevent 76 million cardiovascular deaths, 120 million strokes, 79 million acute myocardial infarctions, and 17 million cases of heart failure. 3 These projections underscore the significant benefits of enhancing hypertension control.
Effective hypertension control necessitates adopting appropriate health behaviors, including weight reduction for individuals who are overweight or obese, healthy dietary intake, salt and sodium restriction, increased physical activity, stress management, limiting or abstaining from alcohol consumption, smoking cessation, and consistent adherence to prescribed medications.4-6 However, modifying health behaviors for hypertension prevention and control requires adequate health literacy. 7 Health-promoting behaviors have been found to correlate significantly and positively with health literacy (r = .927, P < .001). 8 Moreover, hypertensive patients with high levels of health literacy tend to achieve better health outcomes and are more likely to effectively control their blood pressure. 9
Health literacy encompasses a set of cognitive and social skills that shape an individual’s motivation and ability to access, understand, and apply health information to plan and modify health behaviors. Achieving health literacy requires 6 key skills: First, access refers to the ability to locate pertinent health information. Second, cognitive processing involves understanding health knowledge and diseases to correctly apply self-care or appropriate health behaviors. Third, communication is the ability to convey health information and practices that promote well-being. Fourth, self-management highlights the capacity to set goals and plan suitable health behaviors. Fifth, media literacy signifies the skill to critically analyze the credibility of health media, thereby preventing potential health risks. Finally, decision-making is the ability to choose appropriate actions that support good health. These skills foster functional, interactive, and critical health literacy. Individuals must possess adequate health literacy and competence to apply knowledge and communication skills to engage in sustainable health behaviors.10,11 Those with low health literacy often exhibit poor self-care management 12 and are 2.06 times more likely to have uncontrolled blood pressure compared to those with high health literacy. 13
Prior studies consistently show inadequate health literacy levels among patients with hypertension. For instance, a study of patients with uncontrolled hypertension at a Chicago community health center revealed that 47.4% had low health literacy, 33.2% had possibly limited health literacy, and only 19.4% had high health literacy. 14 Similarly, a study on Dominican patients with hypertension in Northern Manhattan’s Washington Heights/Inwood community reported 84.9% with low health literacy. 15 In Hamadan province, a study conducted at comprehensive urban health service centers revealed that 50.5% of patients had uncontrolled hypertension, and their mean health literacy score was significantly lower than that of the controlled hypertension group (P < .001). 16 Similarly, a study at a municipal public health center in Map Ta Phut, Thailand, indicated that 83.2% of patients with hypertension had low health literacy. 17 Furthermore, a comparative study at a subdistrict health promoting hospital in Phayao province observed that patients with controlled hypertension exhibited high health literacy, whereas those with uncontrolled hypertension had low health literacy. 18
Collectively, these studies indicate that most patients with hypertension have low health literacy and poor blood pressure control, whereas those with high health literacy achieve better disease control. Therefore, developing a health literacy promotion program is essential. The program utilized in this study integrated strategies such as the Teach-back method, Ask Me 3, motivational interviewing, and participatory group activities. These strategies aimed to enhance 6 key skills for promoting health literacy, ultimately fostering the adoption of appropriate health behaviors. To date, few studies have examined the implementation of multi-strategy programs designed to improve health literacy for addressing uncontrolled hypertension. This study aimed to examine the effects of a health literacy promotion program on health behaviors and blood pressure levels among patients with uncontrolled hypertension. Outcomes were compared pre-program and post-program, and between experimental and control groups. These findings will provide important empirical evidence for developing effective hypertension care models and facilitating their clinical application.
Methods
Conceptual Framework
This study utilized Nutbeam’s health literacy conceptual framework10,11 as the foundation for developing a health literacy promotion program. The program integrates diverse strategies designed to enhance 6 essential skills across 3 distinct levels of health literacy: (1) functional health literacy, referring to the basic ability and skills to access health information, including understanding and following recommendations relevant to a disease condition; (2) interactive health literacy, which encompasses the ability to use communication skills to comprehend health information and apply it to self-care; and (3) critical health literacy, describing the ability to think analytically to manage health within one’s own context. The ultimate goal is to equip patients with uncontrolled hypertension to adopt appropriate health behaviors and effectively control their blood pressure levels (see Figure 1).
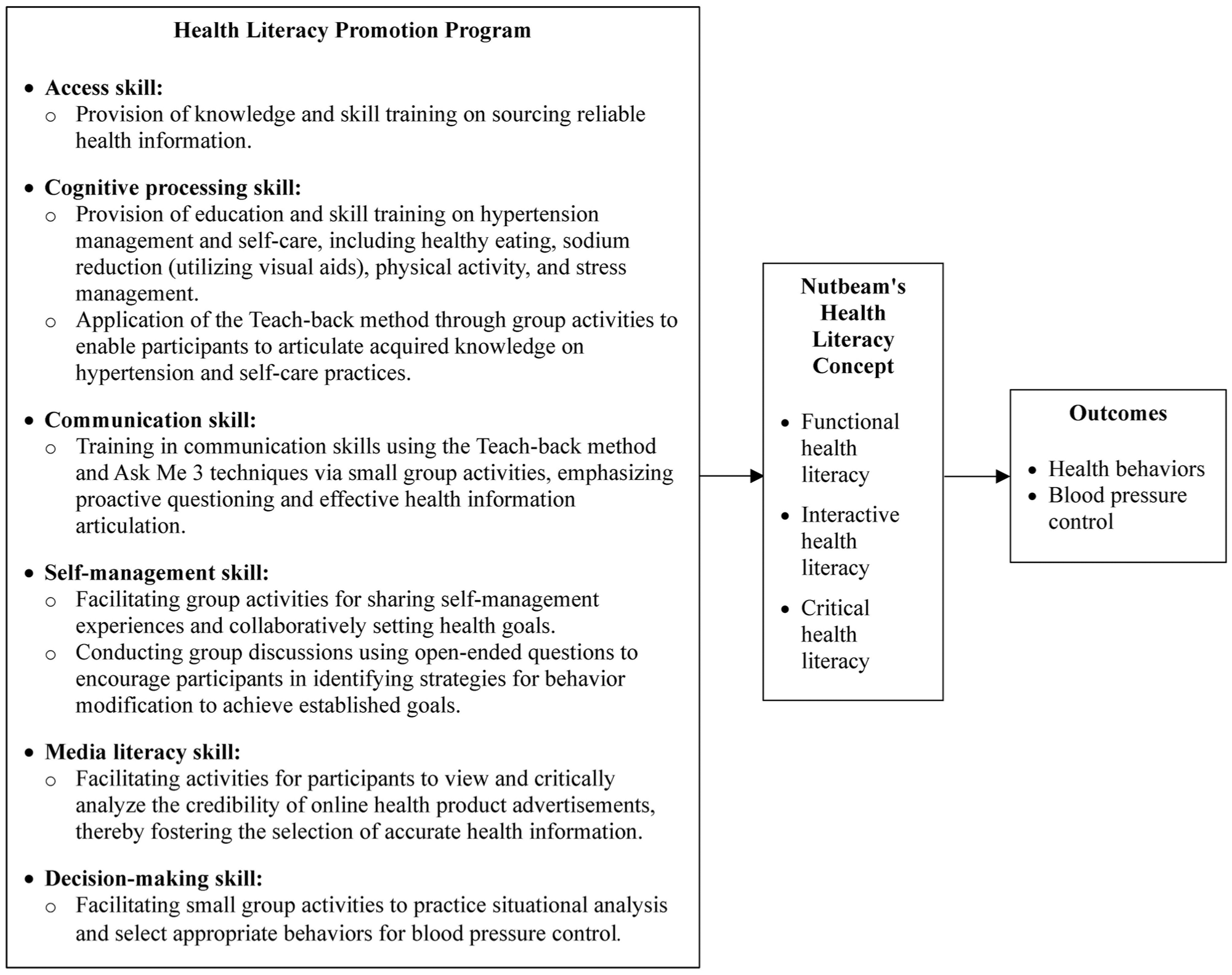
Conceptual framework of the health literacy promotion program based on Nutbeam’s health literacy concept.
Study Design
A quasi-experimental study with a 2-group pretest-posttest design; divided into 2 groups: an experimental group and a control group, was conducted over a 12-week intervention period, implemented between January and April 2025.
Sample
The sample comprised patients with uncontrolled hypertension, defined as a blood pressure level >130/80 mmHg, who were receiving continuous treatment at a subdistrict health promoting hospital in Phayao Province. Inclusion criteria were: good self-care ability, mobility (not homebound or bedridden), no dialysis treatment, ability to communicate and read in Thai, telephone accessibility, and willingness to participate in the research. The exclusion criterion was inability to participate in all study activities throughout the experimental period.
Sample size was determined using G*Power version 3.1.9.7 for a 1-tailed hypothesis test. An effect size of 0.5 was established based on comparable research, 19 with a power of 0.95 and an alpha level of 0.05. This calculation indicated a required sample size of 45 participants. To account for potential dropout and data loss, the sample size was increased by 10%, resulting in a total of 50 participants.
Simple random sampling combined with matched pairing was employed. Matching criteria included age (<40, 40-60, and 61-65 years) 2 and the most recent retrospective blood pressure level (131/81-140/90 and 141/91-160/100 mmHg), measured in the standardized sitting position. Twenty-five matched pairs were obtained and randomly assigned to either the experimental or control group (25 participants each) to control for confounding variables and enhance comparison efficiency.
Interventions for the Experimental Group
The experimental group participated in a 12-week health literacy promotion program, delivered through small group activities designed to foster functional, interactive, and critical health literacy. The program began in week 1 with the provision of knowledge and skill training for searching reliable health information sources, as well as providing education on hypertension and self-care, including healthy eating, sodium reduction (using visual aids), physical activity, stress management, and medication adherence. Motivational interviewing and experience sharing were integrated into group activities. Week 4 focused on communication skills, practicing the Teach-back method and the Ask Me 3 technique, alongside critical evaluation of online health media. By week 8, the curriculum advanced to practical application and decision-making through scenario-based discussions, where participants formulated specific “Ask Me 3” questions for hypertension management. Throughout the intervention, researchers maintained contact via structured home-based phone calls at weeks 2, 6, and 10 to monitor adherence, address barriers, and reinforce positive behaviors.
Intervention for the Control Group
The control group received usual care from the subdistrict health promoting hospital, comprising scheduled follow-up appointments and disease-specific health education. Upon completion of the 12-week study, the researcher provided health promotion to the control group by conducting training on disease-related knowledge, emphasizing the importance of attending scheduled appointments, and encouraging appropriate health behaviors for hypertension management.
Measures
Data were collected using a researcher-developed form. This form encompassed personal characteristics (gathered only at Week 1), as well as health outcomes, which were collected at Week 1 (pre-intervention) and Week 12 (post-intervention). These health outcomes included: Health behavior, specifically encompassing weight control, healthy eating, sodium restriction, physical activity, stress management, alcohol limitation, smoking cessation, and medication adherence, was evaluated using a 13-item questionnaire on a 5-point Likert scale (Cronbach’s alpha = 0.80; CVI = 1.00). Blood pressure was measured by the researcher using a single, calibrated automatic monitor throughout the study; this device had been verified for accuracy prior to use. Measurements were taken concurrently for both the experimental and control groups, with all readings recorded on a standardized form.
Statistical Analysis
Data were analyzed using SPSS. A significance level of P < .05 was set for all statistical analyses. Descriptive statistics were used to characterize participants’ personal information, health behavior scores, and blood pressure levels. The Shapiro-Wilk test assessed data normality. For inferential analyses, baseline comparisons of personal characteristics between groups were examined using chi-square tests, Fisher’s exact tests, and Mann-Whitney U test as appropriate. Paired t-tests compared health behavior scores and blood pressure within each group. Independent t-tests assessed between-group differences for health behavior scores and blood pressure levels. Effect sizes were reported using Cohen’s d. Additionally, Analysis of Covariance (ANCOVA) was performed to compare systolic blood pressure between groups, with baseline systolic blood pressure entered as a covariate. All assumptions for ANCOVA were met.
Results
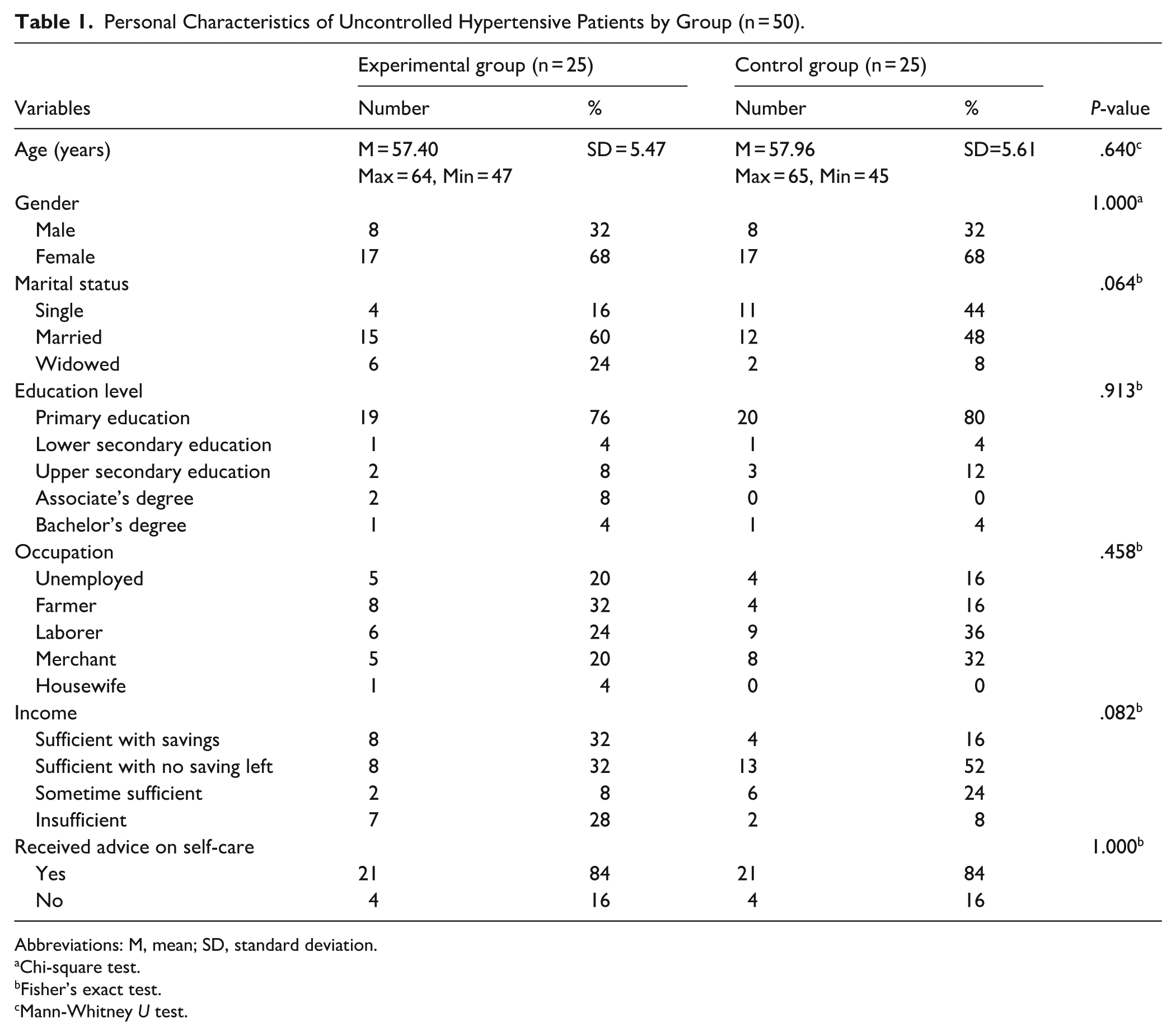
The study included 50 participants (n = 25 per group) in the experimental and control groups. Baseline personal characteristics were evaluated, with no statistically significant differences identified between groups across any variable (P > .05). This confirms the internal validity of subsequent intervention comparisons (see Table 1). In the experimental group, participants ranged from 47 to 64 years (mean 57.40, SD = 5.47 years), with 68% being female. Most were married (60%), and 76% had completed primary education. Dominant occupations included farmers (32%) and laborers (24%). Income was reported as sufficient with savings by 32% and sufficient without savings by another 32%. A significant 84% had previously received advice on self-care. Similarly, the control group participants were aged 45 to 65 years (mean 57.96, SD = 5.61 years), with 68% also female. In this group, 48% were married, and 80% had completed primary education. Primary occupations were laborers (36%) and merchants (32%). A majority (52%) reported themselves to be income sufficient without savings, and consistent with the experimental group, 84% had also previously received advice on self-care.
Personal Characteristics of Uncontrolled Hypertensive Patients by Group (n = 50).
Abbreviations: M, mean; SD, standard deviation.
Chi-square test.
Fisher’s exact test.
Mann-Whitney U test.
In the experimental group, post-program health behavior scores (M = 56.68, SD = 4.32) were significantly higher than pre-program scores (M = 47.96, SD = 5.81), with a mean difference (MD) of 8.72 (95% CI: 6.61, 10.82; t = 8.557, P < .001). Post-program SBP (M = 129.40, SD = 10.26 mmHg) was significantly lower than pre-program levels (M = 143.40, SD = 10.91 mmHg); MD = −14.00 mmHg (95% CI: −17.82, −10.18; t = 7.559, P < .001). Similarly, post-program DBP (M = 73.00, SD = 7.84 mmHg) significantly decreased from pre-program levels (M = 83.24, SD = 8.49 mmHg); MD = −10.24 mmHg (95% CI: −13.72, −6.76; t = 6.068, P < .001) (see Table 2).
Comparison of Mean Health Behavior Scores and Blood Pressure in the Experimental Group Pre- and Post-program (n = 25).

Abbreviations: DBP, diastolic blood pressure; SBP, systolic blood pressure; SD, standard deviation.
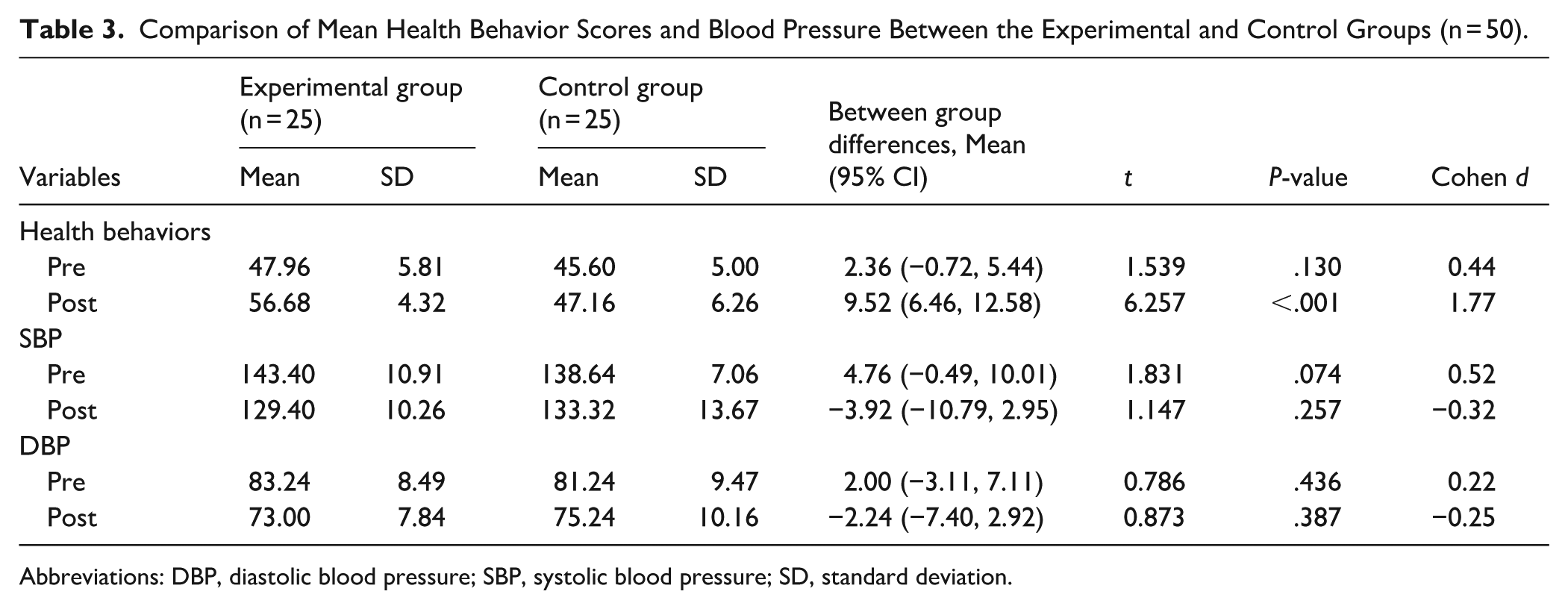
During the pre-program period, health behavior scores and blood pressure levels did not significantly differ between the experimental and control groups (P > .05). Post-program, the experimental group’s mean health behavior score (M = 56.68, SD = 4.32) was significantly higher than that of the control group (M = 47.16, SD = 6.26); the mean difference (MD) was 9.52 (95% CI: 6.46, 12.58; t = 6.257, P < .001), representing a very large effect size (Cohen’s d = 1.77). Although the experimental group’s mean SBP (M = 129.40, SD = 10.26 mmHg) was lower than the control group’s (M = 133.32, SD = 13.67 mmHg), this difference was not statistically significant; MD = −3.92 mmHg (95% CI: −10.79, 2.95; t = 1.147, P = .257; Cohen’s d = −0.32). Similarly, the experimental group’s mean DBP (M = 73.00, SD = 7.84 mmHg) was lower than the control group’s (M = 75.24, SD = 10.16 mmHg), but this difference was also not statistically significant; MD = −2.24 mmHg (95% CI: −7.40, 2.92; t = 0.873, P = .387; Cohen’s d = −0.25). As a moderate difference in pre-program SBP was observed between the groups (Cohen’s d = 0.52), potentially influencing the post-program comparison, an additional analysis using ANCOVA was conducted to control for this variable (see Table 3).
Comparison of Mean Health Behavior Scores and Blood Pressure Between the Experimental and Control Groups (n = 50).
Abbreviations: DBP, diastolic blood pressure; SBP, systolic blood pressure; SD, standard deviation.
Post-program SBP was compared between groups using Analysis of Covariance (ANCOVA), adjusting for pre-program SBP. The experimental group exhibited a significantly lower adjusted mean SBP of 127.94 mmHg (95% CI: 123.56-132.31) compared to the control group’s 134.90 mmHg (95% CI: 130.45-139.35). This represented an MD of −6.97 mmHg (95% CI: −13.33, −0.60; F = 4.853, P = .033; Partial η2 = 0.094) (see Table 4).
Comparison of Adjusted Mean Systolic Blood Pressure Between Experimental and Control Groups Post-program Using ANCOVA (n = 50).

Abbreviation: SBP, systolic blood pressure.
Discussion
Effect of the Health Literacy Promotion Program on Health Behaviors
The health literacy promotion program effectively improved health behaviors in patients with uncontrolled hypertension. Participants demonstrated a statistically significant post-program increase in mean health behavior scores compared to baseline, by 8.72 points (95% CI: 6.61, 10.82; P < .001). Furthermore, participants achieved significantly higher mean health behavior scores than non-participants, with a difference of 9.52 points (95% CI: 6.46, 12.58; P < .001). These positive outcomes stem from the program’s comprehensive design, which incorporated activities targeting all dimensions of health literacy, as guided by Nutbeam’s conceptual framework.10,11 Specifically, program activities fostered functional health literacy by developing patients’ access and cognitive skills. This enabled them to effectively search for health information and comprehend essential content for performing disease-appropriate behaviors. The program further employed the Teach-back method and Ask Me 3, enhancing cognitive and communication skills. This led to interactive health literacy, empowering patients to explain and communicate their understanding of health information for practical implementation. This approach aligns with literature demonstrating that the Teach-back method improves knowledge and self-management in chronic disease patients 20 and that these techniques enhance health literacy and self-care behaviors across multiple dimensions in patients with diabetes and hypertension. 21 Moreover, strategies such as motivational interviewing and participatory group activities (e.g., discussions, self-management experience sharing, and online health media analysis) were integrated. These strategies nurtured self-management, media literacy, and decision-making skills, culminating in critical health literacy. Patients thus became capable of selecting media for health risk avoidance and were motivated to make behavioral decisions aligned with predetermined health goals. Motivational interviewing further stimulated intrinsic learning and built self-efficacy, contributing to sustainable health behavior changes. 22 The effectiveness of participatory action learning in hypertension management has been validated by prior research, showing statistically significant improvements in health literacy, physical activity, low-sodium diet adherence, and medication adherence (P < .01). 23 These findings are consistent with systematic reviews on health literacy promotion programs, which confirm their effectiveness in enhancing health literacy and promoting health behaviors among patients with hypertension.24,25 Consequently, this program demonstrates strong potential for integration into primary healthcare systems to support sustainable health behavior change.
Effect of the Health Literacy Promotion Program on SBP
The health literacy promotion program effectively reduced SBP in patients with uncontrolled hypertension. Participants demonstrated a statistically significant post-program reduction in mean SBP by 14.00 mmHg (95% CI: −17.82, −10.18; P < .001) compared to baseline. Furthermore, participants achieved significantly lower mean SBP than non-participants, with a difference of 6.97 mmHg (95% CI: −13.33, −0.60; P = .033). This SBP reduction is clinically meaningful, as a decrease of 5 mmHg or more can reduce cardiovascular disease risk. 26 The program’s success stemmed from the integration of key strategies promoting sustainable health behavior change, including enhanced patient engagement in decision-making, communication skill development, and motivational interviewing to build self-efficacy in effective health management. Tailored health behavior modification for specific diseases is an effective method for reducing high blood pressure. 26 These findings align with studies employing the Teach-back method, Ask Me 3, and motivational interviewing techniques, which consistently report statistically significant SBP reductions.21,22,27 Moreover, systematic reviews confirm health literacy promotion programs effectively improve health literacy, health behaviors, and blood pressure control. 25 Thus, the systematic integration of health literacy promotion strategies offers an effective approach to enhancing health outcomes in patients with hypertension.
For DBP, participants experienced a mean reduction of 10.24 mmHg (95% CI: −13.72 to −6.76; P < .001) from their pre-program measurement post-program. This reduction is clinically meaningful, as a large-scale meta-analysis demonstrated that a decrease in DBP by just 3 mmHg significantly lowers the risk of cardiovascular complications (P = .024). 28 However, no statistically significant intergroup difference was observed, which may be attributed to several limitations. Both groups resided in the same area and accessed the same healthcare services, potentially leading to information sharing and experiences that influenced behavior changes in the control group similar to those of the intervention group. Additionally, the relatively small sample size and 12-week follow-up period may have been insufficient to detect clear intergroup differences. These findings align with other studies of similar duration that also reported no statistically significant DBP differences between groups.21,29,30 In contrast, studies with larger sample sizes and longer follow-up periods have shown statistically significant differences (P < .001).31-33 Future research should consider increasing sample size and extending follow-up duration to confirm the program’s effectiveness on DBP levels.
This study has several notable strengths. First, the randomized controlled trial design minimized selection bias and enhanced the credibility of the findings. Second, the program was systematically developed based on a theoretical framework, allowing for a clear explanation of underlying behavior change mechanisms. Third, the sample consisted of patients with uncontrolled hypertension, a clinically and publicly significant target group. Fourth, all participants actively engaged in program activities throughout the study, fostering sustainable engagement through collaborative learning. Lastly, the program demonstrated high feasibility for implementation and scalability within the primary healthcare system. Nonetheless, some limitations warrant consideration. First, the limited sample size may have reduced statistical power to detect significant intergroup differences, particularly for variables with high variability. Second, recruiting participants from a single community may have introduced contamination bias due to shared information or similar healthcare access. Finally, the 12-week follow-up period may have been insufficient to assess sustained physiological changes in blood pressure.
Conclusions
The health literacy promotion program, integrating the Teach-back method, Ask Me 3, motivational interviewing, and participatory group activities, effectively improved health behaviors and reduced SBP among patients with uncontrolled hypertension. This program is suitable for adoption by primary care providers to promote health behavior change and achieve improved clinical outcomes. Future research, however, should employ larger sample sizes and longer follow-up periods to more definitively determine the program’s effectiveness in reducing DBP.
Footnotes
Acknowledgements
The authors gratefully acknowledge all the patients with uncontrolled hypertension involved in this study for their invaluable participation, which was fundamental to its successful completion.
Ethical Considerations
This study received ethical approval from the University of Phayao Human Ethics Committee (HREC-UP-HSST 1.2/148/67) on September 17, 2024.
Author Contributions
LT conceptualized the study. LT and PS contributed to the development of the methodology. LT, PS, and JS were responsible for conducting activities with participants and collecting data. LT and PS collaboratively analyzed the data. LT drafted the original manuscript. All authors participated in critically reviewing and revising the manuscript, and all approved the final version for submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by research funding from the revenue budget of the School of Nursing, University of Phayao.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.