
Abstract
Background:
Mental health conditions are a leading cause of maternal mortality. Within Latina ethnicity, being foreign-born has been associated with better health outcomes than being US born, but the relevance of this immigrant paradox to perinatal mental health remains underexplored. This study investigates whether ethnicity (Latina/non-Latina) and nativity (foreign vs. US born) are associated with differences in postpartum depression and anxiety within a sample of women in Central Texas.
Methods:
We conducted a secondary analysis of a prospective observational cohort (n = 76). Participants completed the Edinburgh Postnatal Depression Scale (EPDS) and Generalized Anxiety Disorder-7 (GAD-7) between 6 and 12 weeks postpartum. We performed stepwise forward linear regression models with log-transformed depression and anxiety scores.
Results:
The mean GAD-7 score amongst all participants was 4.07 (SD = 4.72), and the mean EPDS score was 4.68 (SD = 5.21). Approximately 21% of participants met the clinical threshold for anxiety, and 10.8% met the clinical threshold for depression. Hispanic/Latina participants had 56% lower GAD-7 scores compared to non-Latina participants (95% CI: 0.29-0.67), and foreign-born participants had 39% lower GAD-7 scores compared to U.S. born participants (95% CI: 0.39-0.95). Nativity was not significantly associated with EPDS scores and was not retained in the final depression model. Hispanic/Latina participants had 43.1% lower EPDS scores than non-Latinas (95% CI: 0.38-0.86). All results are based on adjusted, log-transformed linear models.
Conclusions:
We found that Hispanic/Latina ethnicity was associated with lower postpartum anxiety and depression scores. Additionally, being foreign born was associated with lower postpartum anxiety scores. These findings suggest the immigrant paradox may apply to perinatal mental health outcomes among Latinas. Future research should explore within-group differences among Latinas and consider variables such as acculturation, immigration status, income, and country of origin.
Keywords
Introduction
Between 10% to 20% of pregnant women in the U.S. experience depression which, when unaddressed, is a risk factor for postpartum depression.1,2 Untreated, poor mental health conditions such as depression, anxiety, or substance use disorders is a major risk factor for maternal mortality, due to suicide or unintentional prescription overdose. 3 For example, data from 14 U.S. Maternal Mortality Committees found that 63% of maternal deaths were due to suicide, and 100% of mental-health related maternal deaths were preventable. 4 Moreover, a national analysis found that the leading cause of maternal death for Hispanic women was mental health conditions (24%). 5
Although depression and anxiety are some of the most common pregnancy and postpartum complications, most mental health data is not disaggregated by race or ethnicity. One population-based study found that Latina women reported higher rates of mild, moderate, and severe prenatal depression compared to White women. 6 Two smaller studies found that Latina women experience unique cultural stressors such as discrimination and acculturation, which can influence perinatal depression or anxiety.7,8 Given link between perinatal mental health and maternal mortality, it is critical to better understand perinatal depression and anxiety among Latinas in Texas. 9
Recent large-scale studies have further examined how nativity and language proficiency intersect with perinatal mental health. A population-based cohort of pregnant individuals in Northern California found that non-U.S. born Hispanic women generally had an equivalent or lower risk of prenatal depression diagnoses compared to U.S.-born Hispanic women, although certain Hispanic subgroups showed higher risks of moderate to severe depressive symptoms. 10 Similarly, a longitudinal study of low-income Latina women found that depressive symptoms declined on average from pregnancy to 6 weeks postpartum, but limited English proficiency predicted worse trajectories of depressive symptoms over time. 11 Together, these findings reinforce the significance of nativity and language in understanding perinatal mental health disparities, which may reflect broader acculturative factors such as reduced social support or increased exposure to discrimination among U.S.-born or English-dominant individuals.
The “immigrant paradox” has been well documented across health conditions within Hispanic and Latino populations. 12 The immigrant paradox is a phenomenon where immigrants have superior health outcomes compared to U.S.-born individuals, and it has been explored with maternal health outcomes among Latinas. 13 While a recent scoping review found that Latinas have lower rates of preterm birth, low birth weight, and infant mortality compared to non-Hispanic White and non-Hispanic Black women, the study did not measure mental health. 14 Another study found that length of residency in the United States was significantly associated with perinatal depression among Latinas; longer residency in the United States was associated with higher levels of depression. 15
Research suggests that the immigrant paradox may be explained by the physical ability to migrate to the United States, the availability of strong social ties in a new country, or cultural traditions among foreign-born populations. 16 Newer research suggests that the immigrant paradox may be better explained by length of time in the US, or other cultural factors such as discrimination and acculturation, particularly for US-born Latinas.14,17 Acculturation, defined as changes in beliefs, attitudes, or behaviors such as language spoken due to living within a new culture, 18 can include stressors such as discrimination, which is linked to risky behaviors such as substance use.19,20 Research also suggests that acculturation level, and potential benefits, can change over time depending on the sociocultural context. 21 While there are several standardized measures of acculturation based on beliefs, nativity or language spoken are often used as a proxy measure of acculturation, yet can be insufficient for measuring the complexity of the acculturation process.22,23
Therefore, we conducted an exploratory analysis with data from a prospective, observational cohort study to examine the frequency and severity of depression and anxiety among a diverse sample of women in Central Texas based on nativity (foreign-born vs. US-born) and ethnicity (Latina vs. Non-Latina). Given the study’s setting in Central Texas, it’s important to note that regional policy and health system factors may influence participants’ perinatal mental health and access to care. Texas ranks 50th in overall women’s health performance, with mental health conditions among the top 3 causes of preventable maternal deaths.24,25 Additionally, despite evidence that doulas improve maternal outcomes, Texas has yet to adopt widespread Medicaid reimbursement for these culturally congruent services.26,27 These structural gaps, alongside limited behavioral health integration in perinatal care and a restrictive immigration climate, may shape mental health risk and help-seeking behavior among immigrant Latinas in Texas. 9
Methods
Study Design and Setting
This is a secondary analysis of data from the Study of Nutrition in Pregnancy and Early Life (SUPER) Clinic Study, a prospective observational cohort of women and their singleton, term infants from Austin, Texas.
Participants, Recruitment, and Data Collection
Pregnant women were recruited from the university-affiliated maternal fetal medicine (MFM) ultrasound clinic. Inclusion criteria included: (1) 18-55 years of age, (2) 18–32 weeks’ gestation, (3) English or Spanish speaking, and (4) no fetal anatomical abnormality. The study team recruited on-site, an average of 3 days a week, from May 2023 through September 2023.
Study team members identified eligible patients via the MFM clinic electronic health record (EHR). A bilingual research assistant approached eligible patients privately at the time of their MFM ultrasound clinic appointment. Interested patients signed informed consent, provided HIPAA authorizations for continued EHR access, and provided contact information to follow up after birth. Only participants with the following criteria were contacted at 6 to 12 weeks to complete survey measurements about postpartum mental health: (1) a verified birth in the university-affiliated hospital system’s electronic health record; (2) a term birth, defined as >37 weeks; (3) no NICU visit for >72 h; and (4) no maternal hospitalization to the intensive care unit. A study team member periodically screened the electronic health record from May 2023 to January 2024 to confirm births, and follow-up concluded in April 2024. This study was approved by the University’s Institutional Review Board (Figure 1).
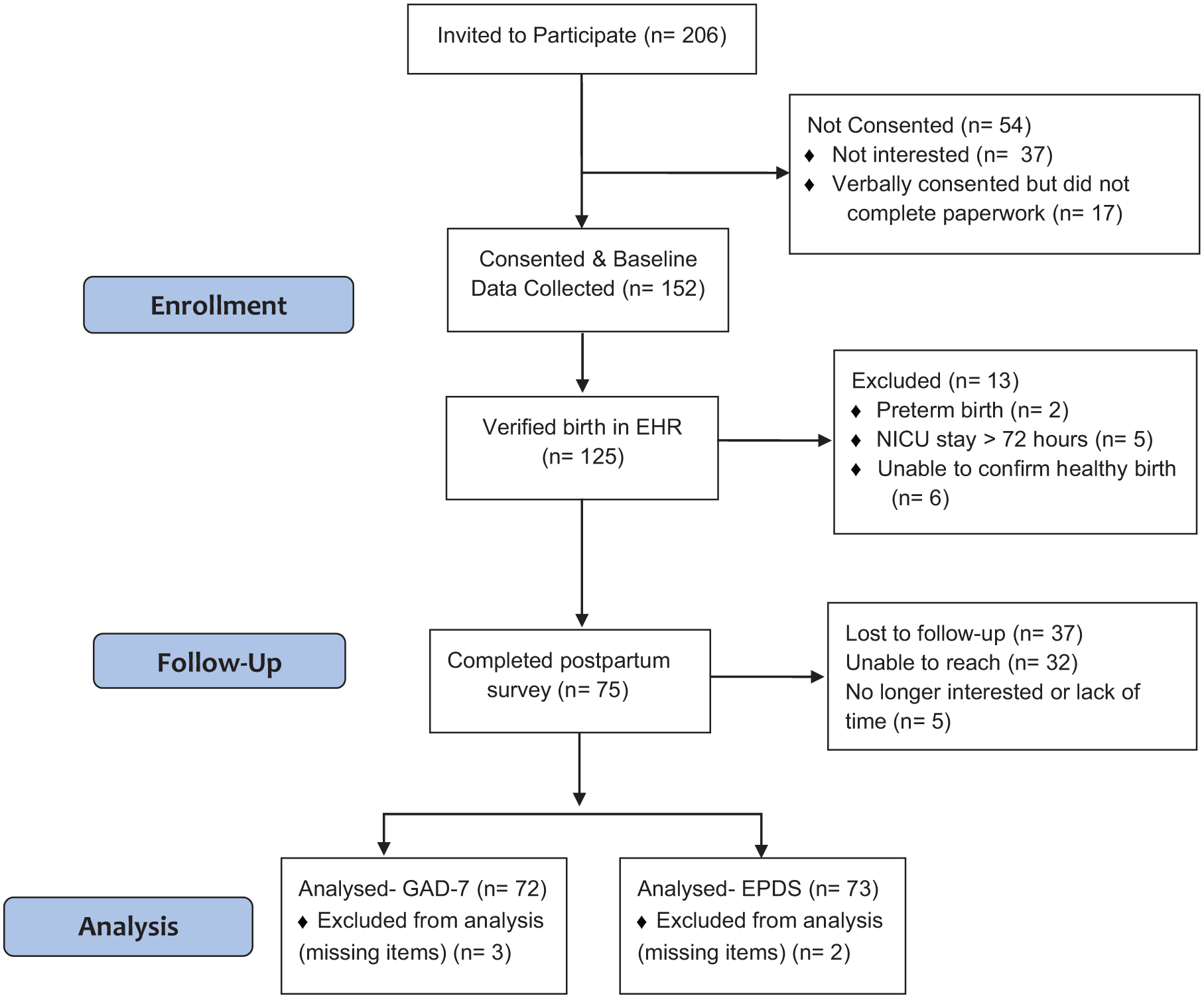
CONSORT flow diagram.
Measures & Variables
During enrollment, mothers completed a demographic survey in English or Spanish that included the following variables: age, race, ethnicity, marital status, sexual orientation, education, number of children in the household, and nativity. The age variable was continuous (increases in 1-year increments) and restricted to adults between 18 and 55. Marital status was coded into dichotomous categories: single (includes “single, never married,” “divorced,” “separated,” or “widowed”) or partnered (includes “married” or “living as married, common law”). Nativity was defined as US-born or foreign born. Country of origin was only asked of women who identified as foreign-born. Therefore, this data was not available for all women who identified as Latina. Education was coded into 3 categories: high school or less, some college, and college or more. Since 26.3% of the data was missing for education level, we created a fourth category for missing data and controlled for this in all models. We measured language based on the language in which the participants chose to complete the survey. Insurance information was extracted from the electronic health record and coded as private or non-private insurance. Non-private insurance primarily referred to government-sponsored programs (e.g., Medicaid, CHIP) and also included 2 uninsured individuals.
Anxiety and depression were measured at 6 to 12 weeks postpartum via the Generalized Anxiety Disorder scale (GAD-7; Spitzer et al, 2006) 28 and the Edinburgh Postnatal Depression Scale (EPDS; Cox, 1987). Responses to the GAD-7 and EPDS screeners use a 4-point Likert scale (from 0 “not at all” to 3 “nearly every day”). A patient’s sum score of the 7 GAD-7 items is categorized as minimal (0-4), mild (5-9), moderate (10-14), and severe (15-21) and their sum score of the 9-item EPDS is categorized as none (0-6), mild (7-13), moderate (14-19), and severe (19-30). The EPDS has been validated with Spanish-speaking, Hispanic women. 29 The GAD-7 have been validated with Hispanic, Spanish-speaking populations as well as Spanish-speaking, pregnant individuals.30,31 Only participants with complete responses to all items in the GAD-7 or EPDS scales were included in the summation of scores.
Statistical Analyses
We included data from all participants who met eligibility criteria and completed the 6- to 12-week postpartum mental health survey.
We described all sociodemographic characteristics (e.g., race, age, language, education, marital status, insurance type, and nativity) and mental health outcomes using means, standard deviations, medians, and ranges for continuous variables, and proportions for categorical variables. All descriptive statistics were stratified by ethnicity (Hispanic/Latina vs. Not Hispanic/Non-Latina). Although anxiety and depression outcomes (GAD-7 and EPDS) were treated as continuous variables in regression models, binary indicators of anxiety and depression were generated for descriptive purposes using establishing clinical thresholds of GAD-7 ≥ 8 and EPDS ≥11.32,33 Due to right-skewed distributions, total GAD-7 and EPDS scores were log-transformed to create approximately normal outcome variables. These transformed outcomes were used in building our model through stepwise regression.
We performed stepwise forward selection (through the MuMIn library) using log-transformed linear regression models to identify the best-fitting adjusted models. Ethnicity was included in the base model, and candidate covariates (nativity, age, insurance status, marital status, education, and language) were selected a priori based on prior literature. Each co-variate was sequentially added and only retained if it lowered Akaike Information Criterion (AIC) by ≥2 points, indicating a meaningful increase in model fit.
The final anxiety model only retained both ethnicity and nativity as predictors. The final depression model retained only ethnicity. All other covariates did not improve model fit and were excluded. Regression coefficients and confidence intervals from the log-transformed models were exponentiated to return estimates on the original scale. This allowed for interpretation as percent differences in EPDS/GAD7 scores relative to reference groups. All analyses were conducted using R version 4.3.2. R packages such as readr, Table 1, MuMIn, and dplyr were used for data cleaning and manipulation. Statistical significance was defined as P < .05.34-37 Because this study was designed as a feasibility trial, the sample size was determined pragmatically rather than based on a formal power calculation.
Demographics and Mental Health Outcomes.

Results
Sociodemographic Findings
Table 1 presents demographic and mental health characteristics for the full analytic sample (N = 76), as well as stratified by ethnicity (Latina vs. Non-Latina). The sample was 53.9% Latina and 72.4% completed the survey in English. Most participants reported being partnered (69.7%), born in the U.S. (65.8%), and had either some college or more education (38.2%), with 51.3% reporting private insurance. The majority of foreign-born women identified as Latina and were from Central and South America such as Mexico (n = 8); Honduras (n = 4); El Salvador (n = 2), Cuba (n = 1), Guatemala (n = 1), and Venezuela (n = 1). The mean (SD) number of children in the household was 1.01 (1.04).
Mental Health Outcomes
Untransformed mean anxiety and depression scores were 4.07 (SD = 4.72) and 4.68 (SD = 5.21), respectively. Among Latina participants, average GAD-7 and EPDS scores were 2.46 (SD = 4.28) and 3.32 (SD = 4.59), compared to 6.09 (SD = 4.54) for GAD-7 and 6.53 (SD = 5.50) for EPDS among non-Latinas. Approximately one-fifth of the sample (20.5%) met the clinical threshold for anxiety (GAD-7 ≥ 8), while 10.8% met the threshold for depression (EPDS ≥ 11).
Regression Analyses
Being Latina was associated with a 43.1% lower EPDS score than being Non-Latina (95% CI: 0.38-0.86). The stepwise regression model for depression included only ethnicity (adjusted R-squared = 0.079, F = 7.20, P < .01). Nativity was not significantly associated with EPDS scores and was not retained in the final model. Being Latina was associated with a 56% lower GAD-7 score than being Non-Latina (95% CI: 0.29-0.67). Additionally, being born outside the US was associated with a 39% lower GAD-7 score than being born in the US (95% CI: 0.39-0.95). The model for anxiety included both ethnicity and nativity after the stepwise regression (adjusted R-squared = 0.24, F = 12.44, P < .001). Refer to Tables 2 and 3 for more details. There was no evidence of an interaction between ethnicity and nativity (data not shown) for either the depression or anxiety models.
Adjusted Stepwise Linear Regression Model for Depression (N = 74).

**P < .01.
Adjusted Stepwise Linear Regression Model for Anxiety (N = 73).

P < .05. ***P < .001.
Discussion
We found that Latinas reported significantly lower depression and anxiety scores compared to non-Latina women, and that foreign-born women reported significantly lower anxiety, but not depression, scores compared to US-born women. One possible explanation is that Latina ethnicity is protective of perinatal mental health because cultural values and practices support women during pregnancy. Caretaking is central in Latina culture and a child’s health and wellbeing is considered above other needs, particularly among women. Although this belief may be shared by different ethnic groups, it is often manifested in Latina culture through specific practices, such as mothers staying home to raise children, avoiding risky behaviors (e.g., drinking, substance use, arduous exercise), and relying on a working partner and other support systems to provide for the child and the mothers’ wellbeing.38,39 Nevertheless, Latina ethnicity is not monolithic, 13 and mental health, as well as wealth and opportunity, vary by nationality. 40 However, while race and country of origin in outcomes have been linked to perinatal outcomes among Latina subgroups, 41 perinatal mental health outcomes remain to be explored in this context.
Another key consideration is that the immigrant paradox is not a static phenomenon. Other relevant variables such as immigration status, length of residence in the US, acculturation, and neighborhood-level variables like residing in ethnic enclaves and experiencing structural segregation can gain saliency in the current sociopolitical climate. 41 Thus, being foreign-born may not be protective enough if federal and state policies put greater pressure on immigrants and other vulnerable populations. 42 To avoid making static assumptions about ethnic and immigrant groups, it is important to consider not only the heterogeneity that exists within a group, but also the social and political climate and its effect on perinatal mental health and access to care.
These findings have important implications for research on perinatal mental health in Latinas in the US. In terms of research, cultural factors are important to consider when developing, culturally adapting, and testing mental health interventions for perinatal Latinas. A larger cohort would shed light on Latina intersectionality (race, nativity, age, immigration status, length of residence) and on policies that facilitate and hinder perinatal mental health and access to care. Where the person resides also matters in research, as states vary in their level of protections for foreign born and undocumented women and children. 43 Additionally, while the EPDS and GAD-7 are considered gold-standard assessments, it is possible that foreign-born Latinas are underreporting mental health symptoms due to low mental health literacy, mental health stigma, or are more fearful or hesitant to report mental health symptoms due to the political climate.44-46 Qualitative studies that explore the perceptions of standardized mental health screenings in perinatal settings with a diverse sample of Latinas could better explain the immigrant paradox among Latina perinatal mental health outcomes.
These findings also have important implications for perinatal clinicians. Several studies have found that foreign-born Latinas have consistently lower rates of depression or anxiety, and residence in the US is associated with higher levels of depression. 15 Screening tools and interventions should be culturally tailored to consider nativity, language, and potential mental health stigma since foreign-born Latinas may underreport symptoms due to cultural norms or fear. Given previous research suggesting that Latinos prefer informal mental health support, 47 public health strategies should include community-based screening models, partnerships with trusted cultural institutions, and expanding access to bilingual mental health services tailored to immigrant mothers.
Limitations
There are several limitations to our analysis. First, this secondary analysis of a single clinic-based cohort with a small sample size (n = 76); therefore, the interaction models may have been underpowered and may not generalize to larger populations or populations located in other regions. However, we minimized selection bias by recruiting all eligible English and Spanish-speaking patients attending the MFM ultrasound clinic and having bilingual staff. Second, we limited our analytic sample to individuals who completed the full post-natal mental health survey to ensure consistent outcome measurement across participants. Patients with any missing items on the GAD-7 (n = 2) or EPDS (n = 3) scales were excluded from analysis to preserve the validity of summed scale measures, but we were unable to assess if data were missing at random. While the PHQ-9 and GAD-7 have been assessed for psychometric quality with perinatal Latinas, it is possible that our findings related to nativity and ethnicity were influenced by the cultural relevance of the screening tools.
Third, we did not include a standardized measure of acculturation due to the design and scope of the original survey; however, we included nativity and language as potential proxy variables. Only nativity was significantly associate with mental health outcomes, and future studies should include more standardized measures or composites of acculturation. Further, we only collected country of origin for foreign-born women instead of all Latina women and could not assess the national heritage of US-born Latinas. We were also unable to explore how nativity status intersected with ethnicity due to the small sample size. Finally, our analytic sample only included participants who gave birth at a university-affiliated hospital, 97% of whom were insured.
Future studies should explore the immigrant paradox in a larger, nationally representative sample that allows for an exploration of how ethnicity (Latina/non-Latina) intersects with nativity (US born/foreign born) to affect perinatal mental health and of differences across Latina ethnic subgroups. Future studies could also assess differences in public health insurance plans, such as distinguishing by type of Medicaid coverage (full vs. CHIP). Finally, future studies in this field should include measures of acculturation, discrimination, and socioeconomic stressors to better understand how these factors shape the immigrant paradox in perinatal mental health. Proxy measures of acculturation such as nativity are not as reliable or valid as standardized measures, and future studies would benefit from using more rigorous methods. 23 Epidemiological studies that are representative of the population and include other relevant variables such as acculturation and immigration status are warranted to more thoroughly explore these relationships.
Conclusions
Our findings of significantly lower anxiety among Latinas and foreign-born women and depression among Latinas suggest that the immigrant paradox may apply to perinatal mental health outcomes. Future research should explore within-group differences among Latinas and consider culturally relevant variables such as acculturation, immigration status, income, and country of origin.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received funding from the National Cattlemen’s Beef Association, a contractor to the Beef Checkoff and the Texas Beef Council for data collection. The funders had no role in study design, execution, or interpretation of research and placed no restrictions on publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.