
Abstract
Background:
Adolescent girls and young women (AGYW) in the U.S. Southeast are disproportionately affected by HIV. We developed and piloted PrEP-Pro, an intervention to support family medicine residents to prescribe HIV pre-exposure prophylaxis (PrEP), with a focus on AGYW. We pilot-tested the intervention, evaluating feasibility, acceptability, and appropriateness.
Methods:
Using intervention mapping, we developed sexual history training, PrEP curricula, and a PrEP champion program. For the 6-month pilot test, we trained PrEP champions who trained and supported residents at their sites. Participating physicians completed enrollment and exit questionnaires capturing PrEP provision experiences, attitudes/skills/barriers to completing a sexual history, and PrEP knowledge/attitudes/beliefs. Exit questionnaires assessed PrEP-Pro acceptability, feasibility, and appropriateness. We compared enrollment and exit scores on sexual history assessment, PrEP knowledge, and provider behaviors.
Results:
Among 46 participants (median age = 29 years), 57% were men, 59% were White, 15% were Asian, 11% were Latinx, and 7% were Black. Among 32 (70%) participants completing both enrollment and exit questionnaires, we observed significant increases in sexual history skills, PrEP knowledge, and PrEP attitudes, and non-significant increases in the proportion reporting routine sexual history assessment and HIV testing. On a 5-point scale, feasibility (mean 4.28 (SD = 0.42), acceptability (4.31 (0.53)), and appropriateness (4.25 (0.46)) scores were high with respect to the PrEP-Pro intervention.
Conclusion:
This multi-component intervention was feasible, acceptable, and appropriate for family medicine residents in the pilot. Pre- and post-evaluation suggest participation in the intervention increased PrEP knowledge and improved sexual history-taking. These findings suggest that the intervention could successfully enhance provider self-efficacy in delivering sexual health care.
Introduction
In the United States (U.S.), adolescent girls and young women (AGYW) accounted for 20% of new HIV infections in 2022. 1 Black AGYW bear a disproportionate burden of new diagnoses. 2 In 2019, Black women accounted for 54% of new HIV diagnoses among women while representing 13% of the female population. 2 In the Southeast, it is estimated that Black AGYW make up over two-thirds (67%) of new HIV diagnoses among women 3 and in Alabama (AL), adolescents and young adults accounted for 52% of new HIV diagnoses among 13 to 29 year old in 2018. 4
Pre-exposure prophylaxis (PrEP) prevents HIV, but uptake is low, especially among populations that may benefit most. In 2021, among PrEP users in the U.S., 64% were White and 14% were Black. 5 Only 9% of PrEP users were female in 2024, and only 11% of all PrEP users were 13 to 24 years old in 2023.6,7 Thirty-nine percent of PrEP users are in the South, despite representing 53% of new HIV diagnoses in 2022 and having the lowest regional PrEP-to-Need ratio of all U.S. regions.6,7 At the national level, PrEP prescriptions are lowest among adolescents and young adults, Black individuals, and those living in the South. 8
Multilevel barriers limit PrEP use. At the client-level these include low PrEP awareness, low risk perceptions, and PrEP-associated stigmas9-12; health care system-level factors include knowledge gaps and comfort among providers, unconscious bias, and racism13-15; and at the structural-level, costs and lack of health insurance15-17 contribute to low PrEP prescriptions. Provider barriers include concerns about structural barriers (eg, PrEP care reimbursement, disruption of workflow), knowledge gaps (PrEP indications and safety among adolescents), and lack of awareness about HIV-risk based on sexual behavior.18-25 Additionally, individual-level barriers among U.S. women26-30 and adolescents12,27,28,31,32 including low PrEP awareness,12,26,29,30 discordance between self-perceived and actual risk for HIV,12,27,31 PrEP-associated stigma,12,26,32,33 mistrust of the healthcare system,26,29,30,32 lack of desire to take a medicine when well, 12 intensive follow-up procedures, 28 and low self-efficacy for daily pill adherence. 28 Those living in the South also face more limited access to PrEP providers and lower health care capacity. 34 While most HIV providers are familiar with the dosing, side effects and comprehensive sexual health services associated with PrEP delivery, the same is not true among general practitioners. 35 Brief single-session educational interventions with family planning clinic providers in Georgia and PCPs in North Carolina showed that greater provider knowledge was associated with higher rates of PrEP prescription.36,37 Alabama’s plans to “End the HIV Epidemic” emphasize the need to “support community [HCPs] to incorporate HIV risk assessment, PrEP eligibility screening, and prescribing into their scope of practice.” 38 One way to overcome these barriers and increase PrEP use among Black individuals and AGYW in the South is by training providers to provide sexual health and PrEP clinical care.35-37,39
To empirically examine whether a multicomponent intervention could effectively train and support family medicine (FM) trainees in providing PrEP for adolescent girls and young women (AGYW) in the U.S. South, we developed and pilot tested PrEP-Pro. 40 To our knowledge, this is the first provider intervention to promote PrEP prescription to AGYW in the South. Working with Family Medicine trainees is an innovative approach to promote PrEP provision by clinicians who work with adolescents in rural communities across the U.S. 41 Adapting PrEP-Pro to trainees provided an opportunity to modify clinician behavior at an early stage of training and may help seed the rural health workforce with effective HIV prevention advocates and providers. 42 Combining education specialists in theory-based intervention mapping with community engagement allowed us to adapt interventions with greater content retention and implementation. We utilized the Capability-Opportunity-Motivation-Behavior (COM-B) model to consider mechanisms for modifying provider behavior through PrEP-Pro, including understanding how healthcare providers take a sexual history from adolescents to assess vulnerability to HIV infection (capability); the clinical and social environment, as well as program-level supports for learning and implementing sexual health into practice (opportunity); and trainees’ willingness to engage with clients in discussion about sexual health and HIV prevention (motivation). The PrEP-Pro training intervention was designed to address each element of COM to increase PrEP prescription to Black AGYW in AL.
Here we present pilot data on acceptability and feasibility of the PrEP intervention and exploratory data around efficacy regarding HIV/STI testing and PrEP prescriptions.
Methods
Setting and Participants
This pilot study was conducted in Alabama with 4 FM residency programs across 5 clinical sites serving urban, suburban, and rural patient populations (Figure 1). When this study was conducted in 2023, there were 11 family medicine residency programs in Alabama, several of which were new within the last 5 years. The adaptation and pre-test phases of this study 43 included trainees from 5 sites, and the pilot test reported here included trainees from 4 programs (one of which had residents rotating between 2 sites), 2 of which had not participated in prior components. All 11 programs were contacted to explore interest in participating in the pilot test, leveraging existing professional relationships through the study institution’s family medicine training program’s leadership. Reasons for declining participation included having a pre-existing PrEP training program, having limited capacity for additional projects, and not having sufficient turnover of residents to participate further (eg, if they participated in the pre-test, we needed new participants for the pilot).

Intervention Development
Intervention Mapping (IM) is a systematic approach to development, implementation, and evaluation of interventions, utilizing community-based participatory methods to address health concerns across multiple levels. IM framework consists of 6 key steps: (1) constructing a logic model of the problem; (2) developing a logic model of change by delineating the targeted behavioral and outcome objectives of the intervention; (3) designing the intervention by identifying behavioral change techniques grounded in theory and empirical evidence; (4) producing the intervention by integrating components into a structured program; (5) formulating strategies to facilitate the adoption, implementation, and sustainability of the program; and (6) assessing the program’s implementation and effectiveness. The PrEP-Pro intervention, developed using IM, consisted of 3 didactic presentations, delivered over two 2-h Zoom sessions to site PrEP Champions. The sexual history and PrEP management curricula covered communication with adolescents and prescribing across diverse populations, while the PrEP Champion module addressed inequities, barriers, and strategies for supporting PrEP access and coverage. Prior work detailed IM Steps 1 through 5.46,47 The present discussion details Step 6.
Community Advisory Boards
Two Community Advisory Boards (CABs) brought together members from rural and urban areas. The “Provider CAB” consisted of specialists in adolescent medicine, FM physicians (including trainees), and clinic administrators. They guided the development of intervention components and offered feedback on the specific local context. The “AGYW CAB” consisted of AGYW residing in Alabama. Each CAB met from April 2022 to February 2023 to evaluate the proposed materials and recommend context-specific modifications.
Frameworks
Capability-Opportunity-Motivation-Behavior Model (COM-B)
The COM-B model of behavior change provides a framework for understanding factors influencing behavior (B) and informed PrEP-Pro and its implementation strategies. The model comprises 3 components: Capability (C) refers to an individual’s ability and confidence to perform a behavior. For instance, healthcare professionals must be proficient in obtaining a sexual history to assess PrEP indications. Opportunity (O) encompasses the social and environmental conditions enabling or hindering behavior execution. Effective PrEP provision requires structural and interpersonal support (ie, guidance from PrEP Champions, to navigate challenges related to insurance coverage, confidentiality, and social stigma). Motivation (M) pertains to an individual’s readiness to engage in a behavior despite competing demands. Motivation can be enhanced through education about PrEP efficacy and by reducing barriers to prescribing.
Consolidated Framework for Implementation Research (CFIR)
CFIR identifies barriers and facilitators to intervention uptake, guiding the customization of implementation strategies and adaptations. CFIR was applied in intervention and questionnaire development to examine provider-level determinants, including readiness for change, self-efficacy, knowledge, and attitudes regarding PrEP and sexual history-taking/risk assessment.43,46
Pilot Test Deployment
Partnering FM residency programs agreed to implement the PrEP-Pro training intervention within their program’s curricula for residents/trainees. PrEP Champions, either faculty or residents, were purposefully selected through partnering program leadership.
Providers serving as PrEP Champions completed 4 hours of training over 2 sessions with study team physician-scientists using the PrEP Champion training tools developed and refined as described elsewhere.46,47 Didactic content covered how to conduct a comprehensive sexual history (tailored for adolescent patient populations), how to manage PrEP care, and how to be an effective PrEP Champion, including advocacy, teaching, mentorship, and problem-solving skills. PrEP Champions received training in curriculum delivery to equip them with skills to instruct their resident trainees. These training sessions, conducted in October 2023, launched the 6-month pilot.
After site activation with PrEP Champion trainings, PrEP Champions led two, 1-hour clinic-site educational sessions over a 1-month period, using the training tools provided to them with support from study staff. Sites had the flexibility to implement PrEP-Pro trainings according to their own preferences (ie, training all site residents or a select group).
All PrEP-Pro participants had access to a manual of resources and training materials (PrEP-Pro website), including study staff and investigator contact information, a peer PrEP Champion, recordings and files of the training sessions conducted by PrEP-Pro team members, and links to external sources.
Participating training programs worked with the academic research partner to implement the training intervention for all FM residents. Those attending the training sessions chose whether to participate in the study. To enroll, participants consented and completed the pre-training baseline questionnaire that included demographics and knowledge, behavior, and attitudes toward PrEP prescription. At the end of the 6-month pilot test, all trained residents were invited to complete a post-training questionnaire consisting of the same questions asked in the baseline questionnaire, with the addition of questions measuring acceptability and implementation of the intervention. Participants were paid $30 for each completed questionnaire.
PrEP Champions were asked to document all PrEP-related interactions and responsibilities within the clinical setting, including resident support, discussions with administrators, and resource provision. PrEP Champions were compensated $50 per hour for these activities based on self-report documented in the study-provided time log. To foster a community of practice, PrEP Champions were connected with peers in the study, allowing for discussions, troubleshooting, and shared learning. They received physical informational resources, including clinic flyers, patient educational pamphlets, and sexual history screening tools, to distribute within their clinical settings, as well as “Badge Buddies” (quick-reference cards). 43 PrEP Champions had access to a resource manual via a Google Sites webpage and ongoing support from study investigators as needed. Participants were also invited to attend two, 1-hour Zoom “check-in sessions” facilitated by Drs. Matthews and/or Elopre and Ms. Pratt from January to April 2024 to discuss their experiences with sexual history-taking and PrEP prescribing, address challenges, and receive feedback from peers and the study team.
Data Collection
Questionnaires
The baseline questionnaire captured socio-demographics (age, race, gender, post-graduate year, and faculty status), practice characteristics (patient population served), type of training program (university-affiliated, community-based, and private), volume of clients seen in clinic by the participant in the past week, proportion of clients who were Black, and qualitative categories (all of the time to none of the time) of frequency of sexual history assessment, STI testing, and HIV testing for these patient groups. Consistent with the COM-B framework, we assessed HIV epidemiology, PrEP knowledge, HIV and STI testing practices, and sexual history- and PrEP-related beliefs and attitudes.48-51
The exit questionnaire consisted of the same items about practice characteristics and behaviors, HIV epidemiology, PrEP knowledge, HIV and STI testing practices, and sexual history- and PrEP-related beliefs and attitudes.48-51 We also evaluated acceptability, appropriateness, and feasibility through the Evidence-Based Practice Acceptability scale, 52 Acceptability of Intervention Measure (AIM), Intervention Appropriateness Measure (IAM), and Feasibility of Intervention Measure (FIM). 53
Process Data
As an indication of feasibility and acceptability, we describe number of participants who completed baseline and exit questionnaires; completed at least 1 training, and contacted the PrEP Champion at least once in the quarter after training. For the PrEP champions, we describe hours logged supporting residents, and the proportion who participated in a check-in session.
EMR Data
We extracted PrEP (TDF/FTC, TAF/FTC, and CAB) prescriptions for people without a diagnosis of HIV or hepatitis B from the EMR for the practices in general and limited to the enrolled providers to evaluate the number of PrEP prescriptions, HIV tests, and STI testing for unique clients (in the 6 months before and after PrEP-Pro training). We describe the number of tests for STIs (chlamydia, gonorrhea, syphilis, and trichomonas) and HIV and PrEP prescription per unit population for the practices in general and limited to the trained providers during these time windows.
Analysis
We used McNemar’s tests to compare the proportion of participants who reported assessing sexual history, offering STI testing, and HIV testing at least some of the time to the referent patient groups at baseline and exit. We used Wilcoxon signed rank test to compare baseline and exit scores for sexual history- and PrEP-related beliefs and attitudes.48-51
We describe the EMR data as proof of concept for obtaining these data across sites for this pilot program.
Ethics
The protocol was approved by the Institutional Review Board of the University of Alabama at Birmingham (UAB; Birmingham, AL, USA; IRB#-300008567). Informed consent was obtained from all participants. Each residency program that served as a site in this study acknowledged their agreement to participate through program administrators and directors. Ethics approvals to obtain deidentified EMR data from each site were granted.
Results
Forty-six participants, including PrEP champions, across the 4 sites completed the enrollment questionnaire (and initial training) with a median age of 29 years (IRQ = 28, 34). Fifty-seven percent were men, 59% were White, 15% were Asian, 11% Latinx, and 7% were Black/African American. All described their primary practice as community-based, with about half identifying as university-affiliated. Eighty-nine percent of participants were residents (37% PGY1, 28% PGY2, and 24% PGY3); 11% were faculty (Table 1).
PrEP-Pro Participant (Including PrEP Champions) Demographics for N = 46 Completing Enrollment Questionnaire.

Abbreviation: PGY- post-graduate year.
All that apply selected. Description of patient population rurality was based on participant report.
Eight participants (17%) at baseline (N = 46) and 6 (19%) participants at exit (N = 32) answered all 5 HIV knowledge items correctly, reflecting understandings of local HIV epidemiology and a status neutral approach to HIV care and prevention (Motivation). Five participants (11%) at baseline (N = 46) and 14 (44%) participants at exit (N = 32) gave correct answers to at least 5 out of 7 questions about PrEP.
Among participants who completed both the baseline and exit questionnaires (N = 32), baseline HIV epidemiology knowledge remained the same, with 6 (19%) of participants answering all questions correctly both pre- and post-training. However, the proportion correctly answering PrEP knowledge questions increased, with 4 (13%) participants answering 5/7 questions correctly at baseline and 14 (44%) answering 5/7 correctly at exit.
At enrollment (N = 46 baseline survey responses), most participants had cared for 1 to 5 adolescents/young adults in their last typical workweek (N = 31/46, 67%) and had assessed a sexual history from at least some (some 41%, many 9%, most 24%, or all 7%) of their AGYW clients. Of the AGYW seen in clinic, 50% (N = 23/46) of participants reported that none had been tested for STIs, and 74% (N = 34/46) reported that none of the ABYM seen in clinic were tested for STIs. Most (N = 44/46, 96%) had not prescribed PrEP.
From baseline to exit, among those who completed both surveys (N = 32), there were modest increases in the proportion assessing sexual history (for AGYW), testing for STIs and HIV (for AGYW and ABYM; Behavior; Table 2).
Provider Behavior (Self-report) Conducted With Adolescent Girls and Young Women (AGYW) and Adolescent Boys and Young Men (ABYM) Seen in the Last Week (N = 32 Participants Who Completed Both Baseline and Exit Surveys).
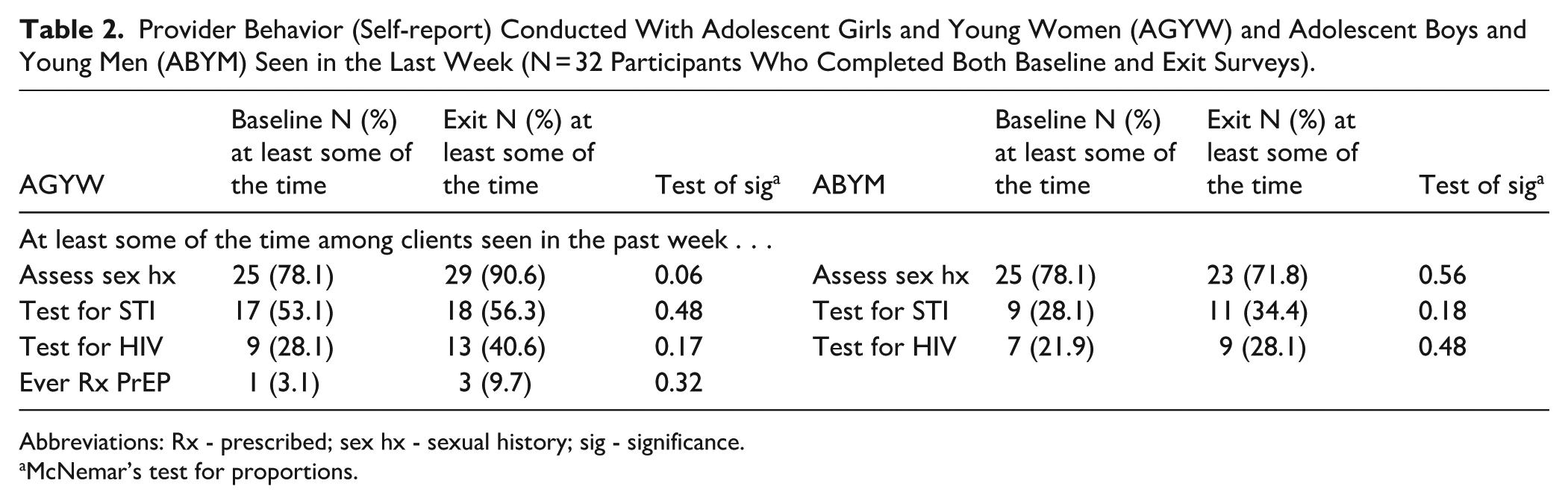
Abbreviations: Rx - prescribed; sex hx - sexual history; sig - significance.
McNemar’s test for proportions.
We did not observe changes in attitudes toward, barriers to, or prior training in sexual history assessment (Table 3). We did observe a significant increase in self-reported sexual history taking skills (P = .03, Capability), PrEP knowledge (P < .01, Capability), and in favorable attitudes toward PrEP (P < .01, Motivation).
PrEP-Pro Participant Score on Baseline and Exit Questionnaires (N = 32 Participants Who Completed Both Baseline and Exit Surveys).
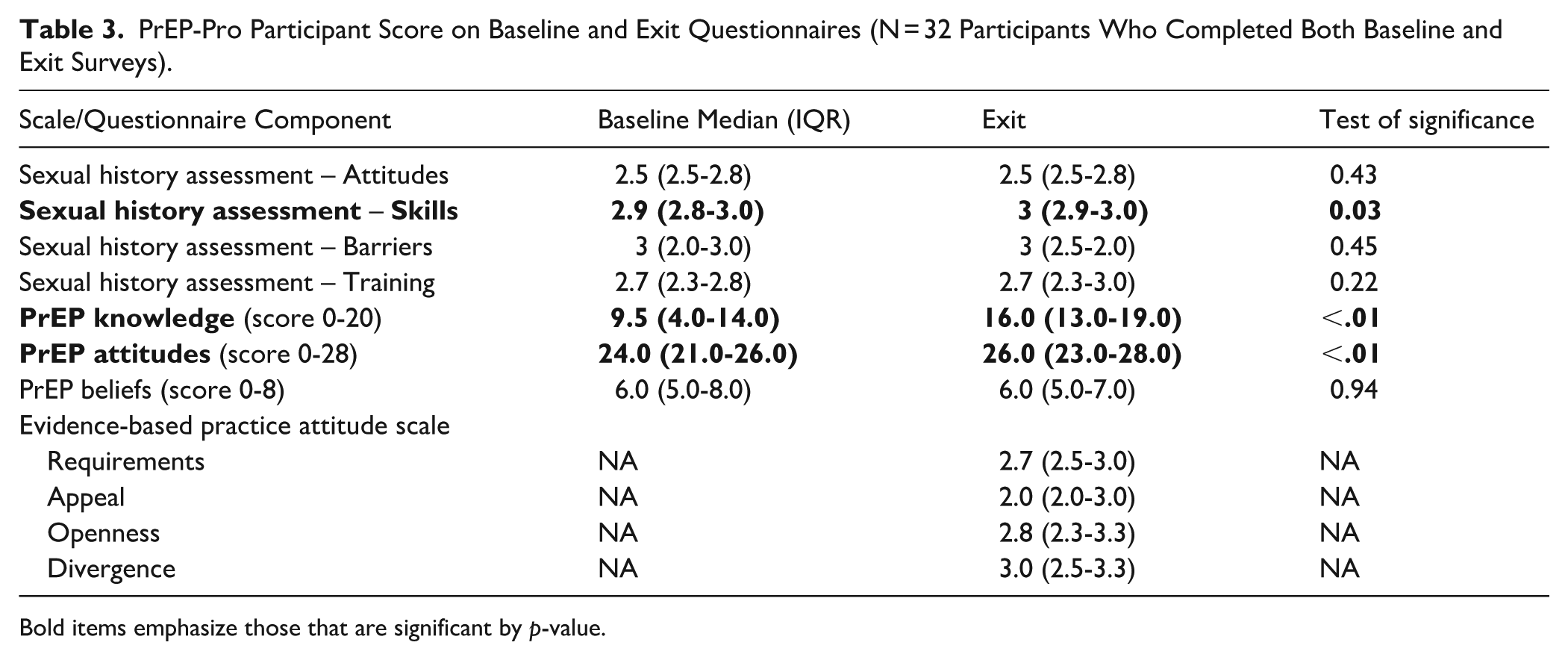
Bold items emphasize those that are significant by p-value.
Intervention Participation
Of the 8 PrEP Champions, 6 (75%) attended the first check-in session, and 4 (50%) attended both sessions. Among study participants, 70% (32/46) completed the exit questionnaire and 37% (17/46) completed the questionnaire section capturing implementation measures 53 and PrEP Champion support. Of those with complete data (n = 17), 59% (10/17) reported contacting a PrEP Champion at least once. PrEP Champions reported a combined total of 87 hours of engagement; 6 of the 8 Champions reported hours; 2 who did not were faculty. Among those reporting, the average number of hours was 9 (range: 6–14).
Among the 14 (30%) of 46 enrolled participants who did not complete the post-pilot exit questionnaire, some known reasons for incompletion included graduating from the residency program or moving to new jobs. In addition, some participants elected not to complete the exit questionnaire.
Due to a technical error in the questionnaire software, among the 32 exit questionnaire participants, 17 completed the acceptability, feasibility, and appropriateness measures. Among those, acceptability (mean [SD] = 4.31 [0.53]), appropriateness (4.25 [0.46]), and feasibility (4.28 [0.42]) were scored highly on a 5-point Likert scale.
Seventeen participants completed questions from the Evidence-Based Practice Attitude Scale, which measures attitudes toward adopting PrEP-Pro, scaled from 0 to 4 with 4 being most favorable. Scores (Table 3) suggest that participants are generally willing to adopt an evidence-based intervention/practice when required to do so by their supervisor, agency, or state (“Requirements”: mean score 2.8 out 4.0 [SD = 0.5]). They are generally willing to use interventions that have a treatment manual and to try new interventions to help their clients, including those developed by researchers, even if they are different than those they have utilized previously (“Openness”: mean score 2.8 out 4.0 [SD = 0.7]). Participants’ scores indicate they generally believe clinical experience is not more important than using manualized interventions and research is useful for developing treatment protocols (“Divergence”: mean score 3.0 out 4.0 [SD = 0.7]). Participants were less influenced to use PrEP-Pro by its intuitive appeal, use by colleagues, or because they felt they had enough training to use it correctly (“Appeal”: mean score 2.1 out 4.0 [SD = 1.2]).
Finally, we explored EMR data documenting HIV/STI testing and PrEP prescribing during 6 months prior to intervention start and 6 months during the intervention period (Table 4). These data were provided by 3 of the 4 clinical programs. For 1 program we were not able to secure site approval for data access. The data show variable baseline rates of HIV and STI testing, patient volume across sites, and low PrEP prescription both pre- and post-intervention (Table 4).
EMR Data to Evaluate PrEP-Pro-trained Provider Practices 6 months Pre- and Post-Intervention Pilot. a

Tests of significance for pre- and post-data were neither planned nor conducted as this pilot study was meant to evaluate feasibility of collecting these data and inform power for a future trial.
One site, not able to obtain EMR data.
Discussion
Our data show that a 6-month pilot trial of a theory-based intervention promoting PrEP prescription to adolescents and young adults, deployed among FM training programs in the U.S. Southeast, was acceptable and feasible. The program utilized a PrEP Champion model54,55 to accelerate dissemination of sexual health and PrEP education to faculty and trainees, with content focused on local HIV epidemiology, taking a sexual history, and PrEP prescribing. To support PrEP service delivery, we were attentive to adult learning principles, particularly minimizing cognitive load for medical residents by delivering targeted educational materials (eg, web-based content inclusive of sexual history videos with U.S. southern actors and content) and integrating practical, point-of-care tools (eg, badge buddies, pocket cards, sexual history screening tools, and patient-facing flyers) at each site.
Based on participation, engagement, and quantitative metrics, the intervention was acceptable and feasible. While not powered to detect differences in behavior, we observed an increase in sexual behavior assessment skills, PrEP knowledge, and PrEP attitudes among participating physicians. We observed non-significant trends toward increased STI testing, HIV testing, and PrEP prescription by self-report. EMR databases were explored to assess objective PrEP prescription outcomes; this process highlighted the opportunities and challenges in developing data-sharing agreements and analyzing data across different health systems. To our knowledge, this is the first study to pilot an intervention focused on training FM providers in HIV prevention care tailored for AGYW. Among primary care physicians, FM practitioners have the greatest reach into rural communities and provide crucial preventive care for underserved populations. 41 They also provide transitional care as children advance into late adolescence, often coincident with the onset of sexual activity.56-58 Therefore, this work showcases an important opportunity to optimize HIV prevention for broad populations through interventions focused on FM practitioners and trainees.
Sexual health and HIV prevention in primary care settings have been explored, but few training interventions combine sexual history elicitation and PrEP prescription and management for physician-trainees. To our knowledge, this is the first program of its kind designed for FM trainees. However, some studies explored primary care providers’ perceived knowledge gaps, finding that more training was needed on PrEP prescribing, indications, dosing, contraindications, adherence concerns, and side effects/adverse reactions59,60 – gaps which our intervention addressed. A study of residents’ and fellows’ confidence in prescribing PrEP found participants preferred to learn sexual health communication early in medical school and emphasized throughout training, with specific attention to prescribing PrEP confidentially. 61 Several studies have shown that PrEP training improves provider knowledge, confidence, and prescribing intentions. In Ohio, a 40-min case-based training for medical residents increased median PrEP knowledge from 44% to 89% and improved comfort prescribing PrEP (55.4%-91.4%). 62 A 1-hour session for internal medicine trainees in New York boosted beliefs in PrEP’s effectiveness, safety, and likelihood of prescribing within 6 months. 63 Similarly, a 3-part training for OB/GYNs significantly improved knowledge of HIV epidemiology, familiarity with PrEP trials, and comfort prescribing PrEP. 64 The PrEP-Pro study is unique in longitudinal assessment of knowledge and behavior. For a future trial, we show the feasibility of using EMR data to collect objective measures of impact on provider behavior.
Results from the Evidence-Based Practice Attitude Scale (EBPAS) highlight provider-level determinants of PrEP-Pro adoption that may inform future implementation strategy refinement. While participants demonstrated openness to new practices and alignment with evidence-based care, the relatively low Appeal subscale score suggests limited intuitive fit or emotional resonance. This finding is consistent with prior research showing that low appeal is a common early-phase barrier to uptake and is modifiable through intervention framing and peer demonstration. 65 Framed through the COM-B model, the EBPAS subscales – particularly Appeal and Openness – reflect underlying motivational factors that influence provider behavior and highlight targets for precision implementation strategies grounded in provider belief systems. 66
Of note, while our study focused on and was tailored to improve PrEP prescription among AGYW, we adopted a comprehensive sexual health training program inclusive of diverse racial/ethnic, sexual orientation, and gender identities. This strategy was adopted based on early feedback from our provider and AGYW community advisory boards who articulated that a primary training need among family medicine practitioners was on taking a sex-positive history that supported future dialog and provider trust. 43 In addition, prior research supports the association between PrEP prescription among primary care providers and greater confidence in taking a sexual history. 67 In our study, we observed significant increases in self-reported sexual history taking skills, PrEP knowledge, and in favorable attitudes toward PrEP. Additionally, a cross-sectional survey of 359 US providers assessing preferences for PrEP training suggest providers need support to take comprehensive sexual histories, inclusive of sexual and gender minority populations. 68 While this did not translate into increased PrEP prescriptions to AGYW at pilot sites, attaining knowledge and self-efficacy in sexual history skills is a likely prerequisite for future PrEP prescription assessed over a greater length of time in future trials with more expansive training on cultural humility and navigating confidentiality for AGYW patients to create an affirming clinical environment support of sexual health wellness.
This study has limitations including that small sample size, sampling of clinics across the state, and a short pilot phase (ie, 6-month post intervention) did not allow for assessment of effectiveness in improving PrEP prescription. However, preliminary data supporting greater comfort and self-efficacy in taking a sexual history and PrEP prescription is encouraging for future larger trials with FM residency programs. As there are a limited number of residency training programs in Alabama, there is the potential for selection bias related to which programs opted to participate in the pilot test. To mediate the potential for sampling bias, we contacted all FM residency programs in the state to invite them to participate. Finally, individual-level stigma among providers and the restrictive, prohibitive legal environment within the state are important barriers to PrEP provision that were outside the reach of this program. Subsequent phases should incorporate additional bias training, support programs in addressing upstream, environmental barriers to PrEP provision for AGYW, and include modular, on-demand content to promote self-directed learning and flexible, practice-relevant engagement.
Conclusions
In summary, AGYW living in the US Southeast face disparate risks for acquiring STIs, including HIV, and have several unique challenges in navigating healthcare systems to access sexual health services. FM providers are ideal implementers for PrEP as they care for populations across the lifespan and those living in rural communities. As such, an imperative first step to addressing the Southern HIV epidemic is furthering research focused on implementation of multi-component, theory-informed interventions addressing the multi-level determinants that hinder equitable healthcare of sexual health services to populations in greatest need.
Footnotes
Acknowledgements
We thank the participants, the participating sites and the leadership at these sites. We are also grateful to support from this project from Dr. Irf Asif and Mr. Ryan Outman (UAB Department of Family Medicine), Drs. Lacy Smith and Karen Dixon (Cahaba Family Medicine), and Dr. Bradley Green (Gadsden Regional Medicine Center Family Medicine Residency Program). We are also grateful to Children’s Hospital of Alabama for allowing us to film content for educational videos in their simulation center.
ORCID iDs
Ethical Considerations
The protocol was approved by the Institutional Review Board of the University of Alabama at Birmingham (UAB; Birmingham, AL, USA; IRB#-300008567). Each residency program that served as a site in this study acknowledged their agreement to participate through program administrators and directors. Ethics approvals to obtain deidentified EMR data from each site were granted.
Consent to Participate
Informed consent was obtained from all participants.
Consent for Publication
Not applicable.
Author Contributions
Madeline C. Pratt – data curation, formal analysis, investigation, project administration, resources, visualization, writing (original draft preparation), and writing (review and editing). Oluwaseyi O. Isehunwa – data curation, investigation, project administration, resources, and writing (review and editing). Lillian Klasen – writing (review and editing), management, and visualization. Vikas Gupta – methods, data collection, analysis interpretation, and writing (review and editing). Trupti Nadkar – methods, data collection, analysis interpretation, and writing (review and editing). Shivani Malhotra – methods, data collection, analysis interpretation, and writing (review and editing). Samantha V. Hill – conceptualization, methodology, and writing (review and editing). Tina Simpson – conceptualization, methodology, and writing (review and editing). Robin Gaines Lanzi – conceptualization, methodology, and writing (review and editing). Nicholas Van Wagoner – conceptualization, methodology, and writing (review and editing). Brook Hubner – investigation, project administration, resources, conceptualization, methodology, and writing (review and editing). Douglas Krakower – conceptualization, methodology, and writing (review and editing). Tara Wood – data curation, formal analysis, visualization, and writing (review and editing). Dustin Long – conceptualization, methods, formal analysis, visualization, and writing (review and editing). Latesha E. Elopre – conceptualization, methodology, data curation, formal analysis, funding acquisition, investigation, project administration, resources, visualization, writing (original draft preparation), and writing (review and editing). Lynn T. Matthews – conceptualization, methodology, data curation, formal analysis, funding acquisition, investigation, project administration, resources, visualization, writing (original draft preparation), and writing (review and editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institute of Mental Health, R34-MH12804 (MPIs Matthews/Elopre); K24-AI184259 (PI Matthews).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Lynn T. Matthews has received operational support from Gilead Sciences for unrelated projects. Douglas Krakower has conducted research with funding from Gilead and Merck to his institution, has received personal funds to develop medical education content from Medscape and UpToDate, Inc., and has received travel support from PrEP4All to attend a conference on a national PrEP plan. Latesha E. Elopre has received support from Merck Foundation for unrelated projects.