
Abstract
Objectives:
We used data from the Veterans Health Administration (VA) to examine rates of alcohol use disorder (AUD), insomnia disorder, and their co-occurrence in a national sample of Veterans prior to and during the COVID-19 pandemic.
Methods:
We analyzed VA electronic health record data for Veterans using VA care between March 2018 and March 2023 (N = 5.6-5.8 million). We identified AUD and insomnia disorder using ICD-10 codes and calculated diagnosis rates for each year. Results were stratified by sex, age, race, and ethnicity. We first examined whether rates significantly changed over time via mixed-models. To understand magnitude of change across time, we then calculated the total relative change in diagnostic rates from 2018 to 2023.
Results:
Approximately 5% of the sample had an AUD diagnosis, with rates staying relatively stable across years; around 6% to 8% of the sample had an insomnia disorder diagnosis, with rates increasing across years. The co-occurrence between AUD and insomnia disorder among the total sample ranged from 0.87% in 2018 to 2019 to 1.12% in 2022 to 2023. Among women Veterans, AUD diagnosis rates increased significantly across all racial and ethnic groups and for those aged 30 to 49 and 65+ years, while rates among men were mostly unchanged. Insomnia disorder diagnosis rates and their co-occurrence increased across all years for most men and women Veterans.
Conclusions:
Diagnosis rates increased for those most vulnerable to the negative health effects of AUD and insomnia (eg, women and older adults). Negative health outcomes could widen if access efforts do not take into account increasing diagnostic rates.
Introduction
Among Veterans, unhealthy alcohol use is common and a leading risk factor for disability and death.1,2 Insomnia disorder—a condition characterized by difficulties initiating and/or maintaining sleep that are accompanied by distress or impairments in functioning—is also common among Veterans and associated with risk of medical and psychiatric morbidity.3-6 The co-occurrence of unhealthy alcohol use (a spectrum ranging from drinking above recommended limits to meeting criteria for alcohol use disorder [AUD]) and insomnia is high: approximately 58% of adults with AUD report clinically significant insomnia symptoms. 7 Rates are possibly even higher in Veterans. 8 Importantly, insomnia and alcohol use alone and together are associated with increased risk for physical and mental health problems often treated in primary care (eg, hypertension and depression). 9
Stressful life events can impact the course and nature of both AUD and insomnia disorder. After the World Health Organization declared COVID-19 a pandemic on March 11, 2020, daily life changed dramatically for individuals nationwide (eg, teleworking, social distancing, school closures, etc.). Research thus began to examine changes in health behaviors, including alcohol use and sleep, during the COVID-19 pandemic (hereafter: the pandemic). 10
Evidence among US adults is mixed about whether unhealthy drinking increased during the pandemic. 11 Some research on non-Veteran populations suggests that unhealthy alcohol use increased over the first year of the pandemic 12 whereas other research found that drinking (both quantity and frequency) decreased. 10 Some self-report data suggests rates of AUD in Veterans stayed stable over the first year of the pandemic 13 or increased14-16 while Veterans Health Administration (VA) electronic health record (EHR) data suggest rates slightly decreased. 17 Other Veteran self-report data suggests that alcohol use declined overall over the first year of the pandemic and that women Veterans and Veterans identifying as Black, Hispanic, Asian, or Multiracial exhibited smaller decreases in unhealthy alcohol use but overall higher rates of alcohol use compared to men and White Veterans.
Longitudinal studies of administrative data suggest that prior to the pandemic, insomnia disorder diagnosis rates were increasing among Veterans.19,20 To our knowledge, few studies have evaluated EHR diagnosis rates over the course of the pandemic 21 ; however, survey studies provide some evidence to suggest rates may also have increased during this time. For instance, 1 nationally representative longitudinal study of Veterans found that nearly 12% of Veterans without insomnia symptoms pre-pandemic (November 2019) developed subthreshold or clinical insomnia symptoms during the pandemic (November 2020) 22 and 8% of Veterans with subthreshold insomnia symptoms pre-pandemic developed clinical insomnia symptoms during the pandemic. 22
Research on pandemic-related unhealthy alcohol use and insomnia prevalence rates in Veterans conducted up until this point share several limitations. First, existing studies primarily used survey methods (self-report), limiting the validity of diagnostic assessment of AUD and insomnia disorder. Second, results have primarily reported on changes in drinking behaviors or diagnostic rates over the first year of the pandemic, precluding conclusions about trends across multiple pandemic years. Last, no studies to our knowledge have examined changes in diagnostic co-occurrence between AUD and insomnia disorder over this time period.
Given historically high rates of comorbidity between AUD and insomnia in Veterans 8 and associations between alcohol, insomnia, and poor outcomes, more research is necessary to understand whether pre-pandemic rates will remit, maintain, or increase over time. This study uses VA EHR data to examine documented diagnostic rates of AUD, insomnia disorder, and their co-occurrence in a national sample of Veterans prior to and during the pandemic (March 11, 2018-March 10, 2023). Given previous mixed findings, we did not have a priori hypotheses about patterns of diagnostic rates over time but expected rates would differ by sex, age, and racial group.
Method
Data Source and Study Sample
We conducted a retrospective study of VA EHR data extracted from VA’s Corporate Data Warehouse. 23 The sample included Veterans ages 18 to 110 with ≥1 primary care visit at a VA facility between March 11, 2018 and March 10, 2023. Veteran patients were classified into cohorts for each year of the study (eg, March 11, 2018-March 10, 2019, etc.). Veterans with encounters in multiple years were included in the cohort for each year they had a qualifying encounter. All study procedures were approved by the VA Pittsburgh Healthcare System Institutional Review Board.
Study Variables
AUD and Insomnia Disorder were identified using International Classification of Diseases-Tenth Revision (ICD-10) codes F10.X (for AUD), and F51and G47 (for insomnia disorder). 24 In line with previous EHR studies, annual AUD and insomnia cases were identified by the presence of ≥1 corresponding ICD-10 code during that study year20,25-27; co-occurring AUD and insomnia disorder cases were identified by the presence of ≥1 AUD and ≥1 insomnia ICD code in each study year.
Sociodemographic information was extracted to characterize the sample and stratify diagnostic rates. Sex at birth is defined as man or woman. We calculated Veterans’ age at the first day of each study year and categorized into the following groups: 18 to 29, 30 to 49, 50 to 64, and ≥65 years. Race and ethnicity were categorized as: Black (non-Hispanic), White (non-Hispanic), Hispanic, and Other (non-Hispanic).
Statistical Analysis
We first describe sociodemographic characteristics of the sample (counts and frequencies). We then calculated rates of AUD diagnosis, insomnia disorder diagnosis, and their co-occurrence for each year in the study period and stratified results by sex and age group as well as by sex, race, and ethnicity. Guided by prior work, 26 we assessed trends over time by comparing yearly aggregates. We first explored the bivariate linear trend via correlation to evaluate the association of each condition with year and found a significant linear association for all models examining diagnostic trends across the whole sample and stratified by sex (P < .05). When examining models stratified by sex, age, and/or race/ethnicity, some trends were non-linear; for those models, we used a Glimmix model which accounts for non-normally distributed data. We thus conducted adjusted mixed-model regression analyses with a linear or non-linear distribution of diagnosis rates with a single continuous term for year as a predictor with values ranging from 2018 to 2022. As discussed, for granularity and interest, the regression model was repeated as an exploratory analysis for sex, race/ethnicity, and age to understand if rates changed significantly over time for these patient subgroups. We also calculated point estimates for each diagnostic rate for each year using the proportion of patients with diagnoses out of all patients in that study year. Next, we calculated the SD and 95% confidence interval estimates for the point estimates using all data combined. Then we computed the total relative change in diagnosis rates (%) for AUD, insomnia disorder, and their co-occurrence from 2018 (first year of study timeframe; March 11, 2018-March 10, 2019) to 2023 (last year of study timeframe; March 11, 2022-March 10, 2023) by using the formula ([diagnosis rate in 2022 − diagnosis rate in 2018]/diagnosis rate in 2018) × 100. 26 We used the total relative change formula to understand the magnitude of change in rates across time.
Results
Descriptives
Sample characteristics are reported in Table 1. Annual sample sizes ranged from ~5.6 to 5.8 million, approximately 90% of whom identified as male regardless of study year. Across years, the largest group were Veterans ages 65+ years and the smallest group were Veterans ages 18 to 29 years. More than half of Veterans using VA care across all years identified as White.
Characteristics of Veterans Using VA Healthcare From March 2018 to March 2023, Stratified by Sex, Age, Race, and Ethnicity.

Column total is the denominator for each respective row. Individuals categorized as Black, White, or Other were all identified as Non-Hispanic.
Diagnostic Rates Across Time
AUD, Insomnia Disorder, and their Co-Occurrence in the Overall Sample (Figure 1; Supplemental Table 1). Approximately 5% of the total sample had an AUD diagnosis, with rates staying relatively stable across years (β = .0006, 95% CI = −0.0008, 0.0020, P = .25); around 6% to 8% of the sample had an insomnia disorder diagnosis, with rates increasing across years (β = .005, 95% CI = 0.003, 0.007, P < .01). The co-occurrence between AUD and insomnia disorder among the total sample also increased across time, ranging from 0.87% in 2018 to 2019 to 1.12% in 2022 to 2023 (β = .001, 95% CI = 0.0003, 0.0010, P = .01).
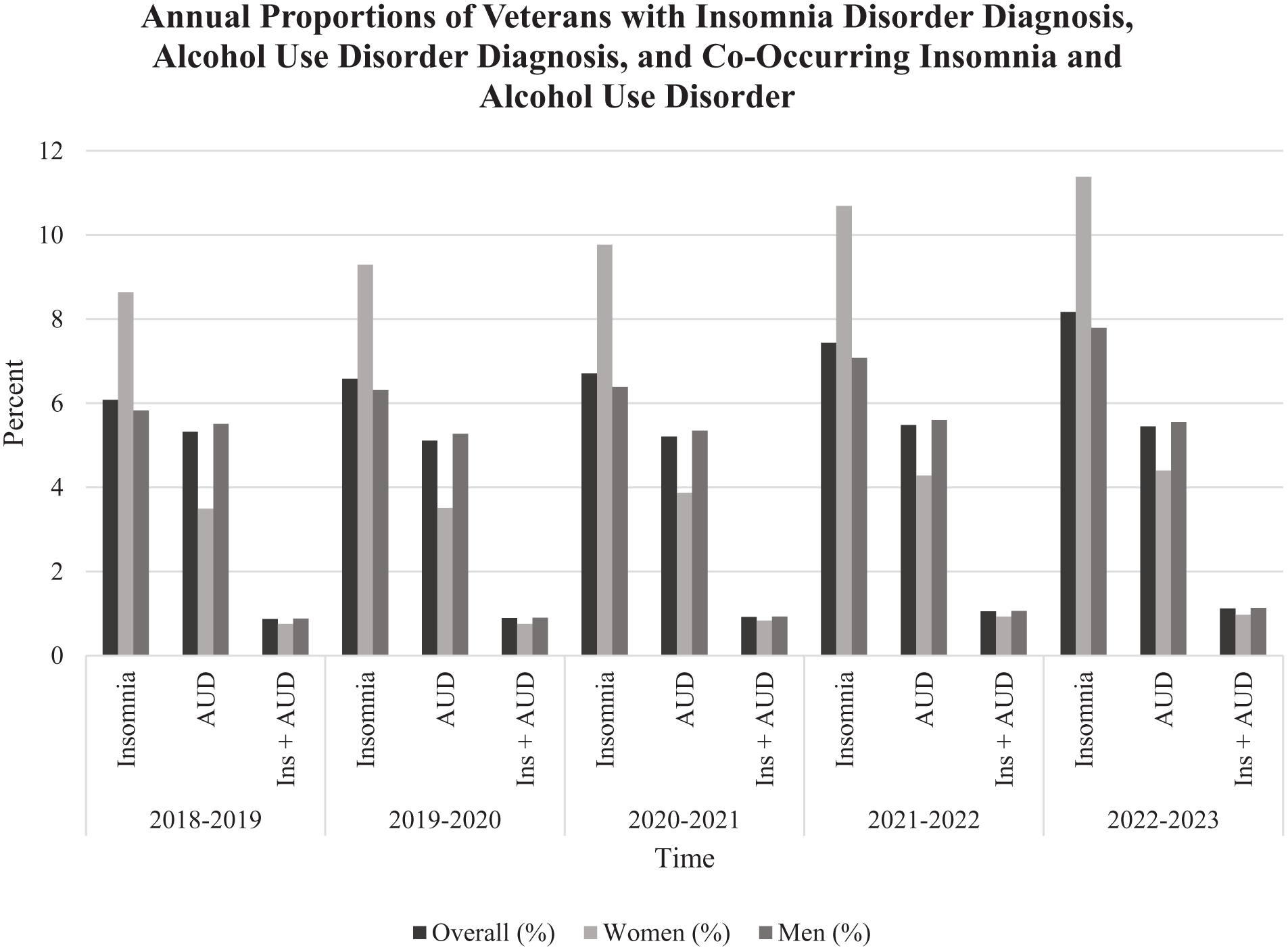
Annual proportions of veterans with insomnia disorder diagnosis, alcohol use disorder diagnosis, and co-occurring insomnia and alcohol use disorder.
AUD, Insomnia Disorder, and their Co-Occurrence Stratified by Sex and Age (Figure 2; Supplemental Table 1). Among women Veterans, rates of AUD increased but not significantly (β = .002, 95% CI = −0.0001, 0.0039, P = .06), whereas rates of insomnia disorder (β = .007, 95% CI = 0.006, 0.008, P < .01), and their co-occurrence increased significantly across years (β = .0006, 95% CI = 0.0003, 0.0009, P < .01). AUD rates for women ages 30 to 49 years (β = .002, 95% CI = 0.001, 0.002, P < .01) and those 65 years and older (β = .002, 95% CI = 0.0016, 0.0024, P < .01) significantly increased over time, whereas rates for those aged 18 to 29 and 50 to 64 years did not significantly change. Insomnia rates for all women, regardless of age, significantly increased across years (all P < .05). Co-occurring AUD and insomnia rates increased significantly across time for all women (all P < .05) except those 18 to 29 years.

Annual proportions of female veterans with insomnia disorder diagnosis, alcohol use disorder diagnosis, and co-occurring insomnia and alcohol use disorder by age group. Annual proportions of male veterans with insomnia disorder diagnosis, alcohol use disorder diagnosis, and co-occurring insomnia and alcohol use disorder by age group.
For men Veterans, rates of AUD diagnoses did not significantly change across study years (β = .0004, 95% CI = −0.0010, 0.0019, P = .43); this pattern of non-significance held when examining AUD rates by age group (all P-values > .05). Rates of insomnia disorder diagnoses (β = .005, 95% CI = 0.003, 0.007, P < .01) and their co-occurrence (β = .0007, 95% CI = 0.0003, 0.0010, P = .01) increased for men Veterans, including for all age groups except those 18 to 29 years whose rates of co-occurring insomnia and AUD did not significantly change across time (P > .05).
AUD, Insomnia, and their Co-Occurrence Stratified by Sex and Race and Ethnicity (Figure 3; Supplemental Table 2). Among women and across time, AUD diagnosis rates increased significantly for all race and ethnicities examined (all P-values < .05). Insomnia diagnosis rates also significantly increased across years among all race and ethnicities (all P-values < .05); co-occurring rates increased across time only for Black women Veterans (β = .0009, 95% CI = 0.0002, 0.0015, P = .02) and White women Veterans (β = .0005, 95% CI = 0.0001, 0.0009, P = .03).
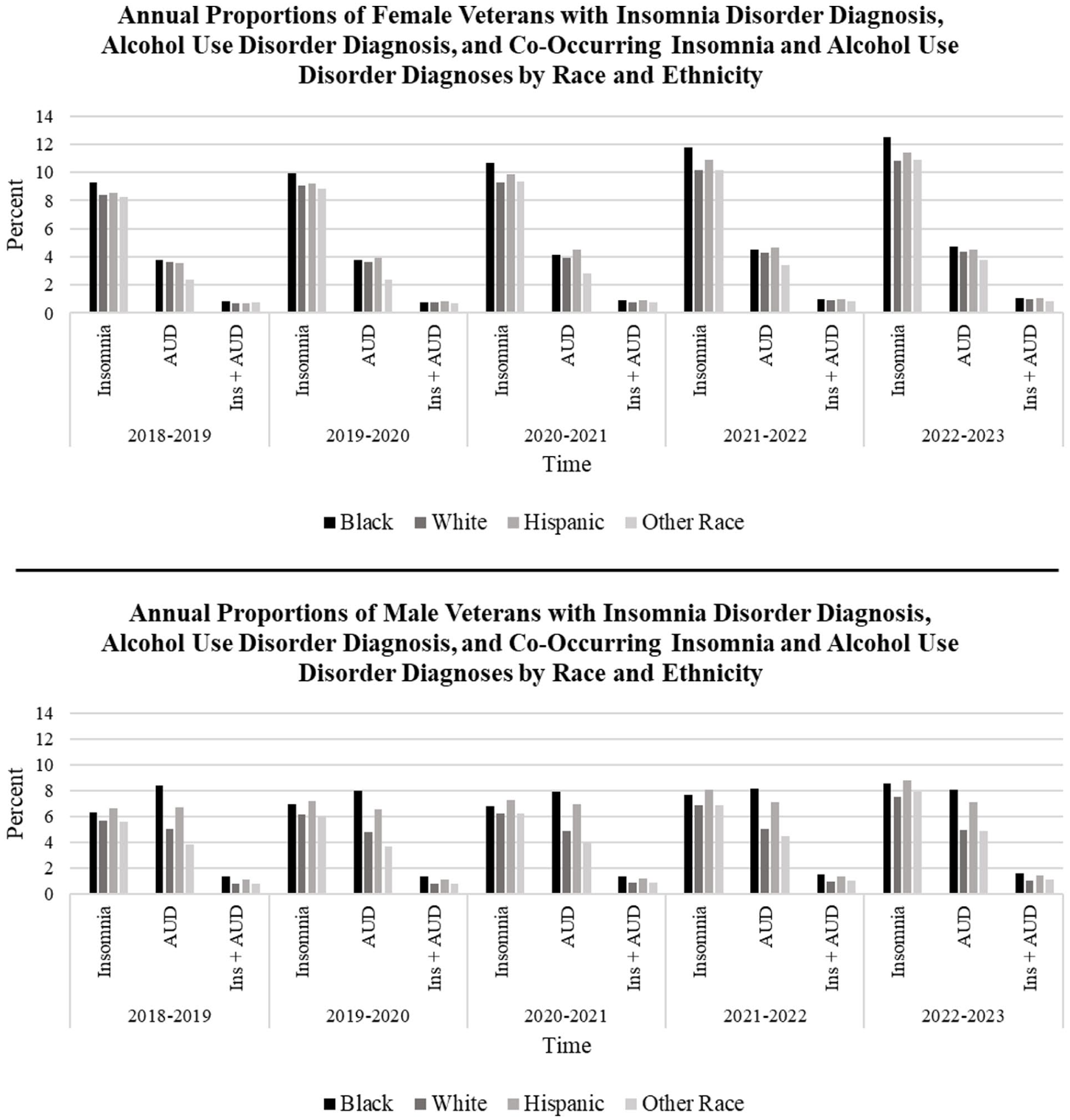
Annual proportions of female veterans with insomnia disorder diagnosis, alcohol use disorder diagnosis, and co-occurring insomnia and alcohol use disorder diagnoses by race and ethnicity. Annual proportions of male veterans with insomnia disorder diagnosis, alcohol use disorder diagnosis, and co-occurring insomnia and alcohol use disorder diagnoses by race and ethnicity.
Among men, AUD diagnosis rates did not significantly change across time for Black, White, or Hispanic Veterans; however, rates increased significantly for Veterans identified as Other race (β = .003, 95% CI = 0.001, 0.005, P = .02). However, insomnia diagnosis rates and co-occurring rates all increased significantly across time for races and ethnicities identified among men Veterans (all P-values < .05).
Total Relative Change in Diagnoses Across Time
Total Relative Change in Diagnostic Rates in the Overall Sample. Over the entire study period (2018-2023), AUD rates showed a relative overall increase of ~2% (from 5.32% to 5.45%); insomnia disorder diagnosis rates for the total sample evidenced a ~34% relative increase (from 6.08% to 8.17%) and co-occurring diagnosis rates showed a relative increase of ~29% (from .87% to 1.12%; see Table 2 for relative change percentages, see Supplemental Tables for annual proportions of diagnostic rates across time).
Total Relative Change in Insomnia Disorder, AUD, and their Co-Occurrence by Sex and Age from 2018 to 2023.
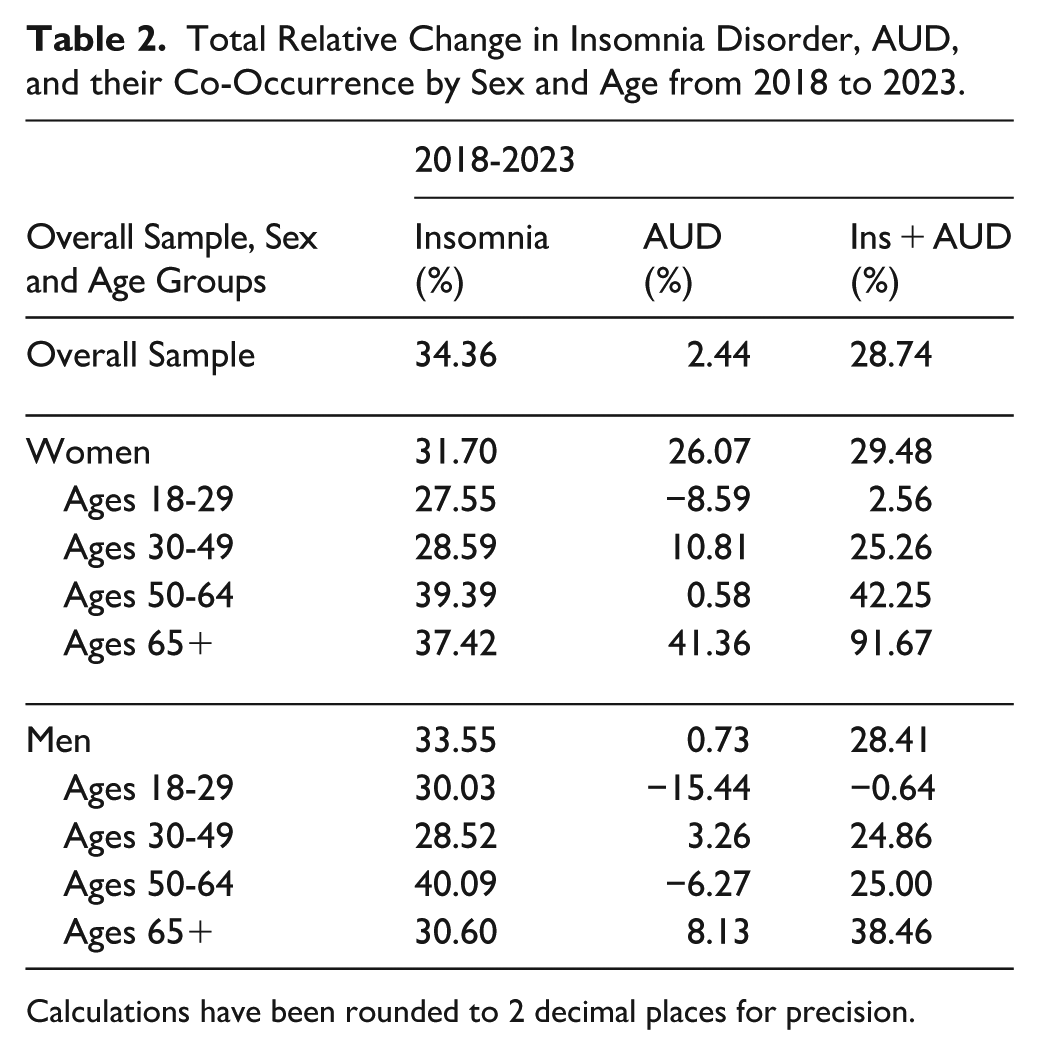
Calculations have been rounded to 2 decimal places for precision.
Total Relative Change in Diagnostic Rates Stratified by Sex and Age (Table 2). Among women Veterans, AUD diagnosis rates showed the most relative change for those aged 65+ years with a relative increase of 41.4% (from 1.91% to 2.70%); the second largest change was for those aged 30 to 49 years, with a relative increase of 10.8% (from 5.46% to 6.05%). Insomnia disorder diagnosis rates increased across the study period for all women Veterans, evidencing a 31.70% relative increase across time (from 8.64% to 11.38%). Relative increases in insomnia rates for women among all age groups ranged from 27.6% to 39.4%. Total relative increases in co-occurring AUD and insomnia diagnosis rates were the largest among women aged 65+ years (91.7% change from 0.24% to 0.46%).
Among men Veterans, there was little relative change in AUD diagnosis rates (.73%). However, insomnia disorder diagnosis rates showed more change for men Veterans regardless of age group. Insomnia rates evidenced a relative increase of 33.6% for all men (from 5.83% to 7.79%); relative increases in insomnia rates for all age groups ranged from 28.5% to 40.1% with men aged 50 to 64 years showing the most change. Men aged 65 years and older evidenced the largest increase for co-occurring insomnia and AUD (38.5% change from 0.39% to 0.54%); while men aged 18 to 29 years showed very little relative change across the study period (−0.64%).
Total Relative Change in Diagnostic Rates Stratified by Sex and Race and Ethnicity (see Table 3 for relative change percentages). Among women Veterans, AUD and insomnia disorder rates increased across time regardless of race or ethnicity. Relative change in AUD diagnosis rates was the highest for women identified as Other race (58.9% change from 2.36% to 3.75%) and lowest for White women (21.3% change from 3.62% to 4.39%). The total relative change in insomnia disorder diagnosis was highest among Black women (34.8% change from 9.26% to 12.48%) and lowest among White women (29.4% change from 8.38% to 10.84%). Total relative increases in co-occurring AUD and insomnia were observed across racial and ethnic groups; the highest increase occurred among Hispanic women (43.1% change from 0.72% to 1.03%).
Total Relative Change in Insomnia Disorder, AUD, and their Co-Occurrence by Sex and Race From 2018 to 2023.

Calculations have been rounded to 2 decimal places for precision.
Black and White men Veterans evidenced relative decreases in AUD diagnosis rates from 2018 to 2023 (−3.47% and −1.79%, respectively), while Hispanic men and men identified as Other race evidenced relative increases in AUD diagnosis rates from 2018 to 2023 (6.0% and 28.2%, respectively). Insomnia diagnosis rates increased across time for men regardless of race or ethnicity, with men identified as Other race evidencing the largest increase (40.57% relative change from 5.62% to 7.90%). Total relative increases in rates of co-occurring AUD and insomnia were the highest for Hispanic men (35.2% change from 1.08% to 1.46%) and lowest for Black men (20.3% change from 1.33% to 1.60%).
Discussion
The current study analyzed VA EHR data to estimate annual diagnosis rates of AUD, insomnia disorder, and their co-occurrence in a national sample of Veterans using VA care from 2018 to 2023. Across the overall sample, rates of insomnia disorder diagnoses and co-occurring insomnia and AUD increased annually, whereas rates of AUD diagnoses stayed relatively stable. AUD rates consistently increased among most subgroups of women examined, while rates among men were relatively unchanged. Insomnia disorder diagnosis rates increased for women and men across all age groups and racial and ethnic groups. Except for Veterans aged 18 to 29 years and women Veterans identified as Hispanic or Other race, all Veterans evidenced increases in co-occurring disorder rates across the study timeframe.
In the most recent study year (2022-2023), AUD diagnosis rates were lower than insomnia diagnoses overall, with 5.5% of the total sample having an AUD diagnosis, and were similar between men and women. Annual AUD diagnosis rates observed in the current study are comparable to recent work looking at substance use disorder diagnostic rates in the VA prior to the pandemic. 26 We observed that AUD diagnosis rates increased by 2% and differed substantially across time for women and men: rates increased by 26% for women and 0.73% for men. When stratified by sex and age, women aged 65+ years had the largest increases in AUD diagnosis rates compared to all other age groups. Given the increased likelihood of both health problems and prescription medication use at older ages, 28 the growth in AUD diagnoses for women 65 years and older is concerning. Men Veterans did not evidence significant change in AUD diagnoses across time among any age group although men aged 65+ years showed the largest relative increases in AUD diagnosis rates from 2023 compared to 2018 (8%). Findings align with epidemiological work showing that older adults and women have been steadily increasing their alcohol use over the past several years26,29,30 while younger adults have decreased their use over the last 40 years.29-31 There are likely multiple individual and societal-level reasons explaining increasing trends in unhealthy alcohol use among women and older adults. On an individual level, life transitions including retirement, loss of a spouse, and/or the shift in caregiving responsibilities may precipitate an increase in either stress/loneliness or decreased daily responsibilities which older adults, particularly women, might manage via increased alcohol use.32,33 On a societal level, increased targeted marketing toward older women, larger societal acceptance of drinking in older adults, messaging purporting the health benefits of alcohol, and the legalization of cannabis in many parts of the U.S. may be associated with an increase in unhealthy alcohol use within this age group. 30
AUD diagnoses increased at relatively similar rates for Black, White, and Hispanic women and more drastically for women identified as Other race. The increase in AUD diagnosis rates across racial and ethnic groups for women Veterans aligns with both Veteran and non-Veteran data showing general increases in unhealthy alcohol use and AUD rates among women in the U.S. prior to the pandemic.12,26,29,34 In contrast, AUD diagnosis rates remained mostly stable across time for men; relative change from 2018 to 2023 indicated that rates fell for Black and White men, while increasing slightly for Hispanic men and men identified as Other race. Overall, AUD rates for Black and Hispanic men were higher across study years compared to White men and those identified as Other race. This finding is consistent with other recent VA data, which found that Black and Hispanic Veterans had a higher likelihood of an AUD diagnosis compared to White Veterans despite similar consumption rates. 35 Given the possible bias occurring in diagnosing AUD among minoritized groups, future work should investigate reasons for fluctuations in diagnostic rates by racial group. For instance, clinicians may unconsciously expect AUD to be more prevalent in certain racial/ethnic groups, leading to overdiagnosis in some populations and underdiagnosis in others. These expectations could be influenced by internalized biases, stereotypes, and/or prior experiences.36,37 Clinicians may avoid diagnosing AUD in certain racial/ethnic Veteran patients due to concerns about stigmatization or legal consequences. Social determinants of health could also impact differential diagnostic rates, as these stressors (eg, economic instability, neighborhood safety, and access to care) often disproportionately affect certain racial/ethnic groups which might contribute to increased risk of AUD and differential diagnoses, independent of actual consumption rates. 38
Annual insomnia disorder diagnosis rates in the total sample ranged from 6% to 8%, evidencing a total relative change of about 34%. Diagnosis rates in the current study are higher than those from a prior study that applied more stringent criteria for insomnia disorder case identification during an earlier timeframe 19 and slightly lower than those from a more recent study that defined insomnia cases similarly but spanned multiple diagnostic coding systems). 20 In our study sample, insomnia disorder diagnoses increased to varying degrees across sexes, age groups, and racial and ethnic groups. For instance, annual insomnia disorder diagnosis rates were consistently higher in women Veterans compared to men Veterans, a finding that aligns with literature identifying sex differences in insomnia disorder risk. 39 Among women Veterans, annual insomnia disorder diagnosis rates were highest among those ages 30 to 49 years and lowest among those ages 65+ years. For men, highest insomnia disorder diagnosis rates were observed among those ages 18 to 29 and 30 to 49 years (depending on the year) and rates were lowest among those ages 65+ years. The finding that, across sexes, insomnia diagnosis rates were lowest among people ages 65+ years and higher in younger to middle adult age groups aligns with prior VA EHR studies. 40 These observations may reflect increased insomnia prevalence (eg, due to developmental factors), reduced stigma around discussing insomnia concerns, or greater awareness of insomnia symptoms among patients and clinicians. Future studies are needed to determine if there is evidence to support these speculations.
Among women Veterans, Black women had the highest rates of insomnia diagnoses and the largest relative increase in insomnia diagnosis rates over time. Among men, insomnia disorder diagnosis rates were highest for Hispanic Veterans compared to other racial and ethnic groups. Although research regarding disparities in insomnia disorder has been somewhat inconsistent, 41 results from the current study point to potential racial and ethnic disparities in insomnia disorder diagnoses among Veterans. As discussed above regarding differential AUD diagnostic rates, multiple factors at multiple levels (eg, individual, social, environmental, institutional, and systemic) may contribute to the identified racial and ethnic differences; future work should focus on identifying and clarifying the nature of these contributors in order to address them.42-45
Across study years and sociodemographic characteristics, rates of co-occurring insomnia disorder and AUD diagnoses were lower than rates of insomnia disorder or AUD diagnoses alone. Yet, the co-occurrence of insomnia disorder and AUD diagnoses increased significantly over the 5-year study timeframe in the overall sample, and across sexes, most age groups, and most racial and ethnic groups. This relative increase in co-occurring disorders is concerning for several reasons. First, insomnia and AUD each carry risks to physical health, mental health, and functioning; such risks may be compounded when these conditions co-occur.8,46 Second, diagnosis rates via EHR may underestimate the true prevalence of co-occurring insomnia disorder and AUD. Historically, insomnia had been considered secondary to, rather than comorbid with, other medical and psychiatric disorders 47 ; this characterization may translate to symptoms of insomnia being characterized solely as a consequence or symptom of AUD, rather than comorbid insomnia disorder, resulting in a person only receiving an AUD diagnosis. Including standardized and psychometrically validated diagnostic assessments within the EHR and improving integration of behavioral health care clinicians into primary care teams could help improve screening, diagnostic accuracy, documentation, and subsequent treatment access for these disorders. 48
Despite this study’s strengths, results should be interpreted in light of the following limitations. First, this study sought to understand trends in diagnoses across cohorts of Veteran patients; thus, results provide diagnosis rates between study years and not within patients over time. Second, our reliance on VA administrative data, which may be impacted by under-coding or miscoding, may have resulted in misclassification of some insomnia or AUD diagnoses. For example, prior work suggests that insomnia and AUD often go undetected and are under-diagnosed.40,49-52 Thus, rates presented here may not be equivalent to prevalence rates in the general Veteran population. Relatedly, our criterion for diagnostic classification could have identified patients who, with more specific criteria, may not meet diagnostic thresholds. However, given the study aims and our awareness that these conditions are often under-diagnosed, we expected that a more highly sensitive inclusion criterion may better estimate true positive rates of these disorders. An additional consideration regarding these data is that multiple phenomena may underlie the observed relative changes in diagnosis rates. For example, observed changes may represent increases over time of the proportion of Veterans living with insomnia disorder and/or AUD, or a positive change in the reporting, detection, and documentation of these diagnoses. To our knowledge, system-wide (eg, clinical reminder) changes to screening for or diagnosing/identifying AUD or insomnia did not occur during the study period. However, VA/DoD clinical guidelines for the management of chronic insomnia disorder and obstructive sleep apnea and for substance use disorders (including AUD) were updated in 2019 and 2021, respectively.53,54 These updated guidelines could have increased awareness and improved documentation of insomnia and AUD diagnoses. It is also possible that expansion of the VA sleep telemedicine programs 55 and increased hiring for mental health-related personnel56,57 could have improved efforts to identify cases of insomnia and AUD. These empirical questions could not be addressed with the current study’s data. It is possible that observed diagnosis rates may reflect better diagnostician efforts and/or true rises in incidence of these disorders. Thus, given the nature of these data, we can conclude diagnostic rates are changing but cannot determine the root causes of these changes. Finally, we are unable to make definitive conclusions regarding diagnosis rates among Veterans categorized as Other race, as this group consists of individuals who identify as Asian/Asian American, Native Hawaiian/Pacific Islander, American Indian/Native American, and possibly other races not easily identifiable in the EHR. Future work should further classify racial groups to better understand changes in diagnosis rates among minoritized populations.
Conclusions
Between March 2018 and March 2023, annual rates of insomnia disorder diagnoses and co-occurring insomnia disorder and AUD diagnoses increased among Veterans engaged in VA care; total relative increases, though to a lesser extent, were also observed for AUD diagnoses. Alone, both insomnia disorder and AUD can have severe negative consequences for health and overall well-being; when they co-occur, the deleterious effects of each may be compounded. The current findings could help inform allocation of resources (eg, increasing access to behavioral health clinicians, more training of primary care physicians in alcohol screening and brief interventions) for those providing healthcare to Veterans. Findings may also inform policy. Given VA’s reach as the largest integrated healthcare system in the U.S., the implementation and dissemination of standardized clinical assessment tools via the EHR (eg, checklists assessing diagnostic criteria for AUD, 58 insomnia, etc.) could improve diagnostic accuracy and better match prevalence rates seen in epidemiological studies. It will be critical to consider the identified sex, age, race, and ethnicity differences in diagnosis rates as the Veteran population continues to age and the number of women Veterans and Veterans of color grows. 59 Disparities in healthcare for minoritized patients with unhealthy alcohol use25,60 and insomnia disorder already exist 61 and could widen if access efforts do not take into account increasing diagnostic rates.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251392790 – Supplemental material for Diagnostic Rates of Alcohol Use Disorder, Insomnia Disorder, and Their Co-Occurrence in the Veterans Health Administration From 2018 to 2023
Supplemental material, sj-docx-1-jpc-10.1177_21501319251392790 for Diagnostic Rates of Alcohol Use Disorder, Insomnia Disorder, and Their Co-Occurrence in the Veterans Health Administration From 2018 to 2023 by Rachel L. Bachrach, Deirdre A. Quinn, Monique Boudreaux-Kelly, Shannon R. Mitchell, Karley Atchison and Caitlan A. Tighe in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We would also like to thank Dr. Jon Walker for his help extracting the data for the current study.
Author Note
The contents of this work do not represent the views of the Department of Veterans Affairs, Department of Defense, or the U.S. Government. Because several authors of this manuscript are employees of the U.S. Government and contributed to this manuscript as part of their official duties, the work is not subject to US copyright.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material is the result of work supported by a 2022 Medical Education and Patient Safety Award (Veterans Health Foundation, Pittsburgh, PA; mPIs: Bachrach & Tighe). Dr. Bachrach was also supported by a VA Career Development Award funded by Health Systems Research (CDA 20-057/IK2HX003087). Dr. Quinn is supported by a VA Career Development Award funded by Health Systems Research (CDA 20-224/IK2HX003327). During a portion of the study period, Dr. Tighe was supported by Career Development/Capacity Building Award Number IK2 RX003393 from the United States (U.S.) Department of Veterans Affairs Rehabilitation R&D (Rehab RD) Service. This material is also partially the result of work supported with resources and the use of facilities at the VISN 4 Mental Illness Research, Education, and Clinical Center at the VA Pittsburgh Healthcare System and the Center for Clinical Management Research at the VA Ann Arbor Healthcare System.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.