
Abstract
Background:
Despite the critical role of dietitians in supporting diabetes management through nutrition education, attendance at dietetics consultations remains suboptimal. Although the Arab Gulf Region has one of the highest prevalence rates of diabetes globally, there is a lack of research investigating the barriers and facilitators influencing both diabetes management and participation in dietetics consultations in this region. This study explored patients’ perspectives on diabetes nutrition management within the framework of self-regulation and self-efficacy constructs of the Social Cognitive Theory (SCT) and their suggestions for improving patient attendance in dietitian-led nutrition counseling sessions.
Methods:
Audio recordings of semi-structured interviews with 44 adults attending a diabetes clinic in the United Arab Emirates (UAE) were transcribed in Arabic, translated into English, and thematically analyzed to examine the participants’ self-management strategies, self-efficacy beliefs, and suggestions for improving attendance at dietitian-led nutrition counseling sessions.
Results:
Five themes emerged: barriers to diabetes self-management, diabetes self-management practices, high self-efficacy, low self-efficacy, and suggestions for improving attendance at dietitian nutrition counseling. Barriers included time constraints, scheduling issues, socio-cultural factors, health status, and nutrition counseling quality. Confidence levels varied, with some patients requiring reminders or additional information. Suggested improvements included coordinated appointments, reminders, remote sessions, and enhancing the quality of nutrition counseling.
Conclusion:
Addressing personal, social, and visit scheduling barriers may improve attendance and support effective diabetes management.
Keywords
Introduction
Diabetes self-management education (DSME) is fundamental to diabetes treatment1,2 and empowers individuals to make informed decisions about their lifestyle. DMSE leads to improved clinical outcomes, including reduced hemoglobin A1c levels, as well as enhanced quality of life, better coping mechanisms, and lower costs. A multi-disciplinary approach, including dietitians, is recommended for effective diabetes self-management education. 3 Medical nutrition therapy provided by registered dietitian nutritionists is a critical component of diabetes management.3,4 Indeed, several randomized controlled trials demonstrated that dietitian-led nutrition counseling improved glycemic control in patients with diabetes.5,6 Therefore, current clinical guidelines emphasize that dietitians play a key role in educating and guiding patients with diabetes toward optimal nutritional practices and behavioral change for effective diabetes management. 7
Bandura’s social cognitive theory (SCT) is a significant framework used to facilitate behavioral change. 8 SCT involves the reciprocal interactions between personal, environmental, and behavioral factors. 9 It describes how people operate and behave psychologically, with environmental influences significantly impacting motivation, learning, self-efficacy, and self-regulation.10,11 Self-regulation, one of the main concepts of SCT, involves managing one’s behavior with the help of planning, setting goals, and self-monitoring to control it. Self-efficacy, a critical factor, significantly impacts effective self-care behaviors among individuals with diabetes.12,13
Self-efficacy beliefs influence individuals’ confidence in adhering to dietary advice and self-care. However, research indicates that certain factors hinder the effectiveness of nutrition counseling, preventing optimal self-efficacy and self-regulation in individuals with diabetes, which are referred to as “barriers.” 7 On the other hand, some factors facilitate the successful implementation of self-regulation and self-efficacy practices, referred to as “enablers.” 7 These enablers and barriers impact DMSE, influencing how decisions about self-management are made by the patient. 7
The Arab Gulf Region has one of the highest prevalences of diabetes in the world. 14 According to the International Diabetes Federation (IDF), the United Arab Emirates (UAE) had an age-adjusted comparative prevalence of diabetes of 16.4% in 2021 and a projected prevalence of 17.2% in 2030. 14 However, very few studies have examined diabetes self-management-related barriers from the perspectives of Arab populations in the region 15 and globally.16-19 In the UAE, diabetes management clinics provide comprehensive health services, including nutrition counseling by licensed dietitians. However, patients’ attendance at dietetics consultations is often suboptimal, even when recommended by their physicians. In 2006, 46% of patients with diabetes attending outpatient clinics in Al Ain, United Arab Emirates, reported that they had never consulted a dietitian since their diagnosis. 20 Infrequent patient-provider contacts in outpatient clinics may not support patients with the complex demands of self-care required in managing a chronic disease such as diabetes. In the Arab Gulf countries, including the UAE, food constitutes an essential component of their cultural identity and social interaction. Traditional dishes are frequently consumed during both routine meals and special occasions. Communal eating is customary and reflects values of generosity and social connection. However, these practices may present challenges to adherence to individualized dietary plans, as declining offered food can be perceived as disrespectful, and modifications to traditional meals are not always socially acceptable. Therefore, there is a need to identify the obstacles that influence regular attendance at nutrition counseling sessions and adherence to dietitian nutrition advice within the socio-cultural context of the Arab Gulf region. Therefore, the aim of this study was to explore the perspectives of adults with diabetes attending a specialized diabetes center in the UAE, regarding diabetes nutrition management and their suggestions for improving patients’ attendance in dietitian-led nutrition counseling sessions.
The study was conducted within the SCT framework, specifically focusing on the constructs of self-regulation and self-efficacy.
Methodology
Study Design
This qualitative study involved individual interviews of adult patients attending a major specialized outpatient diabetes management clinic in Al Ain, United Arab Emirates. Qualitative research enables the exploration of questions that cannot be quantified, providing a deeper understanding of human experiences. 21 This approach enhances our understanding of human experiences, emotions, and practical applications in real-world settings. 22 Investigating patients’ perspectives on non-attendance and adherence to nutrition counseling at a specialized diabetes management clinic in the UAE, this study employed Bandura’s self-regulation and self-efficacy constructs of the SCT. 8 Self-regulation strategies in diabetes self-management include self-monitoring of blood glucose (SMBG), making healthier dietary choices, engaging in regular exercise, practicing effective stress management, adhering to medication, setting goals, and planning, all of which contribute to optimal glycemic control. 23
Qualitative interviews were deemed most appropriate in obtaining participant perspectives, opinions, and attitudes about their nutrition-related diabetes self-management strategies (self-regulation) and their confidence in managing their diabetes effectively (self-efficacy). These patient perspectives will be useful in improving patients’ attendance at dietitian-led nutrition counseling sessions. The study was conducted between October 2022 and March 2023.
Ethical Considerations
The ethical approval was provided by the Imperial College London Diabetes Centre Research Ethics Committee (approval #: IREC 080). Participants were informed that their participation in the project was voluntary and that all the information collected would remain anonymous and confidential. Prior to the data collection, all the participants provided oral and written informed consent and agreed to have the interview audio-recorded within the clinic premises. All study methods were conducted in accordance with the guidelines and regulations of the (anonymized) Research Ethics Committee.
Participant Recruitment
Adults with type 1 or type 2 diabetes attending a diabetes management clinic in Al Ain, United Arab Emirates, were invited to participate in a single interview. The inclusion criteria were adult males and females aged 19 years and older with type 1 or type 2 diabetes receiving diabetes management care in the target clinic. Patients with other types of diabetes were excluded. This purposive sampling allows for recruiting participants with pre-determined criteria. 24 Senior students majoring in dietetics invited patients with diabetes in the clinic’s waiting area to participate in the study. Participant recruitment was carried out in close collaboration with clinic staff. Receptionists assisted in identifying eligible participants from attendance registration and notified the research assistants, while physicians informed their patients about the study. In addition, clinic staff facilitated the process by arranging a private room for the interviews. After obtaining signed informed consent from the patients, the clinic retrieved the patients’ type of diabetes, age, BMI, diabetes duration, diabetes treatment type, and whether they had visited a dietitian within the past 6 months from their medical records. This recruitment strategy was used to ensure adherence to the project’s ethical approval and the study’s inclusion criteria. All the participants were Emirati nationals with government-funded health insurance that fully covered medical care, including dietitian-provided nutrition counseling services.
Setting
The study was conducted at an outpatient facility in Al Ain, United Arab Emirates, specializing in the treatment and education of diabetes and related complications. Al Ain is the fourth largest city in the UAE and the second largest in the Emirate of Abu Dhabi, with a population of 986 910 according to the 2024 Abu Dhabi Emirate census. 25 The facility provides comprehensive healthcare services, including nutrition counseling delivered by licensed dietitians. It serves both Emirati and non-Emirati nationals, with Emirati nationals representing the majority of patients.
Data Collection
Data were collected through individual, semi-structured interviews using a discussion guide focused on 3 areas: diabetes self-management strategies (3 key questions), patients’ confidence in managing diabetes (3 questions), and suggestions to improve attendance at nutrition counseling sessions (1 question). The discussion guide is available as supplementary material (S1). The guide, based on Social Cognitive Theory constructs of self-regulation and self-efficacy, was developed in English by 4 members of the research team and then translated into Arabic by bilingual dietetics students, who reviewed it for accuracy with a native Arabic-speaking member of the research team. Pre-testing the discussion guide with 4 clinic patients led to minor wording adjustments for clarity.
Trained 2 female undergraduate students in nutrition and dietetics (the third and the sixth author), conducted the interviews in Arabic. Each session involved 1 interviewer and 1 observer, both of whom had no prior relationship with participants. Before each interview, the facilitator explained the purpose, assured participants of data confidentiality, and reminded them of their right not to answer any questions or to discontinue the interview at any time. The facilitator emphasized the voluntary nature of participation and the confidentiality of the information shared. She also clarified that she had no affiliation with the health center, encouraging participants to share their opinions freely. The interviews were conducted in-person in a private office at the diabetes center, with each interview lasting 15 to 30 min. The facilitator followed the discussion guide to minimize interviewer bias, supplementing it with additional probes as needed for clarification. All interviews were audio-recorded.
Participant information, including age, BMI, diabetes duration, and diabetes treatment type, and whether they have visited the dietitian within the past 6 months, was obtained from medical records. Preliminary analysis of the first 23 interviews guided further exploration. Recruitment ended after 44 interviews, when no new information related to the topic emerged from the discussions, indicating data saturation.26,27
Data Analysis
Inductive thematic analysis was used to analyze the data to derive the themes. 28 The transcripts of the interviews were imported into NVivo-12 software (QSR International). Text-based thematic analysis based on the constant comparative method, in which each item is checked or compared with the rest of the data, was used. 29 Concurrent data collection and analysis were performed to identify initial codes and categories as the interviews progressed. 30 The interview questions were refined with additional probes based on this preliminary analysis, which was in line with the qualitative research methodology. The preliminary analysis of the first 23 interviews revealed that most participants had not visited a dietitian for nutrition counseling in the previous 6 months; thus, recruitment began to focus on patients who had visited a dietitian within the last 6 months.
The codes were constantly compared and then grouped into themes and sub-themes. Two coders (the third and sixth authors) independently coded the data. Two other coders (the fourth and fifth authors) reviewed the appropriateness of the coding categories and the emerging themes in consultation with the first author. Differences were discussed and resolved to reach a consensus.
Quality Assurance
The interviews were audio-recorded and transcribed verbatim in Arabic by the interviewers, who also translated the transcripts into English. Two additional researchers independently verified the transcripts against the recordings. Twenty translated interviews were randomly selected for independent review against the original Arabic transcripts by team members not involved in data collection. Clarifications were made by consulting interviewers and reviewing recordings as needed. The first author, an experienced qualitative researcher, reviewed the appropriateness of the codes assigned to the themes and sub-themes. The participant quotes were included in the results section to increase credibility. We included the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist. 31 A copy of the completed COREQ checklist is available as Supplementary Material (S-2) to provide additional clarity on the methods followed during the study.
Results
Interview Participants
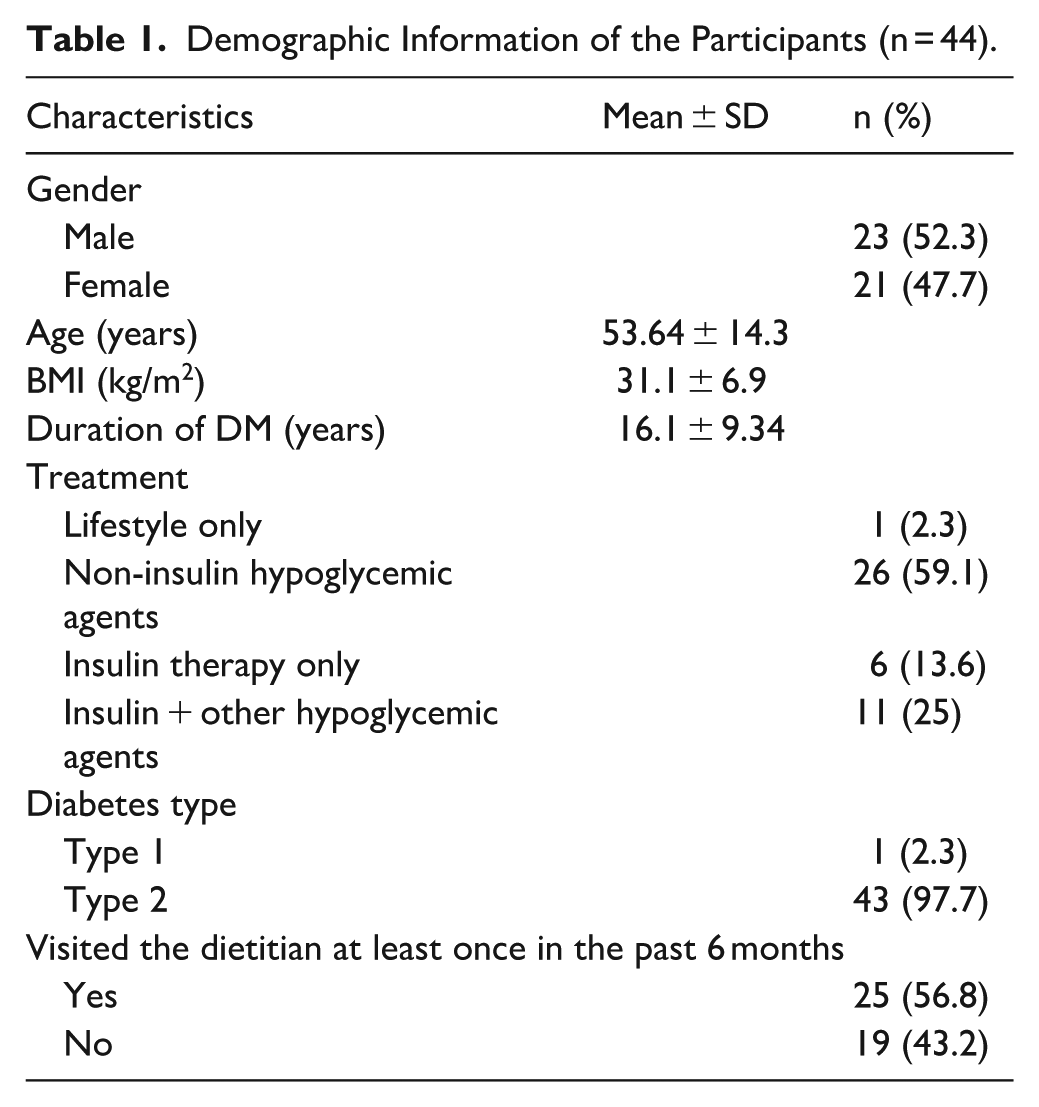
Table 1 presents demographic and clinical information of the 44 participants. The mean age of participants was 53.64 ± 14.31 years (range 20-73 years). Of the 44 participants (43 of whom had type 2 diabetes), only 25 (56.8%) visited the dietitian at least once in the past 6 months.
Demographic Information of the Participants (n = 44).
Themes and Sub-themes
The 5 main themes and their related sub-themes, as identified through the thematic analysis of interviews, are presented in Table 2. The 5 main themes were (1) diabetes self-management barriers, (2) diabetes self-management practices, (3) high self-efficacy, (4) low self-efficacy, and (5) Suggestions to improve patient attendance to dietitian nutrition counseling sessions.
Themes and Sub-themes.

Theme 1: Diabetes Self-Management Barriers
Participants discussed the challenges encountered when attempting to incorporate a dietitian’s advice into their daily lives and the reasons for missed appointments with the dietitian. They also cited factors such as scheduling conflicts, time constraints, and preference for convenient appointments. In the presentation of participant quotes, patients who had consulted a dietitian within the 6 months preceding the interview date are indicated as VD (visited dietitian) and those who did not as NVD (not visited dietitian).
Barriers to Adherence to Appointments
Participants discussed some of the challenges they face in attending appointments with the dietitian. They cited the reasons for missing appointments mainly due to time constraints and issues stemming from the clinic appointment system.
Lack of Time: A recurrent theme was the patients’ struggle with time limitations, which negatively impacted their ability to attend appointments with the dietitian and become actively engaged with dietary advice. One of the female participants who had not seen the dietitian for the past 6 months said: The circumstances and obligations prevent me from visiting the nutritionist due to lack of time, and sometimes transportation. . . . (P#1, NVD)
Some participants mentioned that the dietitian is busy and unavailable due to other patients: . . .No, I mean, when the doctor says go to the dietitian, I go, but sometimes the dietitian is not there or has other patients. . . .. busy clinic. I want to finish my appointment quickly and not wait. (P#15, NVD)
Other participants mentioned the conflict between appointment timings and work commitments, suggesting that a lack of flexibility in scheduling could hinder appointment attendance: The time of appointments, people are at work and cannot take a leave. It is a little difficult to attend this appointment, that is it. (P#27, VD)
Multiple factors, such as family responsibilities and the distance from the clinic, acted as barriers to appointment attendance: Considering my daughter’s busy schedule and the distance we live from the clinic, what should I do about the appointment? (P#28, VD)
Impractical Appointment Arrangement: Participants discussed issues within the appointment system, leading to missed appointments due to a lack of information and challenges in accessing care:
One of the participants said, “They did not tell me that I had an appointment, and I did not go. Yes, when they tell me to come, I go” (P#33, VD).
Another participant said: On the days I do not attend the clinic, I have forgotten the appointment, and no one reminded me. And once I remember, I will go to them, and they will tell me it is over. This has happened to me three or four times (P#35, VD)
Barriers to Implementing Nutrition Counseling
Participants cited that various factors, including social aspects, health status, and the quality of nutrition counseling, have negatively affected their ability to implement nutrition advice.
Family, social, and cultural influences: Participants discussed social pressure during family gatherings and other social events. Moreover, they found it difficult to reconcile dietary recommendations with their cultural heritage and traditional eating habits: When someone invites you, you cannot refuse; the in-laws invite you to come to eat meat and rice. What should we do with them? (P#24, VD) The advice of the dietitian is not in line with our customs and traditions, and there is a huge difference. I will apply it for a day or two. The family and the wife encouraged me for one day to two days, but by the grace of Allah, they would relax later. There are weddings and parties on special occasions. (P#25, VD)
Health Factors: The health status of the participants, such as physical limitations and medical conditions, negatively affected the patients’ ability to follow the physical activity recommendations.
For example, 1 participant mentioned that diabetes-related nerve damage and joint pain negatively impact her ability to engage in physical activity: Nothing; I never thought that it would be difficult for me. I applied it [diabetes management], but the sport. . . I cannot do it. Even standing, I cannot stand for more than 15 minutes, and my dear nerves are tired. I do not walk a lot because my knees are tired. (P#29, VD)
She said to me now, eat only low-fat. . . This is difficult for us. She said, eat more grills, do not eat liver, do not eat the brain, do not eat the kidneys, and I do not eat this. (P#26, VD) Yes, we cannot apply these things. I eat more, I eat more, and it is not healthy. I messed up. The dietitian said to eat a lot of salads, eat less, eat bread, and we cannot live without rice, so we eat a little of everything. (P#40, VD) I mean, it is not difficult, but it gives you things that are not enough. . . We are used to eating extra and feasting on food. (P#30, VD)
Theme 2: Diabetes Self-Management Practices
Participants reported using various strategies to manage their diabetes. Being physically active and following their meal plans were 2 of the main strategies in diabetes self-management.
One of the participants who had not visited a dietitian in the past 6 months commented on how, in the old times, people were very active: Even without diabetes, you have to walk and move, but if you eat and sit around, that will not work. But the nonsense that we eat and wait for someone to give us food or coffee is wrong. And the dinner at a late time is wrong. It is a disaster that we created. Why did we have dinner right after the maghrib [sunset] during the early 1990s? We used to eat dinner very early, and after an hour, we walked together with the neighborhood’s people. Now everyone complains about stomach problems, even the young ones, they eat hamburgers and junk food and get diseases. Twenty-year-olds now have high cholesterol. We have to stick to our old ways, our old lifestyle. I see my blood results are excellent. (P#17, NVD)
Some participants cited being physically active and following their meal plans: The issue with dinner is that I do not have dinner. I follow our customs and traditions, but I focus on vegetables and simple things. For breakfast, my breakfast is special, such as dinner with vegetables and simple things. I mean, lunch, by God, I eat with family from the shared common plate, but I eat a little bit of rice and more chicken and vegetables. Thank God. I used to walk. I can walk up to five kilos, seven kilos, and eight kilos, and I turned around and came back, but during the cold weather, it is not regular. (P#25, VD)
Other participants mentioned that they adopted alternative medicine to manage their diabetes: For a while, I used to walk. Then I read about these recipes, put them in the “Dallah” (kettle), and add cinnamon and dried limes that lower the sugar. I have had it now for more than two months; I drink it daily. Today is my appointment to see if there is a change in my blood sugar level. (P#10, NVD)
Theme 3: High to Moderate Self-Efficacy
Participants exhibited a range of confidence from high to moderate in managing their diabetes based on their statements during the interviews. While some participants indicated a strong belief in their ability to manage their condition, others needed reminders and additional information from their healthcare providers: I find myself able to manage diabetes. I have enough confidence because I am aware of the nature of diabetes, and I receive regular feedback from my doctors. (P#2, NVD) I give myself 6 or 7 out of 10 occasionally; you need to be reminded and given information. (P#12, NVD)
While some people possess the ability to manage their diabetes, they feel that the diabetes management meal plan affects their psychological and emotional aspects, which impact their confidence and mood. The following quote is from a participant who had diabetes for 9 years: I am able to, but with difficulty. It is not easy because you follow a restricted diet. Restriction is always hard. It is not easy, even if there is something good. I mean, you are restricted to a specific diet plan. Honestly, it is not easy, and it presents a challenge. Especially since I lost weight from 94 to 64 kilos. There was an effort that affected you psychologically. Mood can be slightly affected when you are following a diet. If you are on a diet, you might feel a little nervous, it affects you psychologically. (P#36, VD)
Theme 4: Low Self-Efficacy
Some participants showed a disconnect between the nutrition advice they received for diabetes management and their commitment to applying it. One participant who had diabetes for 10 years stated: In terms of commitment to it, yes, in terms of application, no. (P#35, VD)
External factors, such as work-related stress, seemed to impact the confidence and ability to manage diabetes negatively. The statement below is from a patient who was referred to the dietitian, but she did not attend the visit: I want to [take care of my diabetes], but now I think psychologically I am not able to for a while. The pressure of work. Without going to the nutritionist, I could drop 25 kilos due to determination, but that was when I was comfortable, before I started working. (P#10, NVD)
External factors, such as social gatherings, seemed to affect the individual’s confidence in managing their diabetes: No, I can, but I do not have to. I mean, our circumstances and our gatherings do not allow you to do anything like this. (P#34, VD)
Theme 5: Participant Suggestions
Participant suggestions focused on improving: (1) the appointment system, and (2) the quality of nutrition counseling.
Improve the Appointment System: Participants provided valuable insights into the importance of a strong appointment system to enhance patient retention and attendance at dietitian appointments. One of the suggestions mentioned by multiple participants in facilitating the dietitian visits was related to scheduling the dietitian’s appointment on the same day as the doctor’s appointment: Umm, if my doctor’s appointment were with my dietitian’s appointment, I would be motivated. I am busy. Sometimes, I visit my farm, and sometimes I travel. I barely have time to go to my doctor’s appointment. Sometimes, I am busy, yes. It is good if the doctor’s appointment is with the dietitian’s appointment. You come for your appointments for one day and then leave. (P#7, NVD) To make her appointment on the same day as a doctor’s appointment, and during the waiting time for the doctor, we use it to meet the dietitian and talk. (P#5, NVD) Improve the Quality of Nutrition Counseling
Participants made several suggestions for improving nutrition counseling for patients with diabetes. These suggestions were related to various aspects of patient care, education, and communication aimed at enhancing service quality and patient retention.
Provide Practical Strategies: Patients highlight the need for specific practical strategies such as portion control or a structured meal plan for patients to implement dietary changes in daily life. One participant made the following statement: The dietitian told me to reduce the rice, to reduce a little. Give me a regular schedule, a meal plan for diabetes. (P#20, NVD)
Link the Counseling to the Health Goals: Patients suggested that dietitians need to convey the importance of dietary changes to the health goals of the patient: If the patient feels that he needs a nutritionist, the nutritionist must, in return, give him something that suits him. I mean, how does the nutritionist attract me? I must feel that what she [dietitian] talks about is relevant for me. (P#9, NVD)
Focus on Personalized Guidance: Participants suggested regular follow-up appointments with dietitians for continuous personalized guidance and support, considering the changing needs of individuals with diabetes: . . . to be aware of my current situation, to be updated on the information they provide at every appointment, and to review the patient’s body fat, weight, and review with the patient the meal plan. (P#2, NDV)
Provide Support Remotely: Participants highlighted the importance of maintaining patient engagement through regular check-ins and support between clinic appointments: They used to call and follow up with me, and frankly, that was good. Let them do this, and also send us reminders for our appointments. In the phone calls, they ask questions, and you answer, and they give advice, so it wasn’t difficult. But they must choose the right time, for example, in the afternoon, so that you can provide them with enough information. But during working time, you are stressed, they must choose the right time. (P#9, NDV)
Change the Educational Approach: Participants suggested holistic education to improve adherence to dietary recommendations, emphasizing the need to understand the link between nutrition, lifestyle, and effective diabetes management: They can give us tips on nutrition, especially for adult ladies who do not understand how eating, sleeping, and psychological pressure can affect sugar. . . (P#9, NVD)
Discussion
In this study, we explored the perspectives of patients with diabetes in the United Arab Emirates about their diabetes-related self-regulation and self-efficacy barriers to dietitian-led nutrition counseling. Participants discussed diabetes self-management barriers, including time constraints, appointment-related issues, health-related concerns, and social and cultural norms, which hindered adherence to diabetes management nutrition recommendations. The results also indicate varying self-efficacy levels. These factors affected patients’ abilities to adhere to dietary recommendations and attend appointments with dietitians. Participants suggested solutions to overcome these barriers. These barriers and solutions were interpreted in the context of the self-regulation and self-efficacy constructs of the social cognitive theory (SCT). Figure 1 provides a conceptual model of the barriers and solutions to dietitian-led nutrition counseling.
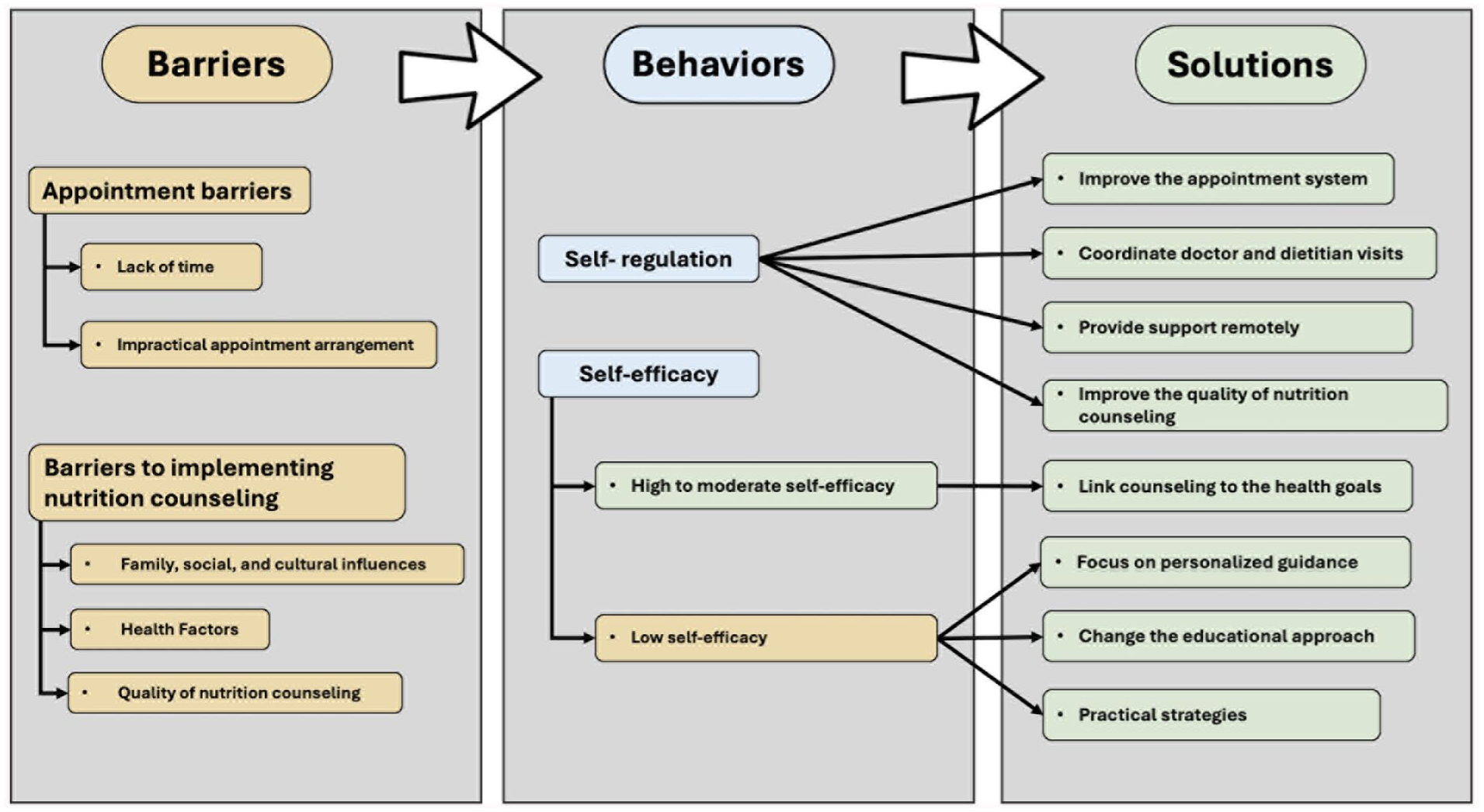
Conceptual model of barriers and solutions to dietitian-led nutrition counseling. The 5 main themes and related subthemes which emerged from the thematic analysis are interpreted in the context of the self-regulation and self-efficacy constructs of the social cognitive theory (SCT). Yellow: Barriers; Blue: Social cognitive theory related behaviors; Green: Solutions.
Social factors, such as family dynamics and cultural norms, were identified as having a negative impact on the implementation of the nutrition recommendations provided by the dietitian. The impact of socio-cultural barriers to diabetes in this study is consistent with other studies.32-34 In a study conducted with adolescents and young adults with type 1 diabetes in Qatar, 15 and another among persons with diabetes in Nepal, 35 socio-cultural issues, such as the traditional food, negatively affected the adherence to a healthy lifestyle. Previous research also found difficulties adhering to diabetes management recommendations during family and social gatherings involving food.36,37
In the Emirati context, dietitian-led nutrition counselling is challenged by deeply rooted traditional transformations and socio-cultural norms, as well as a strong food heritage. Emirati communities are close-knit and highly social, placing great value on hospitality, family relationships, and communal living. Thus, dietitians and other healthcare providers must consider these social influences during nutrition counseling sessions. Indeed, the current guidelines for the management of diabetes, in the UAE, including the ones applicable to this health care center, emphasize individualized medical nutrition therapy.38,39
Dietitians should consider family dynamics and shared decision-making within the Emirati context to minimize some of the barriers cited by the study participants in implementing nutrition recommendations. Dietary guidance must respect Emirati food practices, focusing on portion control and ingredient substitutions rather than eliminating culturally significant foods. Moreover, dietitians need to establish a collaborative counseling relationship with patients for diabetes management during Ramadan and festive occasions, which require tailored guidance that considers traditional foods commonly consumed during these periods.
Time constraints emerged as one of the main barriers to diabetes management. Participants cited busy schedules and work-related stress as barriers to attending regular appointments and engaging effectively with the health center’s dietitians. This issue is consistent with previous research highlighting the impact of time constraints 40 and work-related stress33,41 on diabetes management. Participants also reported issues with the clinic’s appointment system, including poor communication, leading to missed appointments. These findings emphasize the importance of creating a patient-centered appointment system that minimizes obstacles to accessing care. Improved communication and appointment scheduling can enhance patient engagement and healthcare outcomes. 42
Health status, particularly physical limitations and medical conditions, emerged as another influential factor. Individuals with pre-existing health issues, such as eye problems or joint pain, faced challenges in engaging in physical activity, a key component of diabetes management. This highlights the importance of personalized care plans that account for patients’ unique health constraints. 43 Moreover, the quality of nutrition counseling was an important factor in influencing patients’ willingness and ability to implement dietary changes. Patients expressed resistance when they perceived recommendations were overly restrictive or incompatible with their preferences and cultural habits. Effective communication, personalized recommendations, and understanding patients’ habits and preferences are essential for successful nutrition counseling. 7
The findings from the interviews in the present study show that psychological factors and external pressures, such as work-related stress and social gatherings, influence diabetes management and self-efficacy. A previous study found that limited diet knowledge and perceived social unacceptability of healthy behaviors hinder diabetes patients’ healthy eating and exercise. 44 On the other hand, patients’ confidence in making positive choices and following recommendations contributed to their ability to manage their diabetes effectively. According to Bandura, individuals with high self-efficacy engage in behavioral changes. 8
Participants in the study expressed various levels of self-efficacy in managing their diabetes. Participants with a high level of self-efficacy were confident in managing diabetes effectively, whereas those with a moderate level of self-efficacy reported challenges, such as experiencing negative emotions and requiring reminders to remain adherent to dietary advice. On the other hand, those categorized as “low self-efficacy” cited limited engagement in diabetes self-management behaviors due to work-related stress and social gatherings as barriers to diabetes self-management. Previous research found associations of high self-efficacy with high skill level, postgraduate education, and longer diabetes duration.33,45
These variations highlight the importance of assessing self-efficacy in influencing adherence to diabetes self-care. Moreover, the results provide insight into the role of self-efficacy in diabetes management, particularly in the context of following dietary advice and engaging in self-care practices. Previous research reported various levels of self-efficacy among patients with diabetes.46-49
The findings of this study are consistent with previous research on the role of self-efficacy and diabetes self-management, emphasizing the importance of individuals’ beliefs in their ability to control their condition and make positive informed decisions. 48 Dietitians should support patients’ self-care confidence by providing them with the necessary skills and knowledge, since knowledge and intention alone may not always lead to action. 50 Promoting a higher level of self-efficacy has been associated with improved DM self-care practices, including nutrition, exercise, and medication adherence. 51
One of the main self-regulation strategies identified by the participants in this study was exercise. This finding aligns with the literature highlighting the positive impact of regular exercise on blood glucose control and overall diabetes management.52,53 Another strategy the participants mentioned was using alternative medicine, such as recipes containing cinnamon and dried limes, which could help lower blood sugar levels. Although alternative therapies are a topic of interest in diabetes management, rigorous scientific evidence may not support their efficacy. 53 On the other hand, the combination of exercise, healthy eating, and proper sleep mentioned by some participants in the present study aligns with established guidelines for diabetes self-management, 54 emphasizing a holistic approach to managing diabetes.
The patient suggestions are crucial for improving the effectiveness of nutrition counseling and enhancing patient retention. By addressing the patients’ individual needs, offering relevant guidance, and fostering a supportive and empathetic environment, the center can contribute to improved diabetes management outcomes and a higher level of patient satisfaction. The suggestions from participants include a coordinated scheduling system that aligns with patients’ existing healthcare routines, including physician and dietitian visits, as well as sending reminders and offering remote nutrition counseling at patient-convenient times, such as in the afternoons, to improve retention and adherence to dietitian appointments.
Participants suggested that dietitians must convey the importance of dietary changes in relation to the patient’s health goal, highlighting the need for dietitians to effectively communicate how dietary adjustments directly impact the patient’s well-being.
Limitations and Strengths
The main limitation of this study is that it is based on the opinions of 44 adults (43 of whom had type 2 diabetes) attending an outpatient diabetes management clinic. This limits the generalization of the study findings to people with diabetes in the UAE. However, in line with qualitative research methodology, data saturation was achieved to guide the sample size. This study did not collect demographic information, such as educational level and employment status. Future studies should examine these demographic factors and their impact on patients’ attendance at dietitian nutrition consultations to tailor educational approaches better.
On the other hand, the study has several strengths in originality. To our knowledge, this is the only study that explored the perspectives of adults with diabetes in the Arab Gulf region, a region with one of the highest prevalences of diabetes. It provides an insight into the diabetes nutrition self-care among adults within the unique socio-cultural context of the UAE. The social cognitive theory guided the study in interpreting patients’ perspectives on the barriers to diabetes nutrition counseling within the local context. Moreover, the study provides valuable suggestions from participants to minimize barriers to attending dietitian nutrition counseling, including coordinating dietitian and doctor appointments, and providing nutrition counseling remotely.
Informed by participants’ perspectives, the interview findings can enhance diabetes self-management education and support for people with diabetes in the UAE. Further studies that explore the perspectives of people with diabetes in other diabetes education centers could provide additional insight or confirm the findings of the present study.
Implications for Practice
The results of this study can inform strategies to enhance self-regulation to support better health outcomes. Dietitians should recognize the impact of socio-cultural factors, health status, and the quality of nutrition counseling as significant challenges and collaborate with patients to overcome these barriers. Providing tailored advice and psychological support has the potential to improve self-efficacy. Moreover, aligning the patient’s doctor and dietitian appointments, sending automatic reminders for missed appointments, and offering remote nutrition counseling sessions (via telephone or video) at the patient’s convenient times could help overcome barriers to dietitian-led visits. Finally, since there was only 1 patient with type 1 diabetes, the findings from this study are mainly applicable to patients with type 2 diabetes.
Conclusions
The results of this study enhance our understanding of the barriers faced by individuals with diabetes in the UAE. These findings offer insights into the self-regulation strategies, barriers, and factors that negatively impact self-efficacy in adults with type diabetes mellitus within the socio-cultural context of the UAE. Approaches that consider individualized management strategies, counseling quality, and the socio-cultural context of the UAE are essential for enhancing patient adherence to dietitian counseling sessions.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251388306 – Supplemental material for Self-efficacy, Self-regulation, and Barriers to Dietitian-led Nutrition Counseling: Qualitative Interviews with Adults with Diabetes in the United Arab Emirates
Supplemental material, sj-docx-1-jpc-10.1177_21501319251388306 for Self-efficacy, Self-regulation, and Barriers to Dietitian-led Nutrition Counseling: Qualitative Interviews with Adults with Diabetes in the United Arab Emirates by Habiba I Ali, Amal I. Al Harbi, Maitha Alnahdi, Mahra S. Alshamsi, Mariam R. Aldhaheri, Shamma M. Al Meqbaali, Meera A. Aldahmani, Bolaji Ilesanmi-Oyelere, Ayesha S. Al Dhaheri, Leila Cheikh Ismail, Lily Stojanovska and Nishan Sudheera Kalupahana in Journal of Primary Care & Community Health
Footnotes
Ethical Considerations
The ethical approval of this study was provided by the Imperial College London Diabetes Centre Research Ethics Committee (approval #: IREC 080). All study methods were conducted in accordance with the guidelines and regulations of the Imperial College London Diabetes Centre Research Ethics Committee.
Consent to Participate
Participants were informed that their participation in the project was voluntary, and that all the information collected would remain anonymous and confidential. Prior to the data collection, all the participants provided oral and written informed consent to participate in the study and agreed to have the interview audio-recorded within the clinic premises.
Consent for Publication
Not applicable.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from Mubadala as part of the Mubadala-UAEU Collaborative Research & Development Program (grant number 21M159). The funding source had no role in the research project’s implementation, data collection, or analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All relevant data are presented within the manuscript and its supporting Supplemental Information files. Due to ethical considerations, the authors cannot make any additional interview data publicly available because they contain potentially identifiable and confidential patient information with the possibility that individuals may be recognized in the data. Additional data may be shared upon reasonable request to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.