
Abstract
Introduction:
Language development during the first 2 years is crucial for cognitive and social growth. The purpose of this study was to assess receptive language (RL) and expressive language (EL) development and associated factors in 18-month-old Thai children.
Methods:
This cross-sectional study was conducted from September 2024 to February 2025. Multistage sampling was applied to recruit 1150 participants who were parents or primary caregivers of 18-month-old children. Data were collected using structured questionnaires and the Developmental Surveillance and Promotion Manual, a standardized national tool. Binary logistic regression was used to analyze associations between child, parental, and healthcare access factors and language development.
Results:
Overall, 88.7% and 85.6% of children had age-appropriate RL and EL development, respectively. After adjusting for covariates, high parental knowledge and high parental behaviors in language development were significantly associated with both age-appropriate RL development (AOR = 2.122, 95% CI = 1.338-3.364 and AOR = 2.251, 95% CI = 1.396-3.628, respectively) and age-appropriate EL development (AOR = 2.452, 95% CI = 1.618-3.718 and AOR = 1.892, 95% CI = 1.210-2.960, respectively). Access to anemia screening services at 6 to 12 months was also significantly associated with both age-appropriate RL development (AOR = 1.700; 95% CI = 1.104-2.617) and age-appropriate EL development (AOR = 2.026; 95% CI = 1.384-2.967).
Conclusion:
Parental and healthcare access factors were significant determinants of language development. Improving parental competencies and integrating language development surveillance and preventive healthcare at primary care settings could be valuable strategies for promoting language development in early childhood.
Keywords
Introduction
Language development is a critical milestone that influences a child’s long-term cognitive, social, and academic outcomes. 1 Before children develop speech, they communicate primarily through their actions and behaviors. 2 As they grow, they begin to develop thinking operations based on concrete experiences, alongside 2 key language capabilities: receptive language (RL), which involves understanding what others say, and expressive language (EL), which involves producing speech and communicating their own thoughts.1,3 However, language delay is common in early childhood and affects communication problems later. 4
Developmental delays in language and communication are typically identifiable between 18 and 36 months of age.5,6 At this stage, children generally demonstrate distinct milestones in both RL and EL, with receptive abilities typically emerging before expressive skills. 7 A study at the Yale New Haven Hospital shown that EL delays affect approximately 13.5% in children aged 18-23 months and increase to 17.5% in children aged 30 to 36 months. 8 Although, most children with EL delays are likely to recover without intervention (60%), those with both RL and EL delays are substantially less likely to recover spontaneously (25%). 8 Therefore, early identification of speech and language delays at 18 months—considered a critical window of opportunity—is essential for indicating future language developmental trajectories and preventing socio-emotional problems.9,10
Early childhood development is commonly assessed using standardized tools. Globally, the Denver Developmental Screening Test (DDST) and its revisions are utilized to assess language milestones. 11 In Thailand, early childhood development is assessed by using the Developmental Surveillance and Promotion Manual (DSPM), a standardized national screening tool utilized by the Ministry of Public Health. 12 DSPM covers 5 developmental domains: receptive language, expressive language, gross motor, fine motor and cognitive, and self-help and social development. 13 DSPM is used by health personnel, parents, and caregivers to monitor and promote development in children from birth to 5 years and it is widely implemented in primary healthcare settings.12,13
Primary health care systems play a crucial role in promoting early language development and identifying developmental concerns. 14 In Thailand, Subdistrict Health Promoting Hospitals (SHPHs)—the community health centers—serve as the frontline primary healthcare settings. 15 Well-baby clinics provided at these facilities are well-positioned to detect early signs of language delay and to deliver timely interventions during critical periods of development. 16 At SHPHs, children undergo developmental screening by health personnel during scheduled immunization visits at 9, 18, 30, 42 and 60 months. 16
Integrated efforts within Thailand’s primary healthcare system aim to strengthen age-appropriate language development among young children. 16 A prior study estimated that 86.5% of Thai children aged 18 to 30 months demonstrated age-appropriate development. 17 Another study reported that 85.7% of children aged 36 to 62 months met expected developmental milestones. 18 However, another study found that only 59.1% of children aged 24 to 60 months showed age-appropriate development. 19
According to the literature, the determinants of child language development comprise a range of interrelated factors, including child-related characteristics (eg, birth order, 20 history of perinatal asphyxia, 21 and breastfeeding history 21 ), parental-related characteristics (eg, average monthly household income,22,23 and parental knowledge,24 -26 attitudes,27,28 and behaviors24,25,29 regarding language development), and healthcare access factors (eg, access to anemia screening services,30,31 utilization of DSPM,16,19,32 and access to language development services33 -35). These determinants align with Bronfenbrenner’s bioecological model, which emphasizes proximal processes—the dynamic interactions between individual and environmental factors in child development.36,37 In this framework, child-related characteristics represent individual factors, while parental-related characteristics and healthcare access factors constitute environmental influences on child language development.
Despite national screening tools and integrated developmental services in Thailand's primary healthcare system, a substantial proportion of children still experience language development delays. Additionally, there is limited evidence on how multiple interrelated determinants collectively influence age-appropriate language development among Thai children at 18 months of age. These determinants include child, parental, and healthcare access factors. Therefore, this study aims to examine RL and EL development and associated factors in 18-month-old Thai children using Bronfenbrenner’s bioecological framework. The findings are expected to help healthcare providers design early interventions for language development within primary healthcare settings. These insights may also inform policymakers in formulating strategies for enhancing early childhood development programs nationwide.
Materials and Methods
Study Design and Participants
This cross-sectional study was conducted in accordance with the Supplemental STROBE guidelines. 38 In Thailand, the Ministry of Public Health has divided the 76 provinces and 1 special administrative area (the capital, Bangkok) into 13 health service regional networks, called “Health Region.” Health Region 2 is in the lower northern part of Thailand. In 2024, this region reported the highest proportion of normal child development (86.6%) compared to other Health Regions, exceeding the national key performance indicator of 86.0%. 39 This suggests that Health Region 2 may serve as an effective area for learning from success in child development promotion and was therefore selected as the study setting.
The study population were parents or primary caregivers of 18-month-old children residing in Health Region 2, which comprises 5 provinces: Phitsanulok, Sukhothai, Tak, Phetchabun, and Uttaradit. Thus, the total number of this study population was 20 026. 39
The sample size was estimated using G*Power version 3.1.9.7, 40 applying the formula for logistic regression analysis. The calculation was based on a previous study in Thailand, 41 which identified primary caregiver as a predictor of language development in 41.0% of children aged 2 to 5 years, with an odds ratio of 0.64. Therefore, the following parameter values were used for the sample size estimation: Pr(Y = 1 | X = 1) = 0.41, OR = 0.64, α = .05, power (1 − β) = .90, R² for other predictors = .10, X distribution = binomial with X parameter π = .50. 42 Consequently, the minimum sample size was 1030 participants. To account for potential non-response and data loss, the sample size increased by 15%, resulting in a final required sample size of 1185 participants. Ultimately, 1150 completed questionnaires met the eligibility criteria and were included in the analysis, corresponding to a response rate of 97.0%.
A multistage sampling cross-sectional study 43 was employed to ensure a representative and contextually diverse sample within Thailand’s Health Region 2. In the first stage, simple random sampling via a lottery method was used to select 3 provinces from the 5 eligible provinces in the region. In the second stage, since each selected province comprises 9 districts, 4 districts per province were selected using the same lottery method. In the third stage, proportional to size calculation was used to allocate the number of participants to be recruited in each district. The allocation was based on the number of parents with 18-month-old children scheduled for developmental assessments, as recorded by each district’s health office. In the final stage, A sampling frame was constructed using the appointment lists of 18-month-old children scheduled for developmental assessments at the well-baby clinics in SHPHs. From this list, simple random sampling was conducted to select parent-child pairs in each district. Data collection continued until the pre-allocated target number of participants (as determined in Stage 3) was reached in each district. These probability sampling methods minimized selection bias and ensured that all eligible individuals had an equal probability of selection. 43
The inclusion criteria were as follows: participants had to be parents or primary caregivers who had been the main caretaker of an 18-month-old child for at least 6 months, were aged between 20 and 65 years, and were able to read, write, and communicate fluently in Thai. In addition, participants had to be willing and able to provide informed consent and complete the questionnaire. The exclusion criteria included being the caregiver of a child with visual or hearing impairments or of a child diagnosed with genetic disorders or developmental conditions that may affect language development, such as Down syndrome, cerebral palsy, or autism spectrum disorder.
Measurements
The research instruments and their measurements are presented as follows:
Child-related characteristic factors were assessed using 3 dichotomous items: birth order (first-born vs later-born), history of perinatal asphyxia based on the APGAR score (abnormal vs normal), and breastfeeding history (ever vs never). These variables were obtained from the Mother and Child Health Handbook, 44 which is kept by the child’s primary caregiver and brought at each healthcare visit—particularly during scheduled growth developmental assessments and immunization appointments. The handbook is provided to mothers during their first antenatal care and serves as both a medical record and educational guide on pregnancy care, childbirth, child growth and development, immunizations, and health promotion activities up to the age of 12 years.
Parental-related characteristic factors were measured as follows:
Two dichotomous items assessed the primary caregiver (biological parents vs others, eg, relatives or guardians) and average monthly household income (<15 000 vs ≥15 001 Thai Baht), categorized based on the income threshold of previous study. 45
Parental knowledge of language development was measured using 20 dichotomous items. The score range was 0 to 20. Scores were categorized using a cut-point at the 80th percentile,24,46 with scores of 0 to 15 indicating low to moderate knowledge, and 16 to 20 indicating high knowledge.
Parental attitudes toward language development were assessed using 20 items on a 5-point Likert scale. The score range was 20 to 100. Scores were categorized as low to moderate (20-83 points) or high (84-100 points), based on the 80th percentile cut-point.24,46
Parental behaviors to promote language development were assessed using 21 items on a 5-point Likert scale. The score range was 21 to 105. Scores were classified as low to moderate (21-87 points) or high (88-105 points), using the 80th percentile cut-point.24,46
Healthcare access factors were measured as follows:
Three dichotomous items assessed access to key child health services: (1) anemia screening at age 6 to 12 months (received vs did not receive), (2) iron supplementation syrup at age 6 to 12 months (received vs did not receive), and (3) access to and use of the DSPM 12 (used vs did not use).
Access to language development services was measured using 10 items on a 5-point Likert scale. The score range was 10 to 50. Scores were categorized as low to moderate (10-41 points) or high (42-50 points), based on the 80th percentile cut-point.24,46
Language development, the dependent variable in this study, was assessed using the DSPM encompassing both RL and EL. 12 This national standardized tool is validated for developmental assessments at specific age milestones (9, 18, 30, 42, and 60 months). For this study, we focused on the 18-month milestone, as DSPM is specifically designed and validated for each age point. Children were evaluated at 18 months chronological age, in accordance with the Thai national developmental surveillance system protocol, which calculates age from birth regardless of gestational age. In practice, this means that preterm children are also evaluated using their chronological age during routine well-child visits. The DSPM demonstrated a sensitivity of 96.04% and a specificity of 64.67%. 13 Its reliability, as indicated by Cronbach’s alpha coefficient, was .81. 13 DSPM assessment was based on parent or caregiver reporting and direct observation by trained health professionals. Children were categorized as either having age-appropriate development or a suspected delay, depending on whether they met the expected developmental milestones for their age. In the logistic regression model, the outcome was coded as 1 = age-appropriate development and 0 = suspected delay, so that an odds ratio (OR) greater than 1 indicates a factor associated with a greater likelihood of age-appropriate language development.
Validity and Reliability of the Research Instrument
The content validity index (CVI) 47 of the questionnaire was evaluated by 5 experts, including 2 university-based experts in research instrument development, 1 developmental-behavioral pediatrician, and 2 public health professionals in promoting language development in childhood. The item-level CVI (I-CVI) values ranged from 0.80 to 1.00. The scale-level CVI based on universal agreement (S-CVI/UA) values for the parental knowledge of language development, parental attitudes toward language development, parental behaviors to promote language development, and access to language development services questionnaires were 0.80, 0.95, 0.85, and 0.80, respectively. The scale-level CVI based on average method (S-CVI/Ave) for the same 4 sections were 0.96, 0.99, 0.97, and 0.96, respectively. I-CVI values ≥0.78, S-CVI/UA values ≥0.80, and S-CVI/Ave values ≥0.90 indicate that the research instrument meets the criteria for acceptable content validity. 47
After revision based on expert feedback, a pilot test was conducted with 30 participants who shared similar characteristics with the target population. The reliability of the parental knowledge of language development questionnaire, assessed using the Kuder-Richardson Formula 20 (KR-20), 48 was 0.78. The reliability of the parental attitudes toward language development, parental behaviors to promote language development, and access to language development services questionnaires, assessed using Cronbach’s alpha coefficient, 49 were .91, .84, and .96, respectively. Both KR-20 and Cronbach’s alpha coefficient were higher than the acceptable value of .70. 50
Data Collection
Data collection was conducted between September 2024 and February 2025 across selected districts in Thailand’s Health Region 2. In each district, a team of 3 research assistants was assigned to assist with data collection under the supervision of the principal research team. Prior to fieldwork, all research assistants received training on the study objectives, protocols for obtaining informed consent, and standardized procedures for administering the research instruments.
Eligible parents or primary caregivers of 18-month-old children were approached at the well-baby clinics in SHPHs on scheduled developmental assessment days. After participants provided the written informed consent, they completed a structured, self-administered questionnaire in Thai. Each session lasted approximately 30 to 45 min. Completed questionnaires were forwarded to the central research team for data entry and analysis. Despite on-site checks by research assistants prior to submission, 35 out of the 1185 estimated questionnaires were found to be incomplete and excluded from the final analysis. Therefore, a total of 1150 questionnaires from participants were considered eligible for data analysis, yielding a response rate of 97.0%.
Data Analysis
Data were analyzed using SPSS Statistics for Windows, version 17.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics, including frequencies, percentages, means (x–), standard deviations (SD), and minimum (Min) and maximum (Max), were employed to summarize the participants’ characteristics. For inferential analysis, bivariate logistic regression with a 95% confidence level was performed to examine the associations between independent and dependent variables. If variables had a P-value less than .25, they were then included in multivariate logistic regression using the enter method. 51 The Hosmer-Lemeshow goodness-of-fit test was utilized to test model fit, with a P-value greater than .05 indicating good fit. 52 Adjusted odds ratio (AOR), 95% confidence interval (CI), and P-values less than .05 were used to identify statistically significant associations.
Results
Participant Characteristics
Of the 1150 participants (Table 1), 48.3% of the children were first-born. Based on APGAR score records, only 0.7% had a history of perinatal asphyxia. Regarding infant feeding practices, 90.6% had been breastfed. In terms of caregiving, 61.0% of children were cared for primarily by their biological parents. Participants with income data, 67.7% reported a monthly household income of less than 15 000 Thai Baht.
Characteristics of Participants (n = 1150).
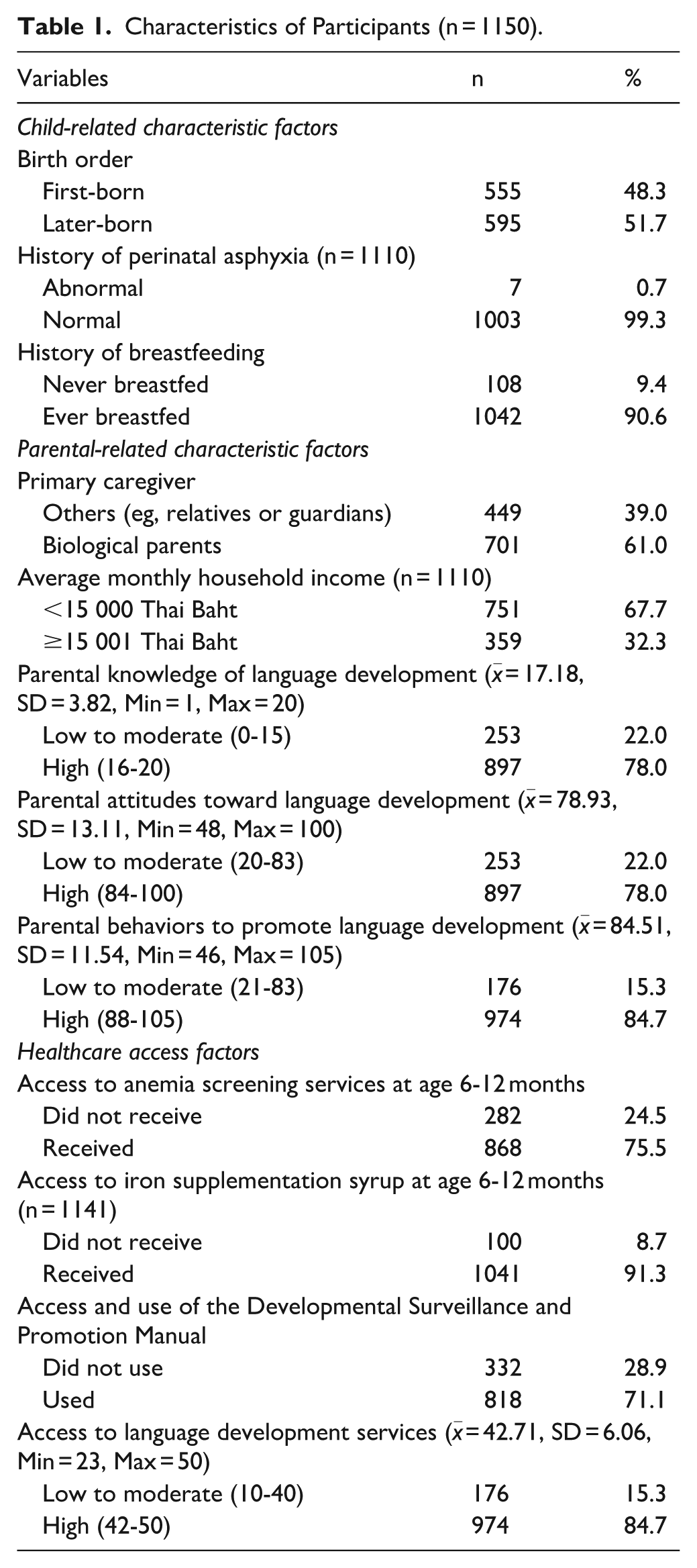
Parental knowledge of language development had a mean score of 17.18 (SD = 3.82), with 78.0% classified as having high knowledge. Attitudes toward language development had a mean score of 78.93 (SD = 13.11), with 78.0% scoring in the high category. Parental behaviors to promote language development had a mean score of 84.51 (SD = 11.54), with 84.7% categorized as high (Table 1).
Regarding healthcare access (Table 1), 75.5% of children had received anemia screening services at 6 to 12 months of age, and 91.3% had received iron supplementation syrup. Use of DSPM was reported by 71.1% of caregivers. Finally, access to language development services had a mean score of 42.71 (SD = 6.06), with 84.7% classified as high access and 15.3% as low to moderate access.
Receptive and Expressive Language Development
Among the 1150 participants as displayed in Figure 1, 11.3% (n = 130) were found to have a suspected delay in receptive language (RL) development, while 88.7% (n = 1020) demonstrated age-appropriate development. In terms of expressive language (EL), 14.4% (n = 166) showed a suspected delay, whereas 85.6% (n = 984) exhibited age-appropriate development.
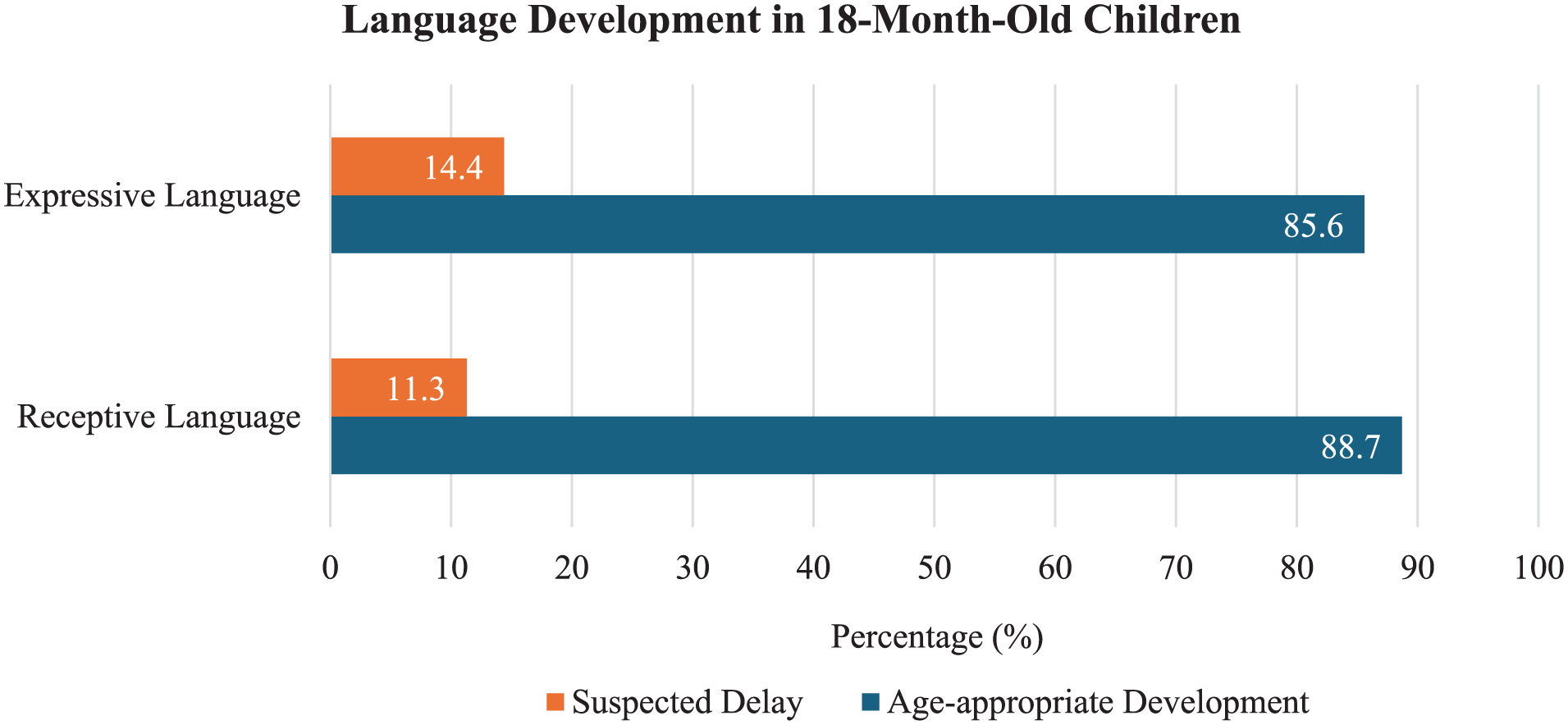
Language development in 18-month-old children (n = 1150).
Factors Associated With Receptive Language Development
Simple logistic regression analysis (Table 2) identified 8 factors significantly associated with RL development. Children who had ever been breastfed were more likely to show appropriate RL development than those who had never been breastfed (OR = 2.212, 95% CI = 1.330-3.680). High monthly household income (OR = 1.967, 95% CI = 1.253-3.089), higher parental knowledge (OR = 3.283, 95% CI = 2.245-4.799), positive parental attitudes (OR = 1.906, 95% CI = 1.283-2.832), and high supportive parental behaviors (OR = 4.079, 95% CI = 2.230-6.095) were all significantly associated with better RL outcomes. Regarding healthcare access, children who received anemia screening services (OR = 1.681, 95% CI = 1.137-2.486), used the DSPM (OR = 1.636, 95% CI = 1.120-2.389), and had high access to language development services (OR = 2.640, 95% CI = 1.737-4.011) were more likely to have age-appropriate RL development.
Binary Logistic Regression Analysis for Exploring Factors Associated With Age-appropriate Receptive Language Development (n = 1150).

p < .05.
After adjusting for potential confounders (Table 2), 3 factors remained significantly associated with RL development. High parental knowledge of language development (AOR = 2.122, 95% CI = 1.338-3.364), high supportive parental behaviors (AOR = 2.251, 95% CI = 1.396-3.628), and access to anemia screening services (AOR = 1.700, 95% CI = 1.104-2.617) were associated with appropriate RL development. The model demonstrated a good fit, as indicated by the Hosmer-Lemeshow goodness-of-fit test (χ² = 9.612, P = .293).
Factors Associated With Expressive Language Development
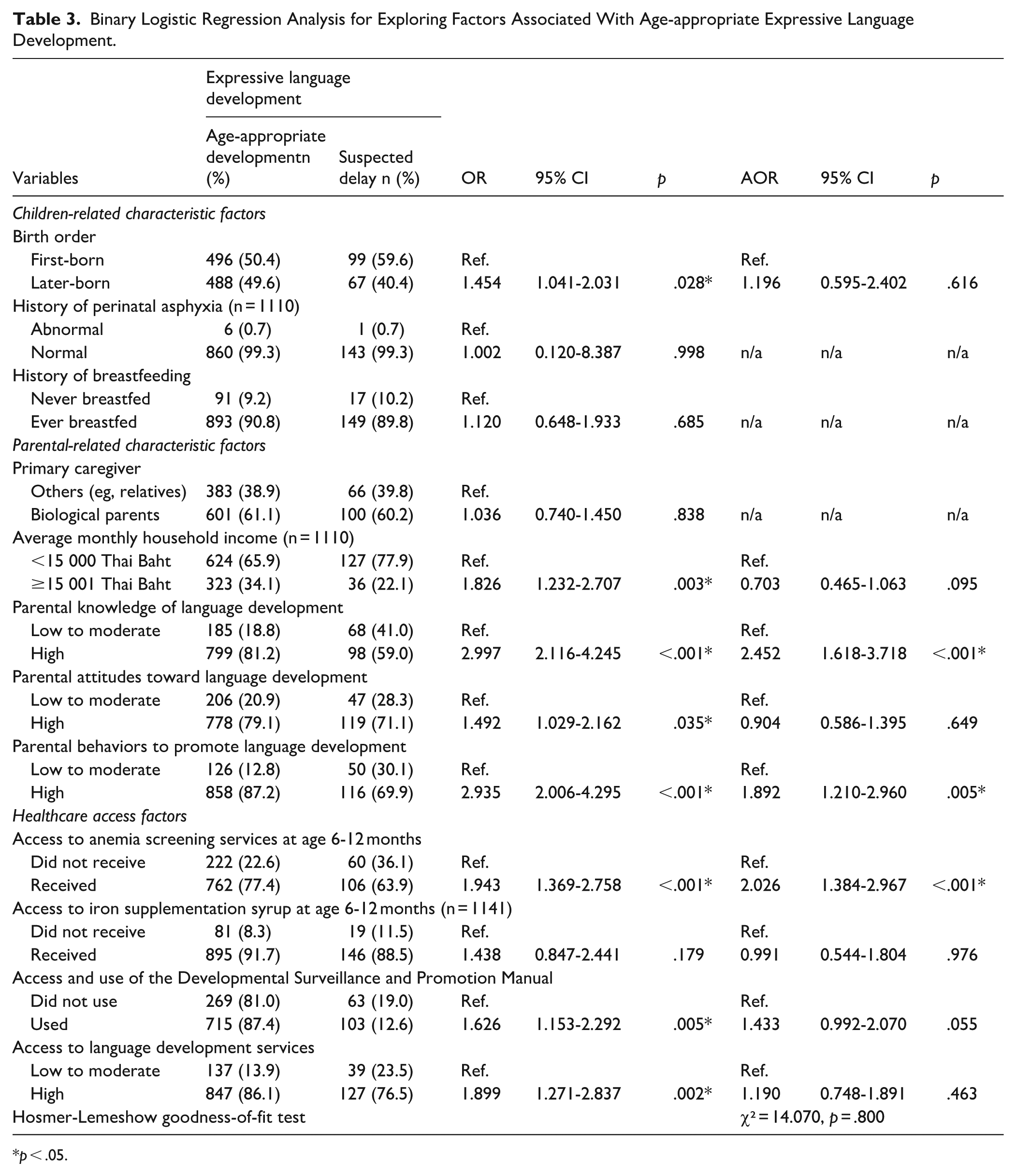
Simple logistic regression analysis (Table 3) identified 8 factors significantly associated with EL development. Later-born children were more likely to show appropriate EL development compared to first-borns (OR = 1.454, 95% CI = 1.041-2.031). High monthly household income (OR = 1.826, 95% CI = 1.232-2.707), higher parental knowledge (OR = 2.997, 95% CI = 2.116-4.245), positive attitudes of parents (OR = 1.492, 95% CI = 1.029-2.162), and high supportive parental behaviors related to language development (OR = 2.935, 95% CI = 2.006-4.295) were all significantly associated with better EL outcomes. Among healthcare access variables, children who had access to anemia screening services (OR = 1.943, 95% CI = 1.369-2.758,), access to and use of the DSPM (OR = 1.626, 95% CI = 1.153-2.292), and high access to language development services (OR = 1.899, 95% CI = 1.271-2.837) were also more likely to have age-appropriate EL development.
Binary Logistic Regression Analysis for Exploring Factors Associated With Age-appropriate Expressive Language Development.
p < .05.
After adjusting for potential confounders (Table 3), the multiple logistic regression model revealed that only 3 factors were significantly associated with EL development. High parental knowledge of language development (AOR = 2.452, 95% CI = 1.618-3.718) and high supportive parental behaviors (AOR = 1.892, 95% CI = 1.210-2.960) remained a strong predictors. Access to anemia screening services was also significantly associated with EL development (AOR = 2.026, 95% CI = 1.384-2.967). The model demonstrated a good fit, as indicated by the Hosmer-Lemeshow goodness-of-fit test (χ² = 14.070, P = .800).
Discussions
Most 18-month-old children in this study demonstrated age-appropriate language development, with 88.7% and 85.6% achieving typical milestones in RL and EL, respectively. This finding is in line with the previous study, whereby about 86.5% of Thai children between 18 and 30 months attained anticipated developmental achievements. 17 Despite that, RL development in this study exceeded the national goal of ≥86%, the rate of EL development fell somewhat short of this goal. 39 This finding reflects a common developmental pattern where EL typically emerges later than RL. 7 To address this deficiency in EL, caregiver-oriented interventions are highly recommended. For instance, a meta-analysis emphasized that parent-implemented interventions in languages brought about favorable impacts in terms of EL skills. 53 More recent systematic reviews also shown that interventions such as shared book reading, dialogic reading, and daily verbal routines were associated expanded expressive vocabulary.23,54 Results from those meta-analysis studies23,53,54 highlighted the need to incorporate such interventions in routine practice in early childhood care. In the Thai context, this might be made possible through incorporation with prevailing DSPM screening services offered in conjunction with well-child visits in SHPHs, where the national child development screening already occurs in the primary health-care setting.12,16
The present study identified determinants of RL and EL development in Thai 18-month-old children based on Bronfenbrenner’s bioecological theory that emphasizes individual and environmental system interactions in dynamical terms.36,37 The findings indicated that the parental and health-care access factors are substantial determinants of RL and EL development. Within Bronfenbrenner’s bioecological model, the parental and healthcare access factors operate as proximal processes through which environmental influences exert their effects on child development. 37
The simple regression analysis suggested that children from higher-income households were more likely to demonstrate age-appropriate language development. This result is consistent with previous studies illustrating the impact of socioeconomic status on early developmental outcomes.22,23 Higher income might assist in offering exposure to better learning environments, greater caregiver responsiveness, and healthier nutrition, all of which are important for language development.55,56 Interestingly, when we controlled for other variables in the multiple regression analysis, household income was no longer statistically significant. This may imply that household income influences language development through more proximal factors such as parenting knowledge and behaviors and access to healthcare.
Our study pointed out that parent knowledge and behaviors in language development were significant determinants of both RL and EL outcomes. Parents with high knowledge were more likely to engage in appropriate ways to stimulate language development—such as frequent verbal interactions, shared book reading, and encouraging children’s speech. These results are in line with previous studies indicating that parents with more advanced developmental knowledge are more likely to supply more supportive input to facilitate children’s vocabulary acquisition.24 -26 Similarly, high levels of parental behaviors to promote language—such as giving simple instructions for RL or encouraging vocalizations for EL 57 —were significantly associated with better language outcomes in this study. This finding supports previous studies that demonstrates the important role of parents’ responsiveness and linguistic stimulation to develop early proficiency in language.24,25,29 Although parental attitudes showed initial associations, they did not remain significant after covariate adjustment, suggesting that attitudes alone may not suffice unless they are translated into concrete supportive behaviors. 27 Therefore, interventions that aim to strengthen caregiver knowledge and to prompt active practice of language-stimulating behaviors may be vital to assist in maximizing early language development.
This study found that healthcare access factors, especially access to anemia screening services, DSPM utilization, and language development services, were associated with both RL and EL development. Among these, access to anemia screening services at 6 to 12 months remained significant in the final model after adjusting for confounders. These findings are consistent with previous studies demonstrating that iron deficiency during childhood can negatively impact language development.30,31 Furthermore, families that were able to access anemia screening services may have greater opportunities to receive developmental monitoring, caregiver education, and consistent follow-up care for their children.
In this study, families utilizing the DSPM generally achieved better language development outcomes. Although the adjusted model showed no significant association between DSPM use and language development outcome, the finding still underscores the DSPM’s utilization in Thailand’s national child health strategy. These findings demonstrate the effectiveness of community-level developmental monitoring approaches in supporting early identification and timely intervention.16,19,32 The developmental screening system enables immediate intervention when developmental delays are detected. 58 Early language screening can provide timely intervention for preventing the language impairments. 30
Additionally, results from this study showed that children with higher access to language development services at primary health care setting were more likely to achieve age-appropriate language development. This finding is consistent with prior studies demonstrating that early intervention programs delivered through health services can positively influence language outcomes.33 -35 Therefore, strengthening equitable access to preventive services and developmental interventions through primary healthcare systems is critical for enhancing language development in early childhood.
Strengths and Limitations
This study has several strengths. First, this study applied a multistage sampling cross-sectional study with a population-based sample of 1150 participants. This design enhanced representativeness and allowed the capture of both contextual and regional variation. Second, this study employed a comprehensive set of validated instruments to measure knowledge, attitudes, behaviors, and service coverage, contributing to a comprehensive understanding of language development determinants. Third, the application of both crude and adjusted regression models increases the validity of the results. Despite these strengths, limitations should be acknowledged in this study. First, due to its cross-sectional design, causality between factors that are involved and the outcome in language development cannot be established. Future research employing perspective longitudinal study would be crucial to understand the causal pathways and the temporal sequence of the determinants on language development trajectories. Second, some variables—such as health-care access and parental behaviors—were based on self-report assessment tools that are subject to recall bias and social desirability bias. These biases may have led caregivers to overreport positive health service utilization and favorable parenting practices, potentially leading to overestimation of the observed associations between these variables and child language outcomes. Third, important socioeconomic characteristics of caregivers, such as educational level, were not collected in this study. Including such variables in future study would provide a more complete understanding of factors influencing child language development. Fourth, in line with the Thai national protocol, children were assessed at 18 months chronological age from birth, regardless of gestational age. While this reflects routine practice in Thailand, it may differ from protocols used in other studies that adjust for prematurity, and this should be considered when comparing findings across different contexts. Finally, while we employed the rigorous sampling methods to ensure a representative sample, the study was conducted in 1 Thai health region, which may limit generalizability to areas with different sociodemographic or healthcare settings.
Conclusion
This study found that most 18-month-old children demonstrated age-appropriate development for RL (88.7%) and EL (85.6%). Important factors positively associated with language development included high parental knowledge and positive caregiving behaviors, as well as access to anemia screening services. These findings emphasize that both family-level and health system factors play important roles in early childhood language development. Improving parental competencies and integrating developmental monitoring and preventive health services, especially within the primary care system, could be valuable strategies for promoting language development in early childhood.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251386692 – Supplemental material for Determinants of Language Development in 18-Month-Old Children within Primary Healthcare Settings
Supplemental material, sj-docx-1-jpc-10.1177_21501319251386692 for Determinants of Language Development in 18-Month-Old Children within Primary Healthcare Settings by Piyaphan Trakultip, Artittaya Wangwonsin and Wutthichai Jariya in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors would like to thank the local health personnel and research assistants in Health Region 2 for their support in data collection. We also extend our gratitude to all participants for generously contributing their time and effort. Without their active involvement, this study would not have been possible.
Ethical Considerations
This study was reviewed and approved by the Human Research Ethics Committee of Naresuan University, Thailand (COA No. 220/2024; IRB No. P2-0253/2567; Date: July 8, 2024).
Consent to Participate
This study was conducted in accordance with ethical standards. Written informed consent was obtained from all participants prior to data collection. The data collection process adhered to the relevant rules and regulations stipulated in Declaration of Helsinki.
Consent for Publication
Not applicable.
Author Contributions
WJ and AW conceptualized the research aims and design. PT, AW, and WJ developed research methodology and instruments. PT collected data. PT, AW, and WJ contributed to data analysis and interpretation. PT drafted the initial manuscript, and WJ revised, visualized, and finalized the manuscript. All authors read and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.