
Abstract
Background:
In Canadian healthcare, systemic racism subverts commitment to universal coverage by building inequities into the system of governance, regulation, and clinical practice. Although racial disparities have been documented, little attention has been paid to how institutional structures perpetuate these inequities.
Objective:
This study critically examines the organizational aspects of racism in the Canadian healthcare system. It aims to identify structural obstacles faced by racialized patients and foreign-trained physicians and to provide policy recommendations grounded in evidence.
Methods:
The authors employed a narrative review framework for qualitative analysis of documents. Public inquiries (eg, Truth and Reconciliation Commission and Viens Report), government audits (eg, PHAC and CHRC), case files (eg, Brian Sinclair, Joyce Echaquan, and Dr. Akinbiyi), and peer-reviewed publications between 2000 and 2024 were the data sources. Thematic coding occurs across 4 areas: (1) institutional discrimination, (2) licensing and workforce exclusion, (3) patient and cultural safety, and (4) accountability gaps.
Results:
The review found continuing institutional disregard for Indigenous and Black patients, and the disparities were most marked in emergency and maternal services. Internationally educated doctors face opaque and delayed credentialing procedures, which can exacerbate workforce disparities. Case examples illustrate how system failures, including disregarding patient suffering, ignoring cultural requirements, and inadequate oversight, can lead to harm. It is a recurring pattern in which the recommended action is not taken following a review, suggesting organizational resistance to change.
Discussion:
Canadian systemic racism in health care occurs through omissions (failure to act on reform) and commissions (institutional exclusion). To tackle this, it is necessary to entrench antiracism in legislation, make cultural safety training a requirement, collect race-disaggregated data, and transform licensing routes.
Conclusion:
Universal healthcare is not equitable unless systemic racism is eliminated. Systemic changes that recalibrate healthcare governance in accordance with antiracism and equity values are necessary to provide safe and inclusive care.
Plain-Language Summary
Racism in healthcare is not only about individual attitudes; it is also built into the way the system operates. Despite major reports calling out these problems, such as those from the Truth and Reconciliation Commission and In Plain Sight, little has changed. Indigenous, Black, and racialized people still face poor treatment and outcomes. Qualified immigrant doctors and nurses face unfair barriers to work. Other countries, such as the UK and New Zealand, have taken steps to address these issues by collecting race-based data and holding healthcare systems accountable. Canada has not. Without real rules to ensure that changes occur, things remain the same. If Canada wants healthcare to be truly fair to everyone, we need laws, better data, antiracism training, and stronger oversight, not just words. This study showed that the time taken for an action is now.
Keywords
Introduction
Systemic racism in health care has emerged as one of Canada’s most pressing public health and policy challenges. Although disparities in health outcomes between indigenous and racialized populations have been documented for decades, recent high-profile cases, such as the deaths of Brian Sinclair in 2008 and Joyce Echaquan in 2020, have revealed how racial bias and institutional neglect can lead to preventable harm. These tragedies, alongside a series of federal and provincial inquiries, clarify that inequities in access, treatment, and outcomes are not isolated incidents but manifestations of deeper structural issues within Canadian health systems.
Despite being lauded for its universal coverage, Canada’s health care system often fails to deliver equitable care. Research has consistently shown that indigenous people, Black Canadians, and internationally trained physicians face systemic exclusion from professional opportunities. This disconnection between policy ideals and lived experiences highlights the limitations of universality when equity is not explicitly integrated into governance, regulation, and practice.
Although public and institutional awareness of systemic racism has increased, critical deficiencies persist in how the issue is measured empirically and resolved. Early reports, such as the Truth and Reconciliation Commission’s Calls to Action and In Plain Sight, recorded systemic racism in indigenous healthcare provisions.1,2 In recent years, the Canadian Human Rights Commission and the Public Health Agency of Canada have reaffirmed the presence of persistent disparities and accountability shortcomings in all health institutions.3,4
Most existing literature consists of descriptive reports, advocacy pieces, or isolated case studies. What is lacking is an integrated, policy-oriented analysis that draws together findings from diverse sources, including public inquiries, academic research, legal proceedings, and government audits to reveal the structure and sustainability of systemic racism.
This study addresses this need by conducting a qualitative examination of publicly accessible evidence. By employing thematic coding and embedded case studies, we discerned patterns of discrimination and exclusion based on race in 4 central areas: (1) patient safety and outcomes of care, (2) provider experience and workforce integration, (3) credentialing and professional regulation, and (4) institutionally based accountability and policy response. Brian Sinclair, Joyce Echaquan, and Dr. Amos Akinbiyi provided context-based grounding for the analysis.
The contributions of this study are twofold: it provides a structured synthesis that brings empirical evidence to bear on a larger healthcare governance framework. It also positions systemic racism not simply as an issue of interpersonal bias but of policy and structural concern that necessitates legislative, regulatory, and organizational change. In pursuing this approach, this study aims to inform accountable and equity-motivated interventions.
Method
Study Design
This study employed a qualitative document analysis with embedded case studies to examine systemic racism in the Canadian healthcare system. The design conformed to the adopted techniques of policy-bounded qualitative research, merging thematic coding of policy documents and exemplary case evidence. Thematic analysis was conducted using the template proposed by Braun and Clarke. 5 It has enabled the examination of the mechanisms by which systemic racism pervades patient outcomes, the workforce, and regulation.
Data Sources
The publicly available sources were specifically chosen for breadth and applicability. These included:
a. Large-scale survey databases regarding healthcare access and demographics (eg, the Canadian Community Health Survey 6 ).
b. Government reports and audits (eg, Truth and Reconciliation Commission, 1 In Plain Sight, 2 Canadian Human Rights Commission, 3 and PHAC equity assessments 4 ).
c. Professional association documents (eg, CMA perspectives on systemic racism 7 ).
d. Academic literature (eg, thematic analysis methods 5 and health equity studies 8 ).
e. Investigative and media coverage of systemic failings in healthcare access and professional regulation (eg, Sinclair, 9 Echaquan, 10 and Akinbiyi 11 ).
f. Legal and tribunal documents, including litigation related to provider discrimination. 11
g. Grey literature on internationally trained physicians (eg, Radius SFU community report 12 and CBC coverage 13 ).
h. Workforce datasets (eg, CIHI’s 2023 Health Workforce Quick Stats 14 ).
Inclusion Criteria
Documents were included if they:
Responding to racial/ethnic disparities in Canadian healthcare (in patient care or workforce areas)
Embedded case evidence, policy recommendations, or recorded empirical data;
They were published between 2000 and 2025, ensuring contemporary relevance. 8
Case studies, such as those of Brian Sinclair, 9 Joyce Echaquan, 10 Dr. Amos Akinbiyi, 11 and a pseudonymized, globally educated doctor (“Dr. Ramirez”), were retained due to their national recognition and demonstration of systemic failure.
Data Extraction and Analysis
The papers were closely studied and coded thematically in three phases:
A.
B.
C.
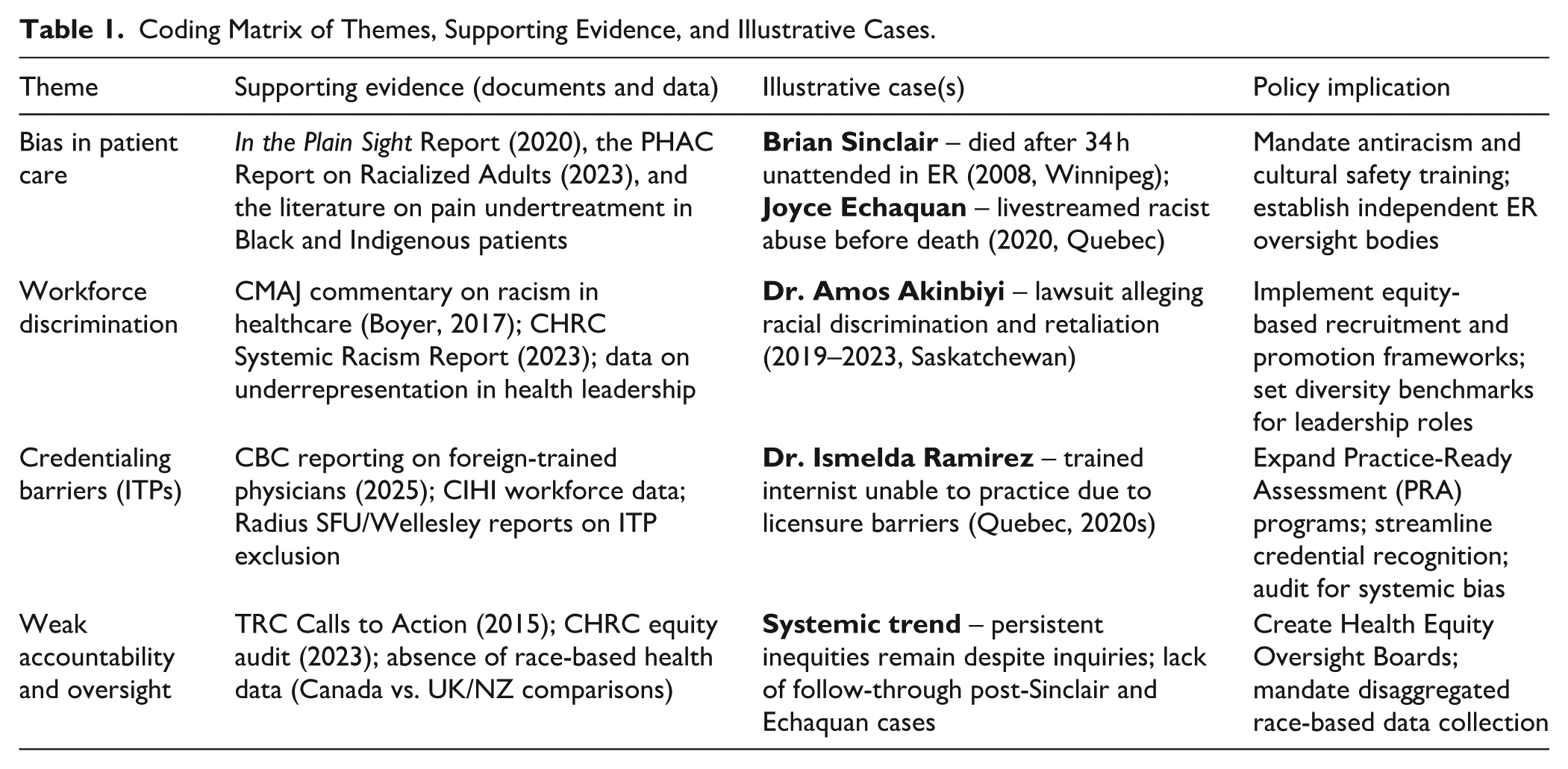
D. A coding matrix (Table 1) was used to triangulate data sources, themes, supporting evidence, and policy links.
Figure 1 illustrates the conceptual framework developed in this study, mapping the interlocking domains through which systemic racism is embedded in Canadian healthcare. These include biases in patient care, workforce discrimination, credentialing barriers, and gaps in institutional accountability. The framework underscores how these domains reinforce each other and highlights policy entry points for intervention.

Interlocking domains of systemic racism in Canadian healthcare.
Result
This section presents the findings organized into 4 thematic domains: bias in patient care, workforce discrimination, credentialing barriers for internationally trained physicians (ITPs), and institutional accountability. Evidence was drawn from publicly available inquiries, academic literature, workforce data, and case studies.
Bias in Patient Care
Systemic racism is responsible for differential treatment and disparities in outcomes between indigenous and racialized patients. Studies such as plain sight and PHAC health inequalities analysis reveal that racialized patients are at a higher likelihood of being misdiagnosed, undertreated for pain, or overlooked in emergency rooms.2,4
Most egregiously, the 2008 death of Brian Sinclair, who died in a Winnipeg emergency room after 34 h of being untreated, is an oft-cited instance of racially motivated medical neglect. 9 Similarly, Joyce Echaquan, an Atikamekw woman, streamed hospital staff’s racial insults just before she died in 2020. 10 These instances are typical of the discrimination faced by indigenous patients and reveal the life-threatening consequences of biased triage, cultural insensitivity, and implicit bias in clinical decision making.
Despite decades of documentation, including studies on pain undertreatment among Black and Indigenous patients, 15 these issues persist in both rural and urban settings. These findings reaffirm the need for mandated cultural safety and antiracism training for frontline healthcare workers.
Workforce Discrimination
Black, Indigenous, and racialized healthcare professionals have been excluded, targeted by microaggressions, and denied equal access to career advancement.3,7 The Canadian Human Rights Commission and CMAJ have observed underrepresentation in leadership roles and the persistence of disrespectful workplace environments.
One such case is that of Dr. Amos Akinbiyi, a Black emergency doctor in Saskatchewan who brought a discrimination suit against the Saskatchewan Health Authority following allegations of reprisal for having reported systemic racism. 11 It is a case that illustrates the institutionally entrenched reluctance toward equity advocacy and the professional risks entailed in being a racialized doctor.
Data on leadership reinforce this gap: Racialized doctors continue to be underrepresented in health management positions, and career advancement-related mentorship frameworks continue to be lacking.3,12 Such trends indicate a structural inability to retain and promote racialized healthcare workers.
Credentialing Issues Confronting Internationally Trained Physicians
International medical graduates (IMGs) in Canada face a disproportionately long, expensive, and complex path to licensure. Reports by the CBC News and Radius SFU document multiple structural hurdles, including redundant examinations, limited residency placements, and opaque recognition processes.12,13
The composite case of Dr. Ismelda Ramirez, a highly qualified physician unable to secure licensure despite prior international practice, reflects a common trajectory among ITPs. Many are relegated to non-clinical roles despite meeting educational standards.
According to the CIHI, only 13.6% of immigrant International Medical Graduate (IMG) secure Canadian licensure, despite 84.7% having held medical licenses abroad. 14 Pharmacists and physicians were most likely to be internationally trained (35% and 27%, respectively), whereas only 10% of RNs came from international backgrounds. These disparities suggest that licensing bottlenecks are both professional-specific and systemic.
Weak Accountability and Oversight
Despite numerous commissions and inquiries having found systemic racism in the healthcare of Canadian provinces, recommendations remain, for the most part, unimplemented. In 2015, the Truth and Reconciliation Commission (TRC) issued 94 Calls to Action, which included a number explicitly related to discrimination in healthcare;1,8 however, very few have been systematically upheld in health systems.
Similarly, the Viens Commission and CHRC Equity Audit confirmed the existence of systemic racism and suggested structural reform.2,3 However, such progress has been undone due to the lack of enforcement-based mechanisms of accountability and transparency in data.
For instance, the CIHI workforce datasets do not capture the racial or indigenous identity of healthcare providers. 12 Without race-based data, it remains difficult to monitor progress on equity goals or to hold institutions accountable. Compared to international frameworks, such as the NHS Workforce Race Equality Standard in the UK and New Zealand’s Te Tiriti o Waitangi framework, Canada’s data and governance gaps are stark.16,17
Table 1: Coding Matrix of Systemic Racism Themes in Canadian Healthcare. This matrix outlines the 4 major thematic domains identified through qualitative analysis of documents. For each theme, representative data sources, illustrative case examples, and corresponding policy implications are presented. Table 1 demonstrates how evidence was triangulated across documents, real-world events, and institutional responses.
Coding Matrix of Themes, Supporting Evidence, and Illustrative Cases.
A summary of the thematic findings, including key insights and representative sources, is presented in Table 2 (see also Table 1 for the coding matrix).
Summary of Thematic Findings.

Table 2 provides a synthesized overview of the core findings across the 4 thematic areas. Each row presents the central insight derived from the data, accompanied by corresponding illustrative cases and reference sources that exemplify these patterns. Case examples correspond to citations,9 -11 in the reference list. This summary provides a high-level understanding of how systemic racism operates at multiple levels within the healthcare system.
Discussion and Policy Implications
The findings of this study validate that systemic discrimination in healthcare is perpetuated through action (discriminatory regulations or organizational structures) and inaction (lack of implementing reforms). Discrimination in clinical interactions, exclusion of racialized professionals, and disjointed oversight demonstrate how ingrained these problems are.
Historic provincial differences in health status and service use have been reported over the past decades, reflecting the patchwork and incoherent nature of Canadian health equity policies across provinces. 18 Such differences make it clear that consistent, coordinated pan-Canadian policy initiatives are warranted, going beyond periodic reports and voluntary recommendations.
In making successful interventions, the eight-fold path to policy analysis, as outlined by Bardach and Patashnik, offers a helpful process for structured decision-making. 19 Applying the model can help identify where institutions’ incentives, administration, and areas of government support perpetuate inequalities.
The global paradigm offers teachable opportunities. Britain’s Workforce Race Equality Standard (WRES) requires all NHS trusts to undertake mandatory equity audits, which adds greater transparency in the matter of workplace racism and progress tracking. 16 Similarly, New Zealand’s Te Tiriti o Waitangi framework incorporates indigenous partnerships and accountability in health planning, providing a rights-based framework for indigenous health equity. 17
However, similar requirements do not exist in Canada. Institutions are not held responsible because of the lack of race-based health statistics, ineffective enforcement of anti-discrimination policies, and insufficient representation of racialized professionals in decision-making positions.
While race-based data are essential for monitoring disparities, governance frameworks must safeguard against potential misuse, misapplication, or discrimination, concerns raised by equity advocates, particularly in reference to U.S. practices.
Recent Canadian research confirms that anti-black racism and other forms of discrimination persist across all levels of the healthcare system. A national qualitative study by Williams et al 20 documented how racialized healthcare users and professionals continue to face exclusion, tokenization, and institutional mistrust within mainstream settings. These findings align with the study’s thematic analysis, reinforcing the need for urgent and systemic reform. Encouragingly, recent federal investments, including over $47 million to enhance the health workforce data infrastructure, physician mobility, and credential recognition, signal growing national momentum to address these systemic barriers in workforce planning and inclusion. Provinces integrate mandatory cultural safety training into accreditation frameworks and licensing standards. 21
To fill such gaps, the following policy recommendations are necessary:
Legislate antiracism mandates within health acts and professional practice guidelines.
Mandate the collection of race-based data across all jurisdictions.
Expand and fast-track credential recognition for internationally educated professionals.
Provide cultural safety and equity training for all licensed providers.
Establish independent oversight bodies to monitor the implementation and outcomes of health equity initiatives.
Without enforceable reform, Canada’s universal healthcare system will continue to perpetuate the inequalities it aims to eliminate.
Limitations and Future Research
This project took the form of a qualitative document study and did not incorporate interviews, focus groups, or other primary data-collection modes. Consequently, the results rely on the content available in public documents and may not reflect the full spectrum of lived experiences or informal organizational dynamics. We were unable to conduct intersectional or subgroup analyses because of a lack of race-disaggregated workforce data in most Canadian databases, such as CIHI’s QuickStats. Where direct measures were unavailable, proxy indicators (eg, country of training) were employed.
Cases were selected from news reports and public inquests, and hence, potentially possess reporting biases or are prone to narrative framing. Although an attempt was made to include peer-reviewed scholarship and court filings, the selection had to be selective in its scope. It could potentially have excluded pertinent unpublished or community-based scholarships.
Future Research Should Prioritize
As structural racism is multifaceted and adaptive, ongoing empirical studies are essential for monitoring progress, designing effective interventions, and holding institutions accountable.
Future research could benefit from incorporating direct interaction methods, such as interviews or participatory research involving racialized patients and foreign-trained doctors. Long-term studies on the effects of equity reforms and cross-jurisdictional research, particularly those involving other systems, such as the UK’s WRES and New Zealand’s Te Tiriti o Waitangi framework, could provide more detailed evidence for structural change. Most importantly, research using a race-disaggregated workforce and patient data requires empirical investigation to monitor progress, identify gaps in implementation, and hold institutions accountable for their actions.
Conclusion
This paper reveals that systemic racism in Canadian healthcare is not a case of sporadic events, but a result of structural design inherent in clinical practice, workforce policies, and organizational decision-making. Based on public inquiry reports, real-life case examples, and peer-reviewed evidence, it is clear that racial disparities are ingrained in the manner in which care is provided and who is licensed to offer it. Despite universal access, racialized patients and internationally educated professionals (IEPs)/internationally trained professionals (ITPs) continue to be overwhelmingly denied/adversely harmed.1 -4,8 -15
Despite numerous commissions and policy reports such as the Truth and Reconciliation Commission, 1 the Viens Report, 2 and the CHRC equity audit, 3 Canada’s enforcement mechanisms have proven ineffective in translating the acknowledgment of racism into systemic reform. In sharp contrast, the UK’s Workforce Race Equality Standard (WRES) 16 and the Te Tiriti o Waitangi-based framework 17 in New Zealand have no equivalent national plan or accountability mechanism in the Canadian healthcare system.
The reform of policy ought, then, to transcend rhetorical assurances. Equity-facilitating strategies include:
i. Incorporate antiracism provisions in the provincial and federal health acts 19 ;
ii. Require collection of race-based data to track disparities and monitor progress 18 ;
iii. Reform credentialing and licensing for ITPs, providing transparent and equitable access to enhance licensing equity and workforce planning12-14,21;
iv. Standardize cultural safety training and accountability mechanisms across jurisdictions8,15;
v. Craft stand-alone oversight units to monitor institutional equity progress and insist on compliance.3,16,17
Without these structural reforms, universal healthcare will remain aspirational for many racialized Canadians, and tragedies such as the deaths of Brian Sinclair and Joyce Echaquan will remain systemic and not exceptional. Equity must be built into the healthcare architecture and not added afterward, and the time for performative acknowledgment has passed. What is now needed is coordinated, enforceable, and measurable policy actions across all levels of the health system.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251386672 – Supplemental material for Systemic Racism in Canadian Healthcare: A Policy and Equity Analysis
Supplemental material, sj-docx-1-jpc-10.1177_21501319251386672 for Systemic Racism in Canadian Healthcare: A Policy and Equity Analysis by Kola Adegoke, Abimbola Adegoke, Deborah Dawodu and Temitope Kayode in Journal of Primary Care & Community Health
Supplemental Material
sj-xlsx-2-jpc-10.1177_21501319251386672 – Supplemental material for Systemic Racism in Canadian Healthcare: A Policy and Equity Analysis
Supplemental material, sj-xlsx-2-jpc-10.1177_21501319251386672 for Systemic Racism in Canadian Healthcare: A Policy and Equity Analysis by Kola Adegoke, Abimbola Adegoke, Deborah Dawodu and Temitope Kayode in Journal of Primary Care & Community Health
Footnotes
Ethical Considerations
This research used only publicly published documents; no institutional ethics approval was necessary. It is worth noting, however, that ethical diligence was observed in the presentation of sensitive content, avoiding sensationalism and framing case narratives within a systemic analysis rather than individual blame. This study did not involve human or animal subjects, and no new data were collected.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
Conceptualization, K.A. and A.A.; methodology, K.A.; validation, K.A., A.A., and D.D.; formal analysis, K.A.; investigation, K.A. and A.A.; resources, K.A. and T.K.; data curation, K.A.; writing – original draft preparation, K.A.; writing – review and editing, A.A., D.D., and T.K.; visualization, K.A.; supervision, A.A.; project administration, K.A.; funding acquisition, A.A. All authors have read and agreed to the published version of the manuscript. K.A. and A.A. contributed equally to this work as first authors. D.D. and T.K. also contributed equally to this work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data supporting the findings of this study are openly available in the Open Science Framework (OSF) at ![]() . This includes all the coded documents, case summaries, and analytic frameworks referenced in the manuscript. The dataset comprised only publicly available documents and did not include any identifiable or sensitive personal information. No new data were created or analyzed in this study. Data sharing was not performed in this study.
. This includes all the coded documents, case summaries, and analytic frameworks referenced in the manuscript. The dataset comprised only publicly available documents and did not include any identifiable or sensitive personal information. No new data were created or analyzed in this study. Data sharing was not performed in this study.
The OSF repository includes:
● The full thematic coding framework
● Case study summaries and legal references
● Workforce data tables (from CIHI QuickStats)
● Annotated bibliography and reference matrix
● Final manuscript with Vancouver-style referencing
● Stata command script used for random sampling
● Supplementary files:
○ Systemic_Racism_Canadian_Healthcare_Dataset.xlsx
○ Systemic_Racism_Canadian_Healthcare_Dataset.docx
All materials originated from publicly available sources and do not include any identifiable or sensitive personal information. No new human subject data were collected or analyzed. Data were curated to ensure the reproducibility of the policy analysis.
Trial Registration/Grant No.
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.