
Abstract
Introduction:
To combat persistent health and social disparities, the VA Greater Los Angeles and its community partners piloted a novel vocational rehabilitation program that employed persons who have experienced homelessness (PEHs) as app-based food deliverers. The program focused on removing barriers to employment, providing subsidized electronic bicycles for deliveries and personal use; “priority status” as deliverers; and access to financial literacy coaching. We aimed to characterize program experiences, with a lens toward program scale-up.
Methods:
We conducted semi-structured interviews with a convenience sample of 6 participants and 5 vocational rehabilitation staff. Interviews explored motivations to participate (among participants), and program strengths/challenges. Data were analyzed using rapid qualitative methods.
Results:
PEHs reported high motivation to participate due to the e-bike and flexible scheduling of work duties. Interviewees reported positive program impacts including: financial relief; reduced transportation barriers; and improved mental health. Suggesting for improvement included enhanced technical support (with the app and e-bike); improved communication among program partners; and more individualized employment opportunities.
Conclusions:
These data suggest the value of this novel vocational rehabilitation model for PEHs. Specific recommendations for program scale-up include a centralized platform for participant technical support requests; and regular communication and data sharing agreements between implementation partners.
Introduction
Homelessness is associated with profound health disparities, including higher rates of chronic and communicable disease, poorer mental health outcomes, 1 and higher rates of all-cause mortality 2 among persons experiencing homelessness (PEHs) versus their housed counterparts. Here, we define PEHs as persons who have experienced sheltered or unsheltered homelessness (i.e., lacking a stable, safe, and adequate nighttime residence) 3 to highlight the dynamic nature of housing which may vacillate over time. Employment is often a key goal for PEHs and conceptualized as a pathway to improved physical and mental wellbeing through increased financial security, community integration, and stable housing. Though many PEHs desire to engage in meaningful employment, barriers to competitive employment associated with experiences of homelessness (e.g., lack of transportation, fear of discrimination, competing priorities [e.g., mental health treatment]) are often persistent, limiting access to employment for PEHs even as they attain housing. 4 Mitigating these barriers presents a potential opportunity to advance health equity for this vulnerable population.
While highly visible programs like “Housing First” 5 —which provides subsidies for housing and supportive services—improve housing among PEHs, 6 other services beyond the provision of housing, like vocational rehabilitation, are essential to support community integration and self-efficacy among PEHs. Vocational rehabilitation models (e.g., supportive employment) effectively improve employment outcomes among individuals with serious mental illness (SMI), a group that is disproportionately affected by housing instability. However, for individuals with SMI and housing instability, the challenges of obtaining and maintaining housing while managing mental health treatment create additional complexities to achieving vocational goals. 4
At the Department of Veteran Affairs (VA), there is widespread emphasis on the value of vocational rehabilitation services and the development of programs tailored toward vulnerable Veteran populations like those with SMI. Despite this, the proportion of Veterans with SMI successfully connecting with supported employment services (a vocational rehabilitation service specifically targeting individuals with SMI) is low, just over 1% nationally. 7 Furthermore, despite high rates of homelessness among individuals with SMI, research on vocational rehabilitation utilization and effectiveness for PEHs is scarce. Emerging studies show that evidence-based vocational rehabilitation services—often characterized by case management, care coordination, and harm reduction approaches 8 —can improve employment and housing outcomes for PEHs 9 ; however, additional work is needed to improve PEHs’ engagement and retention in vocational rehabilitation programs by addressing practical barriers to engagement such as transportation, the need for flexible schedules, and access to immediate income. As such, programs inside and outside the VA may require innovative adaptations that target these challenges alongside traditional vocational supports.
In 2022, the VA Greater Los Angeles worked with community partners to pilot a novel vocational rehabilitation program (“Pathways to Success”) that employed eligible PEHs as mobile application (app)-based food deliverers. The 6-month program incorporated fully subsidized electronic-bicycles (e-bikes) for work and personal use, “priority status” for deliveries, and access to financial literacy resources, aiming to reduce transportation barriers, provide flexible hours, and offer immediate earnings. To improve the program and inform plans for scale-up to other sites, we used qualitative methods to examine participant and staff experiences in this pilot. Findings add to existing vocational rehabilitation literature by illustrating how integrating adaptations in program design may improve engagement among vulnerable populations. Lessons learned from this VA effort may apply to other healthcare systems and community-based homeless service settings.
Methods
Program Description
Pathways to Success was a 6-month vocational rehabilitation pilot program based in an urban VA facility; it employed a small cohort of eligible PEHs (n = 12) as app-based food deliverers and aimed to: (1) increase PEHs’ financial self-sufficiency (i.e., monthly income); and (2) enhance access to financial empowerment resources. To be eligible to participate, PEHs needed to be utilizing VA homeless program services (a proxy for homeless experiences), have access to a smartphone with data, and a valid state identification card; participants also had to consent to a background check. Program components were developed via organizational partnerships as described in Figure 1 and detailed below.

“Pathways to Success” organizational partners and role/program components.
VA Vocational Rehabilitation: Recruitment and Engagement of Eligible Veterans
Vocational rehabilitation staff recruited eligible PEHs from their existing caseloads to participate in Pathways to Success. The VA hosted a 1-day training and onboarding session for participating PEHs. There, PEHs were provided a program overview, received their e-bikes, and received training to participate in the program. After onboarding, vocational rehabilitation staff continued to support Veterans in their vocational rehabilitation goals (e.g., by assisting with employment applications) during their participation in Pathways to Success.
Food Delivery Mobile Application: Employment as Food Deliverers with Priority Status and Direct Payment Mechanism
Participating Veterans were employed as mobile app-based food deliverers. They were granted “priority status” which increased opportunities for more deliveries and higher earning deliveries. Veterans were provided a prepaid debit card where earnings were deposited immediately after each delivery.
Electronic Bicycle Vendor: Fully Subsidized E-Bike
All participating PEHs were provided a fully subsidized e-bike to use for food deliveries and for personal use. They also had access to an e-bike mechanic when needed. E-bikes were subsidized by the food delivery mobile application company.
Community-Based Organizations: On-Demand Financial Empowerment Resources
Participating Veterans were provided access to financial empowerment resources, including remote on-demand financial literacy courses and remote financial coaching. Examples of available financial literacy courses included “Auto-Financing For Beginners,” “Thriving In The Gig Economy,” and “Budgeting for Groceries.” Financial empowerment resources were subsidized by the food delivery mobile application company.
Data Collection
We obtained a roster of the first 12 pilot participants and all 9 vocational rehabilitation staff. We used letters and phone calls to invite all 12 participants for semi-structured phone interviews and interviewed 6. We used emails to invite all 9 VA pilot program staff for semi-structured interviews and successfully interviewed 5. All data collection and analyses were determined as non-research by the VA Greater Los Angeles Institutional Review Board administrator; verbal informed consent was provided by all interviewees.
Semi-structured phone interviews (~30 minutes each) were conducted with participating PEHs by 2 authors (TJP and EJ) and with staff by 1 author (TJP). Detailed notes were taken by additional authors (TJP, EJ, MC) during the interviews. Recordings were used to supplement interview notes. Interview guides and note-taking templates were developed collaboratively with VA vocational rehabilitation program leadership. To ascertain motivations for participating in the pilot, we asked PEHs about their prior employment experiences, how they learned about the program, and what interested them about it. We asked staff about program recruitment, their expectations for participants, and whether these expectations were met. We explored participant and staff perspectives about program features and impacts to understand which features were valuable and why. We asked all interviewees about challenges experienced by participants. We asked staff about challenges implementing the program. Finally, we sought general feedback to improve experiences with VA vocational rehabilitation programming, and suggestions that would support scale-up.
We used VA’s electronic health record “problem lists” (i.e., a list of diagnoses, by patient) to gather basic demographic (age, sex) and mental health diagnostic information about participants. We were unable to gather quantitative data about deliveries and employment outcomes as these were maintained by community partners. We queried staff about their role and years of experience in VA using a brief survey.
Data Analyses
Two authors (TJP and SG) developed an interview summary template for rapid qualitative analyses10,11 derived from the interview questions. Applying rapid-qualitative analysis methods, 3 authors (TJP, EJ, MC) independently used this template to develop structured summaries of 2 interviews to ensure consistent use of template categories. Authors worked iteratively to refine the template, applying the finalized template to each interview field-notes by 2 authors (EJ and MC). Authors did not develop summaries for interviews they conducted. Matrix analyses 12 were used to identify salient perspectives on positive aspects and challenges of the pilot program experience, with a lens toward improving the program and informing its expansion.
Results
Sample
Interviewed PEHs (n = 6) were men and women with a diversity of race/ethnicity. On average, interviewed participants were 35 ± 7 years old and most had a post-traumatic stress disorder diagnosis. Interviewed staff represented a diverse range of positions, supervisory responsibilities, and years employed in their current role.
Interview Findings
Salient findings from the interviews are summarized in Table 1 and detailed below. Interviewees reported many positive program impacts, including financial relief, increased mobility via e-bikes, and improved mental health and wellbeing. Participants also described challenges, including receiving technical support (for the mobile-app and e-bikes) and a desire for strengthened communication between pilot program partners.
Key Findings and Exemplar Quotations.
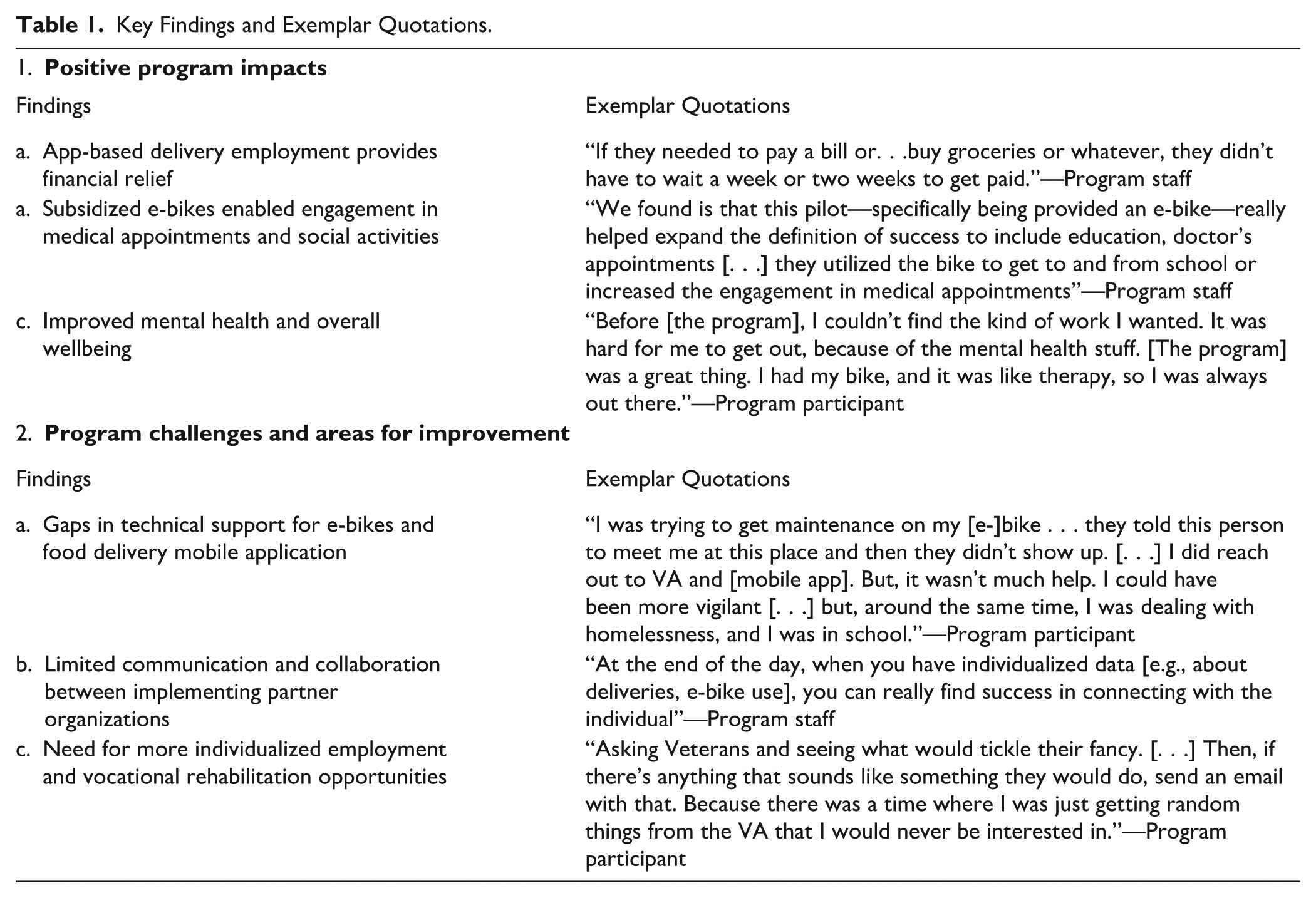
App-Based Delivery Employment Led to Financial Relief
Most interviewees reported positive effects on PEHs’ finances. Relative to other employment options, app-based delivery offered more flexible and immediate earnings, allowing participants to address immediate basic needs (e.g., groceries). One staff reflected on the challenge of finding jobs that “meet all our Veterans’ expectations and needs,” but noted that this program was “really good” because it “gave the Veteran flexibility and power to do their own thing.” Overall, interviewees felt that app-based delivery offered a “good, reliable source of income” and that for participating PEHs, Pathways to Success was “a steppingstone” toward achieving their vocational goals.
Subsidized e-bikes Enabled Engagement in Medical Appointments and Social Activities
Participants reported that they were highly motivated to participate in Pathways to Success due to the e-bike. One participant stated that the e-bike was the “main reason” they joined. Another participant explained that he “would not have been able to [participate]” without the e-bike due to transportation barriers. Two staff emphasized the positive impact that mitigating transportation barriers had for participants via the e-bike: they felt that participants having “access to increased mobility [could not] be overstated enough.” Participants reported using the e-bike for personal and professional use (e.g., medical appointments, attending classes) in addition to food delivery.
Several participants reported improved social connections and highlighted increased daily interactions with community members as a positive aspect of Pathways to Success. Participants shared examples of connections they made due to this pilot, including delivering food to sick or elderly individuals and forming friendships with other participants.
Improved Mental Health and Overall Wellbeing
Most participants reported enhanced wellbeing due to Pathways to Success. Participants reported feeling more emotionally secure due to increased income, access to transportation, and “having a real sense of employment.” The e-bike offered participants an alternative to public transportation, which is sometimes a reportedly less preferred mode of transportation for several PEHs due to their mental health condition(s). Similarly, for PEHs whose mental health conditions may have created difficulties in prior jobs, the pilot program offered a viable alternative. Overall, several PEHs reported feeling a gained sense of community, respect, and “morale” due to employment.
In addition to the program overall providing a sense of enhanced wellbeing, both participating PEHs and staff highlighted the smooth and “expedited” PEH onboarding process. The 1-day onboarding process included program orientation as well as time to practice using the e-bike. Most staff and participants felt that the streamlined, 1-day onboarding process both eased anxiety due to unemployment and increased access to the program, though 1 PEH mentioned a desire for additional e-bike practice and training.
Gaps in Technical Support for e-bikes and Food Delivery Mobile Application
Several staff and most participants reported needing to access technical support for e-bikes (e.g., bike maintenance) and the food delivery mobile application (e.g., safety on routes, priority status malfunctions). While the program did offer an e-bike mechanic, participants mentioned that the mechanic was particularly inaccessible due to lack of transportation. In addition, coordinating mechanic appointments was a challenge. Particularly for PEHs, coordination needed to be more streamlined: 1 participant suggested more consistent program coordination and communication—perhaps through 1 point of contact—to improve the PEH experience in Pathways to Success. In addition, a few participants reported stolen e-bikes and were unable to recover the e-bike or identify alternative transportation to complete deliveries. Several participants also experienced technical challenges utilizing the food delivery mobile application, including not feeling safe on suggested routes, direct deposit malfunctions, and priority status malfunctions. Staff corroborated these various challenges, stating that the main “challenge was on the back-end support.”
Limited Communication and Collaboration Between Implementing Partner Organizations
Related to the prior finding, several staff emphasized a need for increased communication with program partners for troubleshooting issues experienced by participating PEHs and ongoing program evaluation. Staff felt that increased and ongoing collaboration between implementing partner organizations (i.e., VA vocational rehabilitation, e-bike company, and mobile app company) would alleviate some of the challenges faced by participants and staff. While all staff agreed that the pilot program was a success, most agreed that the biggest challenge was coordinating communication with partners when needed (e.g., to navigate software issues, coordinating mechanic appointments, addressing bike theft). In addition to coordination for on-going program support, some staff felt that increased communication between implementing partners may have been beneficial for program evaluation. Of note, none of the interviewed participants participated in financial literacy courses or coaching, due to various reasons including scheduling, lack of interest, lack of perceived need, and competing priorities.
Need for More Individualized Employment and Vocational Rehabilitation Opportunities
We asked interviewees about their perceptions about VA vocational rehabilitation programming and opportunities. When asked about the best methods to let PEHs know about vocational rehabilitation programs, most participants preferred direct and more personalized messaging (e.g., texting, email) that are tailored to their professional interests as opposed to more broad communications about opportunities (e.g., email blasts). Several PEHs shared a desire for a centralized platform to post and answer questions related to employment opportunities.
Discussion
Using qualitative methods, we characterized participant and staff perspectives about a novel vocational rehabilitation pilot tailored to reduce barriers to employment for PEHs. Immediate financial relief, flexible scheduling, and increased access to transportation were key factors that incentivized participation, as well as stated program benefits. Technological issues presented challenges to participating in and implementing the program, and many interviewees desired streamlined communication channels for technical support and strengthened partnerships among implementing organizations. Despite challenges, interviewees reported overall improved financial stability, mobility, mental health and community engagement from program participation.
Participants’ appreciation of app-based food delivery as employment suggests that jobs, like the gig-economy, that prioritize flexible hours and less oversight may be a viable option for PEHs with specific needs and competing priorities (e.g., full-time students, individuals with serious mental illness, individuals searching for more permanent work, individuals searching for housing). To the best of our knowledge, this is the first study to explore the impacts of a vocational rehabilitation program integrating gig-economy employment with subsidized transportation for PEHs. In addition, the relatively streamlined onboarding process and training reduced barriers to initial employment and facilitated more immediate work. The provision of transportation, specifically via a subsided e-bike, not only reduced barriers to employment, but also provided additional benefits by encouraging increased physical activity and community engagement, and by reducing barriers to medical appointments and other social services. The independent nature of the e-bike, as opposed to public transportation, reduced additional barriers related to mental health concerns (e.g., anxiety, PTSD). Future iterations of vocational rehabilitation programs for vulnerable groups may benefit from similarly targeting structural barriers that disproportionately affect PEHs—such as transportation costs and inflexible work hours. In doing so, programs may address inequities in employment access for groups marginalized by homelessness, mental illness, and other intersecting factors. Future iterations may also benefit from increased understanding of desired financial empowerment resources and preferred modalities.
This project has limitations. As a single organizational case study of a small pilot program, these findings may not extrapolate outside the VA, or to VA populations in different settings. We interviewed a small convenience sample of participants, and the perspectives described may not reflect all participants in the pilot program. In addition, given the study’s small sample size, we omit specific demographic characteristics (e.g., race/ethnicity) to protect the anonymity of the pilot program participants. Moreover, participants with strong views on the pilot program may have been more likely to participate in interviews. We were unable to gather quantitative data about deliveries, e-bike utilization, employment outcomes, which would be important in future quality improvement efforts. However, the data we collected suggest that this pilot program—and its focus on PEHs—was valued and may hold promise in diverse settings. Lastly, implementation of the pilot program relied heavily on partnerships to provide funding and infrastructure (e.g., the mobile application); implementation of a multi-faceted program like this pilot would likely face additional logistical challenges without such partnerships. Relatedly, we were unable to gather cost estimates for the pilot program. Future research should examine the costs, effectiveness, and sustainability of such adaptations, including impacts on employment stability, income, and broader health equity outcomes.
Conclusions
Developing tailored vocational rehabilitation programs for vulnerable populations, and for PEHs, may be a valuable tool to promote health equity. In this pilot, employment via app-based delivery with fully subsidized transportation options was positively received by participants, provided timely financial relief, increased engagement in other important community activities, and reduced overall stress and anxiety, and may hold promise in community-based mental health or homeless service agencies, or other healthcare systems. Qualitative findings highlight vocational rehabilitation program adaptations, including transportation supports, flexible work structures, and streamlining technical assistance, that may improve engagement and retention among PEHs and other vulnerable populations. Future efforts would be strengthened with embedded evaluation efforts, including quantifying deliveries and employment outcomes, and gathering structured data about program satisfaction from patients and all involved partner organizations.
Footnotes
Acknowledgements
The authors are grateful to VA QUERI for the opportunity for continued training that supported this study. The authors would also like to acknowledge the VA staff and Veterans who made this work possible.
List of Abbreviations
PEHs = persons experiencing homelessness
SUD = substance use disorder
VA = Department of Veteran Affairs
Author’s Note
The funders had no role in study design; collection, analysis, and interpretation of data; writing the manuscript; or the decision to submit the manuscript for publication. Peter J. Stigers is now affiliated to Vocational Rehabilitation Services, VA Greater Los Angeles Healthcare System, Los Angeles, CA, USA
Ethical Considerations
All quality improvement activities described in this manuscript were deemed nonresearch by the VA Greater Los Angeles’ Institutional Review Board (IRB) administrator.
Consent to Participate
All participants provided verbal informed consent for project participation.
Consent for Publication
Not applicable.
Author Contributions
TJP: Conceptualization, Methodology, Analysis, Writing – Original Draft, Writing – Review and Editing. MC: Methdology, Analysis, Writing – Original Draft, Writing – Review and Editing. EJ: Analysis, Writing – Review and Editing. PJS: Conceptualization, Writing – Review and Editing. PR: Conceptualization, Writing – Review and Editing. SG: Conceptualization, Methodology, Writing – Review and Editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: TJP was supported in part by a VA Quality Enhancement Research Initiative (QUERI) supplement award to Housing Transitions QUERI (PIs: Finley, Gabrielian).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Non-Anonymized Methods Sections
[Line 114]
All data collection and analyses were determined as non-research by the VA Greater Los Angeles Institutional Review Board administrator; verbal informed consent was provided by all interviewees.
[Line 118]
Semi-structured phone interviews (~30 minutes each) were conducted with participating PEH by 2 authors (TJP and EJ) and with staff by 1 author (TJP). Detailed notes were taken by additional authors (TJP, EJ, MC) during the interviews.
[Line 139]
Two authors (TJP and SG) developed a template for rapid qualitative analyses derived from the interview questions. Applying rapid-qualitative analysis methods, 3 authors (TJP, EJ, MC) independently used this template to developed structured summaries of 2 interviews to ensure consistent use of template categories. Authors worked iteratively to refine the template, applying the finalized template to each interview field-notes by 2 authors (EJ and MC).