
Abstract
Background:
The country’s ageing population, particularly in rural areas, presents growing public health and policy challenges. Gender-based disparities in socioeconomic domains further exacerbate vulnerabilities among the elderly. Assessing ageing through domains that incorporate local factors is essential for designing effective interventions.
Objectives:
This study aimed to: (1) assess active ageing levels among rural older adults using a locally adapted Active Ageing Index (AAI) aligned with the WHO framework; (2) examine the association between AAI scores and sociodemographic factors, including age, gender, marital status, education, employment, and social class; and (3) explore gender-based disparities in economic and social security indicators—such as land ownership, income sufficiency, and pension access—that influence active ageing through secondary analysis.
Methods:
A community-based cross-sectional study was conducted among 355 older adults in rural study area. The AAI was constructed using domain-based indicators across health, participation, and security, and categorised into Poor, Moderate, and Good levels. Associations with sociodemographic variables were assessed using Chi-square tests. For the third objective, gender differences in economic and security-related indicators were assessed through secondary analysis involving cross-tabulations and chi-square tests.
Results:
Among the participants, 53.5% had Good AAI scores, 40.3% Moderate, and 6.2% Poor. A significant association was observed between AAI and social class (χ² = 7.02, p = .0306). Gender was not significantly associated with overall AAI categories; however, Secondary analysis of economic indicators within the Security domain revealed that women had lower land ownership, pension access, and income sufficiency compared to men.
Conclusion:
Active Ageing Index was significantly associated with social class. While overall AAI scores did not differ significantly by gender, domain-level analysis demonstrated that socio-economic disadvantages place elderly women at greater risk of security. These results underscore the importance of gender-sensitive policies and interventions to strengthen the Security pillar of active ageing in rural India, ensuring equitable opportunities for all older adults.
Keywords
Introduction
A profound demographic shift is underway globally, with a staggering surge in the population aged 60 years and above. Once perceived as a challenge limited to industrialised nations, population ageing has emerged as a critical concern for developing countries like India, where demographic transitions are outpacing economic and infrastructural development.1 -3 India’s health systems and social protection mechanisms face increasing pressure, particularly in rural regions, necessitating community-based and context-specific solutions. The discourse around ageing must evolve beyond biomedical approaches to address the socio-economic and dignity-related challenges faced by rural elders.4,5
Global and National Ageing Trends
According to the United Nations World Population Prospects 2022, the global population aged 60 years and above is expected to double from 1.05 billion in 2020 to 2.1 billion by 2050. 6 This unprecedented demographic transition poses critical implications for health systems, pension structures, care provision, and the overall perception of ageing. Developing nations, particularly in rural or underserved areas, often lack the preparedness to manage these demographic pressures.
India, now the world’s most populous country, is experiencing a swift demographic shift. The proportion of Indians aged 60 years and above is projected to rise from 10.1% in 2021 to 19.9% by 2050—translating to over 319 million older adults. 7 More than 70% of these individuals reside in rural areas, where access to healthcare, transport, eldercare, and economic safety nets remains severely limited. These communities struggle with chronic illnesses, disability, absence of pension coverage, and increasing social isolation. 8 Thus, ageing in rural India reflects not only functional limitations but also compounded marginalisation due to inadequate infrastructure and socio-economic vulnerability.
Concept of Active Ageing and the WHO Framework
Recognising the multi-dimensional nature of ageing, the World Health Organisation (WHO) introduced the concept of Active Ageing in 2002. Unlike conventional approaches that prioritise disease control or longevity, active ageing emphasises optimising opportunities for health, participation, and security to enhance quality of life as people age. 9
The framework is anchored in 3 pillars:
Health: Enabling functional independence and access to preventive and curative healthcare supports mobility, emotional well-being, and community participation. 10
Participation: Continued engagement in social, economic, cultural, and civic activities fosters mental health and strengthens intergenerational ties. 11
Security: Economic protection, housing stability, and freedom from abuse ensure dignity and reduce vulnerability in old age. 12
To operationalise this concept, the European Commission and the United Nations Economic Commission for Europe (UNECE) developed the Active Ageing Index (AAI)—a composite measure of ageing outcomes across 3 domains. While the AAI has been widely applied in European contexts, its application in India remains limited. This is especially true for rural areas, where socio-cultural norms, infrastructure, and economic realities differ significantly from those in high-income countries. 13
Rural Ageing in India: Specific Challenges
Rural India presents unique and complex challenges for ageing populations. Many older adults are employed in informal sectors, lacking retirement benefits or financial security. 14 With limited access to formal social protection schemes, they depend heavily on family members who may themselves face economic hardship. Gender-based disparities exacerbate the situation—older women are more likely to experience widowhood, lower educational attainment, poor health, and reduced mobility. 15
Healthcare access remains a significant barrier. Rural regions are underserved in terms of trained health professionals and lack geriatric care infrastructure. 16 Geographic isolation, low community engagement, and the migration of younger family members to urban areas increase the risk of loneliness and neglect. Despite these challenges, India lacks a standardised tool to measure quality of life or levels of active ageing, particularly for rural populations. There is a critical need for culturally adapted instruments that reflect the heterogeneity of rural ageing and inform targeted policy interventions. 17
Contribution and Policy Relevance
This study makes a significant contribution to the emerging literature on active ageing in India, particularly in under-researched rural settings. By contextualising the WHO Active Ageing Index (AAI) to reflect local realities and applying it through a community-based framework, this research not only provides empirical evidence but also offers a replicable methodological model for similar low-resource contexts. The use of a validated and structured composite tool allows for meaningful intra-population comparisons and supports the design of age-sensitive programming across key domains such as healthcare, pensions, housing, and social protection.
Furthermore, the findings align closely with India’s commitments to the United Nations Sustainable Development Goals (SDGs), specifically:
By highlighting the relationship of ageing, gender, poverty, and access to services, the study presents a foundational step towards equitable and inclusive development strategies. It reframes ageing not merely as a health challenge but as a multidimensional policy concern with long-term demographic implications.18,19
Policy Integration
The National Policy for Senior Citizens (2011) acknowledges the compounded disadvantages faced by elderly women—especially widowed, landless, and economically dependent individuals. Although it advocates for gender-sensitive measures, implementation at the grassroots remains sporadic and inadequate. Similarly, the National Social Assistance Programme (NSAP), through initiatives such as the Indira Gandhi National Old Age Pension Scheme (IGNOAPS) and Indira Gandhi National Widow Pension Scheme (IGNWPS), attempts to provide minimal support. However, low benefit amounts, poor awareness, and administrative bottlenecks often limit its effectiveness, especially for rural elderly women. This study provides empirical insight into these policy gaps and underscores the urgent need for more inclusive and gender-responsive reforms.20,21
Objectives of the Study
In light of this, the current research was formulated to fulfil the following aims:
To estimate the percentage of aged persons in a rural Indian context falling under poor, moderate, or good Active Ageing Index (AAI) scores, based on a multi-dimensional scoring framework incorporating health, participation, and security
To investigate the relationship between AAI scores and some sociodemographic variables, such as age, gender, marital status, educational level, occupational history, and wealth status.
To explore gender-based disparities in economic and social security indicators-such as land ownership, income sufficiency and pension access that influence Active ageing through secondary analysis.
Literature Review
Global and Indian Perspectives on Active Ageing
The WHO defines active ageing as optimising opportunities for health, participation, and security to improve quality of life in older age. 7 Foster and Walker 8 critique its European implementation, noting it often prioritises economic productivity over holistic well-being. Zaidi et al 6 developed the AAI across the EU, revealing persistent gender disparities despite high-income settings. Similarly, Haque et al 10 showed how localised AAI applications in Thailand informed regional policy interventions. Bosch-Farré et al 11 emphasised the biopsychosocial model as a more inclusive framework than traditional medicalised views.
In India, Guntupalli and Chakraborty 12 noted that elderly employment is largely necessity-driven, calling for localised ageing indicators. Studies from Assam, 13 Mangalore, 14 and Karnataka 15 highlighted widowhood, poor education, and social exclusion as key determinants of reduced quality of life, reinforcing the need for context-sensitive measures.
Interventions and Gender Disparities
Evidence from Mexico by Perez-Cuevas et al 16 showed structured active ageing programmes improved quality of life and occupational functioning, though effects vary by gender and context. The WHO-5 Wellbeing Index is validated as a robust tool across cultures.17,18
Ageing in India is shaped by sociodemographic and economic factors. About 29% of older adults have pensions or provident funds, but women are disproportionately without income. 19 Men often remain in the labour force longer, facing health risks, while widowhood increases economic vulnerability for women, who experience pronounced socio-economic disadvantages. 21 Agarwal documented barriers to land inheritance, Wani highlighted the need for updated rural poverty measures, 22 and Srivastava and Mohanty 17 reported over 70% of elderly women are financially dependent, with widowhood being a major vulnerability factor. 23 These inequities necessitate gender-sensitive ageing policies, as women remain underrepresented in employment and earn less, heightening poverty risks.24,25 Existing active ageing measures often overlook these disparities, highlighting the need for inclusive frameworks.26 -28
Research Gap
Gap in Application of Active Ageing Framework
Although the AAI is recognised globally, its application in rural India is limited. Most studies focus on isolated dimensions such as health or income, without integrating the comprehensive multi-domain AAI. Guntupalli and Chakraborty questioned the European model’s applicability due to cultural and socio-economic mismatches, and local adaptations remain minimal. Large datasets like LASI and BKPAI are fragmented and rarely support composite index creation. Few studies examine how AAI interacts with sociodemographic variables such as gender, education, and occupation. This study bridges that gap by developing a context-specific AAI.12,29 -31
Gap in Gender-Based Socioeconomic Disparity Analysis
Gender disparities in land ownership, pensions, and income are often analysed in isolation rather than through an intersectional ageing lens. In rural areas, older women’s active ageing outcomes are underexplored, while men also face challenges such as poor health and limited social support. This study examines these differences to determine whether active ageing interventions, particularly addressing “security,” adequately meet the diverse needs of older adults in India.22,23,32,33
Research Methodology
This section presents the structured strategy undertaken to examine levels of active ageing and its correlation with different sociodemographic characteristics in rural elders of the Study area. An adequately conceptualised methodology was critical to ascertain the validity, reliability, and contextual salience of evidence within a rural Indian context, considering the nuances of sociocultural and infrastructure realities influencing the experiences of ageing away from cities.
Study Design and Setting
A cross-sectional, community-based study design was utilised to measure active ageing and determine its sociodemographic factors. The field research was done in rural Karnataka, representing an appropriate microcosm for assessing rural Indian demographic trends (cross ref Supplemental Annexure 1).
Study Population and Sampling Technique
The study population consisted of individuals aged 60 years and above who were permanent residents of the selected villages and cognitively capable of providing informed consent. The inclusion criteria were: (a) age ≥60 years, (b) residency in the village for at least 6 months, and (c) absence of severe cognitive impairment. The exclusion criteria were individuals who were not available at their homes during 3 consecutive home visits.
A multistage sampling method was applied as follows:
•
•
•
• The final sample size was calculated as 355 using the finite population correction formula. This was based on a previous Indian study by Nair SB, which reported a 63.8% prevalence of moderate active ageing. The sample size was determined at a 95% confidence level, with a 5% margin of error, and included an additional 10% allowance for non-response. 34
Development of Data Collection Instrument
Data was gathered with a pre-validated, structured interview schedule prepared by combining items from internationally acclaimed tools7,35:
WHO Active Ageing Framework
Longitudinal Ageing Study in India (LASI)
Building Knowledge Base on Population Ageing in India (BKPAI)
WHO STEPS Questionnaire for NCD surveillance
The questionnaire was initially translated into Kannada (local language) and then back-translated to English to provide consistency. Pilot testing involving 20 older persons from a village nearby assisted with pretesting for clarity, time, and cultural acceptability. Revisions as needed were implemented prior to final administration. Internal consistency was measured for the questionnaire using Cronbach’s alpha constant method which was found to be favourable.36,37
The completed tool consisted of 5 modules:
Sociodemographic Profile
Sociodemographic profile consisted of age, gender, education, marital status, caste, religion, family composition, and socioeconomic status (SES) based on a revised Udai Pareekh Scale. 38
Health Domain
Health domain: self-rated health, history of chronic illness, dependency on ADL/IADL (utilising Katz and Lawton-Brody scales), psychological well-being through WHO-5 index, and habitual health behaviour (sleep and physical activity).
Participation Domain
Participation domain: measured involvement in household and community decision-making, organisational memberships, level of social interactions, and leadership within organisations.
Security Domain
Security domain: contained data regarding housing condition, sources of income, pension rights, financial independence, and eligibility for welfare programmes.
Support and Abuse Context
Support and abuse context: rated for elder neglect, abuse (verbal, financial, or physical), and presence of family or community support during illness or distress. 35
Construction of the Active Ageing Index (AAI)
The Active Ageing Index was developed using 3 pillars from the WHO framework: Health, Participation, and Security. Each domain included multiple indicators, which were scaled from 0 to 1 for comparability (cross ref Supplemental Table 1).
Health Domain Score: based on self-rated health (0 = poor to 1 = excellent), ADL/IADL dependency, and WHO-5 mental well-being (score >13 classified as good well-being).
Participation Domain Score: based on coded social roles (0 = no involvement, 0.5 = member, and 1 = office bearer).
Security Domain Score: included economic security and social protection. Home ownership was scored as 1.0 and dependent/rented accommodation as 0. Pension receipt added a weight of 0.2.
The AAI was calculated as the mean of the 3 domain scores and classified into:
Poor Active Ageing: AAI <0.50
Moderate Active Ageing: AAI 0.50 to 0.79
Good Active Ageing: AAI ≥ 0.80
Although gender disparities in economic resources were not originally included as a primary design focus, the information collected under the “Security” domain (income sources, pensions, financial dependency, and asset ownership) provided an opportunity to conduct a secondary analysis of gender-based differences. This post-hoc exploration addressed the third study objective.
Data Management and Statistical Analysis
The data were double-entered into Microsoft Excel and cleaned and coded after. SPSS Version 26 was used with cross-platform statistical investigation and representation from Python. For the first objective, descriptive statistics such as mean, standard deviation, frequencies, and proportions were used to construct and summarise the Active Ageing Index (AAI) and its pillar-wise scores. To address the second objective, the association between socio-demographic variables and AAI scores was examined using chi-square tests for categorical variables. For the third objective, a secondary analysis was carried out by disaggregating the economic and security-related variables by gender. Cross-tabulations and chi-square tests were employed to identify differences between men and women participants in access to economic resources and financial security. A p-value of <0.05 was considered statistically significant.
Descriptive Statistics
Percentages and frequencies for categorical variables; mean ± standard deviation for continuous variables.
Bivariate Analysis
Relationships of AAI categories to independent variables were examined via Chi-square tests for independence.
p-value
A p-value of <0.05 was deemed statistically significant.
Results
The Active Ageing Index (AAI) was calculated for the rural elderly in the Rural District study area.
Demographic Characteristics of the Study Population
Table 1 presents the socio-demographic profile of the 355 elderly respondents covered in the study. The table facilitates the setting of a contextual baseline in measuring variation in Active Ageing Index (AAI) scores among population subgroups.
Table Showing Sociodemographic Characteristics of Participants.

The demographic profile of study participants points out a number of significant patterns to ageing in rural Karnataka. More than half the elderly respondents (51.3%) were aged between 60 and 69 years, which suggests that the elderly population was relatively younger, and 14.1% were above 80 years. Women outnumbered men slightly, with 54% of the sample. Marriage status data indicates that 62% were married, with implications of possible emotional and social support, while the 28% widowed could be at higher risk, especially for women. Educationally, 42% of the sample were illiterate, and a mere 8% had reached secondary level or more. Occupationally, 40% were engaged in agriculture or informal activities, 9.3% were professional or skilled, and 50.7% were retired or unemployed, showing high dependency. Economically, 45% belonged to lower-middle or middle-income classes, 43% were below the poverty line, and a mere 12% were upper-middle or wealthy classes—showing high economic insecurity.
Distribution of Active Ageing Index (AAI) Categories
This section gives an overview of the proportion of Active Ageing Index (AAI) scores among the 355 elderly respondents, which have been divided into Poor, Moderate, and Good based on averaged scores over 3 domains—health, participation, and security. These classifications are indicative of each respondent’s degree of independence, social involvement, and access to support. Figure 1 presents a graphical summary of the number of respondents per AAI category.

Distribution of participants by active ageing index (AAI) categories.
Of the 355 rural older people who were surveyed, 53.5% (n = 190) were in Good AAI. 40.3% (n = 143) were in Moderate AAI; A low but significant 6.2% (n = 22) were classified as Poor AAI.
Association Between AAI and Sociodemographic Variables
This section of the research considers how AAI differs across main demographic and socioeconomic groups in order to identify populations at risk and inform interventions. It uses Chi-square analysis to examine associations between AAI and 6 variables: age, gender, education, marital status, Employment, and social class, and tests whether or not these variables affect active ageing outcomes in rural elderly.
Age Group and Active Ageing Index (AAI)
This sub-section examines the distribution of the Active Ageing Index (AAI) across different age groups. The 3 AAI levels—Poor, Moderate, and Good—are compared among 3 age ranges: 60 to 69, 70 to 79, and 80+ years. Table 2 presents the percentage distribution of participants in each AAI category by age group, gender, and Marital status.
Distribution of AAI Categories by Age group, Gender, and Marital status.
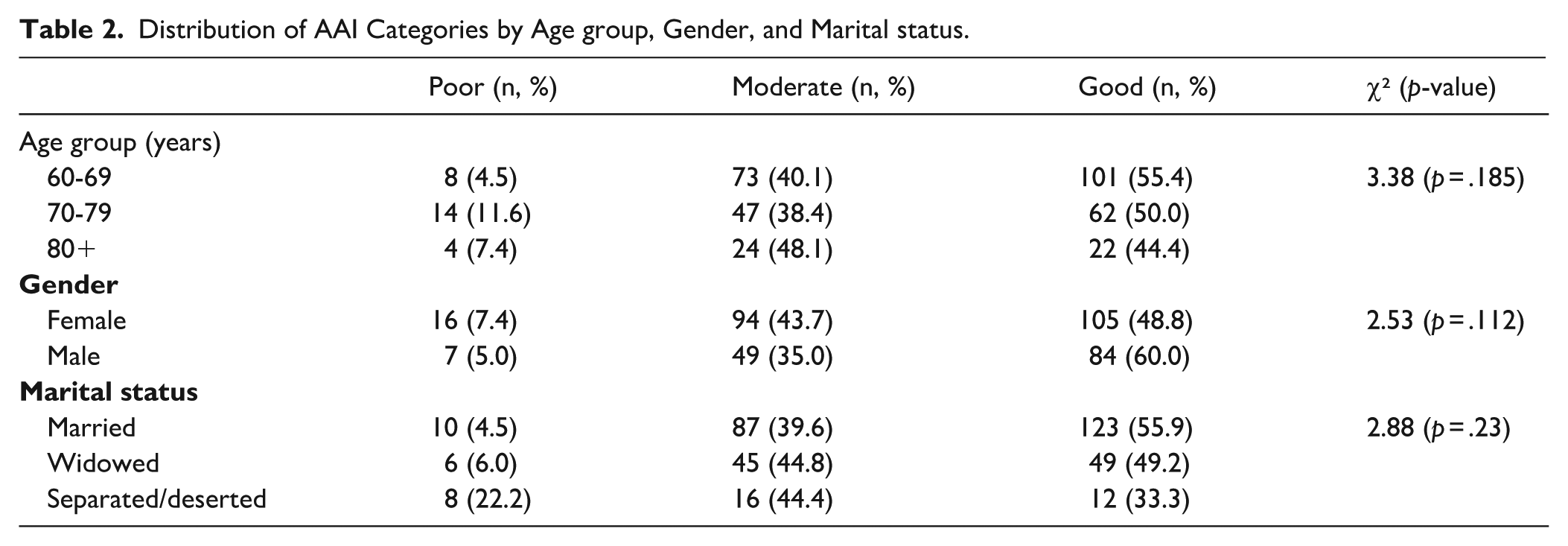
Figure 2 is a stacked bar graph that graphically presents the comparative percentages of Poor, Moderate, and Good AAI across the three age ranges.
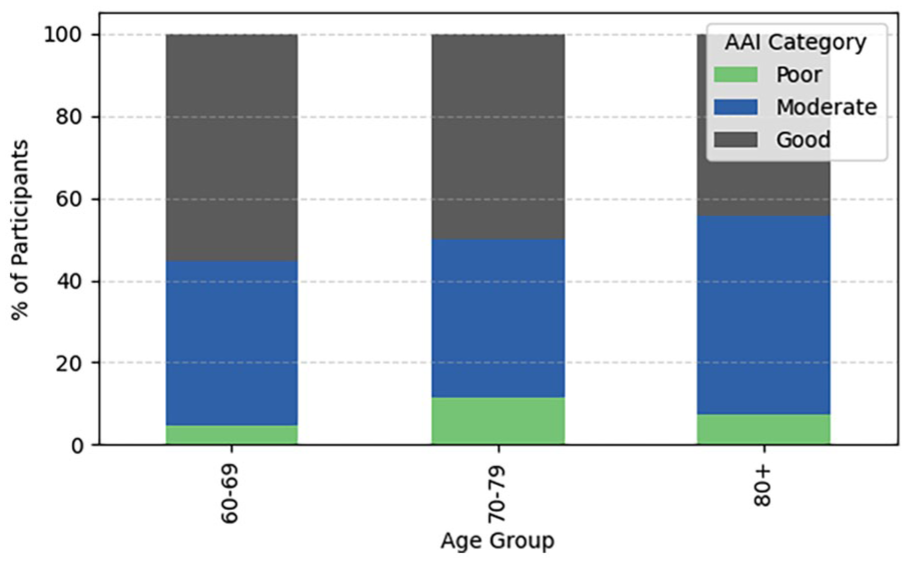
AAI category distribution by age group.
The information indicates a decreasing pattern in the percentage of the elderly with Good AAI with advancing age. For the youngest age group (60-69 years), 55.4% were reported to have Good AAI scores, whereas in the group consisting of participants aged 80 years and older, only 44.4% reached the same. This could point to the fact that with increasing age ranges, other factors like presence of morbidities or ageing process itself led to reduced scores of Active ageing. Moderate AAI category was the most frequent among the oldest participants (48.1%).The greatest prevalence of Poor AAI was seen in the 70 to 79 years age group (11.6%), then 80+ years (7.4%), and lowest in 60 to 69 years (4.5%).
Gender and Active Ageing Index (AAI)
Table 1 shows the proportion of men and women respondents in each AAI category—Poor, Moderate, and Good—drawing attention to possible differences in ageing outcomes.
Figure 3 gives a stacked bar chart that gives a visual comparison of men and women participants according to their distribution by AAI levels.

AAI category distribution by gender.
The analysis shows that 60.0% of men scored a Good AAI, while 48.8% of women did. On the other hand, a greater percentage of women (43.7%) were in the Moderate AAI category than men(35.0%). Also, Poor AAI was somewhat higher among women (7.4%) than men (5.0%).
Education and Active Ageing Index (AAI)
This sub-section examines the effect of education on AAI distribution among rural older adults. As education affects health awareness, social participation, and economic choice, it is crucial in determining active ageing. Table 3 and Figure 4 show the percentage distribution of AAI categories—Poor, Moderate, and Good—according to different levels of education, ranging from illiteracy to education beyond high school.
Distribution of AAI Categories by Education Level.

Chi-square = 3.27, p = .35.

AAI category distribution by education level.
The results indicate a positive correlation between greater educational levels and a greater percentage of individuals in the Good AAI category. For example, 100% of those who were able to read only or had education beyond high school had Good AAI, and 65.4% of high school graduates were also in this group. Compared to illiterate people, they had a more balanced distribution with 44.4% in Moderate AAI and 47.2% in Good AAI, which indicates that having no formal education might lower the chances of achieving the best active ageing outcomes. Respondents who could “Can Read and Write” contributed with the largest proportion in the Moderate AAI group (55.6%), which suggests that limited literacy might bring limited assistance towards realising full active ageing potential (Figure 4).
Marital Status and Active Ageing Index (AAI)
This sub-section investigates the interplay between marital status and active ageing outcomes for older people. Because marital support frequently brings emotional, financial, and social benefits, it can make a considerable difference to the important areas of AAI. Table 2 demonstrates how AAI categories—Poor, Moderate, and Good—are distributed among married, widowed, and separated/deserted individuals.
Highest good AAI ratio (55.9%) occurred in married groups, and for widowed people (49.2%). Poor AAI rate was the maximum (22.2%) and low Good AAI (33.3%) rates were seen for separated or deserted individuals. Good AAI high ratio seems to be supporting higher ageing outcomes that are maintained from stable marital groups. The marital status showed no association with AAI (P = .23)
Occupation and Active Ageing Index (AAI)
This section explores the impact of occupational history—professional, farming, or manual—on active ageing. The type of job may affect financial security, social standing, and retirement benefits, which are important to the AAI domains. Table 4 shows the percentage distribution of AAI categories according to occupational group.
Distribution of AAI Categories by Occupation Type.

Chi-square = 3.1, p = .37.
Respondents from skilled/professional jobs exhibited the highest percentage of Good AAI (65.5%), followed by those from unskilled/caste-based jobs (45.5%). Poor AAI was highest among unskilled workers (12.1%), reflecting possible vulnerabilities. Although trends suggest occupational differences influencing ageing quality, it was not statistically significant.
Social Class and Active Ageing Index (AAI)
This section assesses the relationship between socio-economic status, defined as measured through social class, and the Active Ageing Index (AAI). Wealth affects access to medical care, diet, accommodations, and social security—variables that have a direct effect on the 3 AAI domains: health, participation, and security. Table 5 summarises the percentage distribution of categories of AAI (Poor, Moderate, and Good) by 5 social classes.
Distribution of Active Ageing Index (AAI) Categories by Social Class.
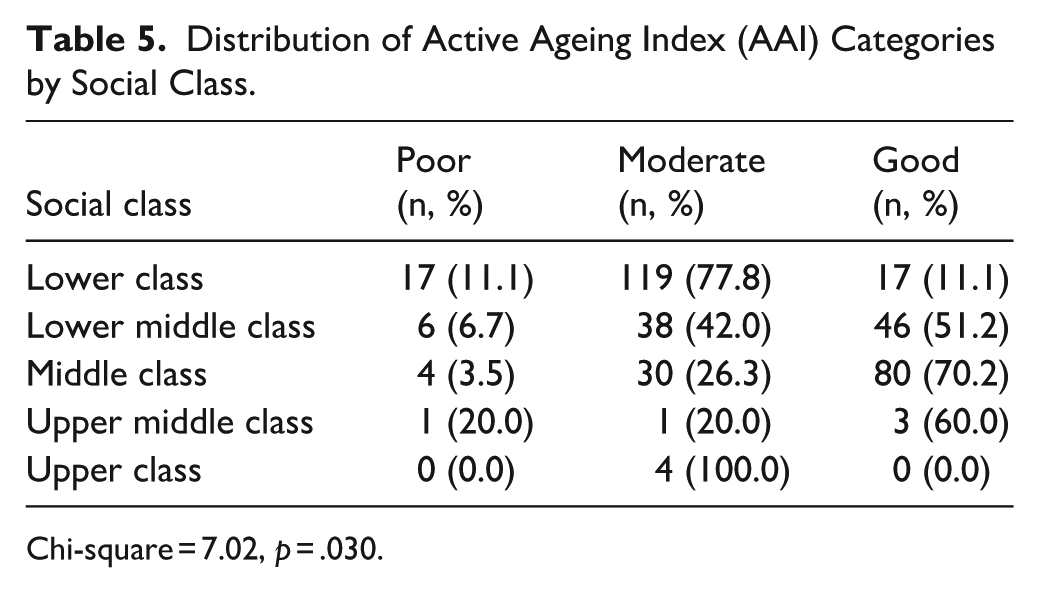
Chi-square = 7.02, p = .030.
It shows that Social class demonstrated the strongest and statistically significant relationship with AAI status (Chi-square p = .0306), separating it from other sociodemographic variables. The Middle Class had the largest proportion of Good AAI (70.2%), followed by the Upper Middle Class (60.0%) and Lower Middle Class (51.2%).
Employment History and Active Ageing Index (AAI)
This section investigates the correlation between working history and Active Ageing Index (AAI) groups. Respondents were divided into 3 groups: currently working, formerly working, and never working. The allocation of AAI groups for each group is provided in the table below.
The results in Table 6 indicate that presently employed older people exhibited a marginally higher percentage of Good AAI (5.4%) than the other groups, and never employed participants had no cases of Good AAI. The majority of Poor AAI cases (55.4%) occurred in the never employed participants. These results indicate that extended workforce detachment could restrict the possibility for healthy and active ageing, presumably as a consequence of decreased financial independence, limited social interaction, and poorer long-term health conditions.
Distribution of AAI Categories by Employment Status.

Chi-square = 4.37, p = .316.
Gender Based Disparities
Table 7 shows that there is a significant difference for the factors sufficiency of income, proportion of persons below poverty Line (BPL), Sources of income, as well as Employment status between the men and women.
Showing Gender Based Differences of Socioeconomic Factors.

Numerical findings (ref Supplemental Tables 2 and 3).
Summary of Statistical Results
This section summarises inferential statistical analyses examining correlations between Active Ageing Index (AAI) categories and sociodemographic variables. Pearson’s Chi-square tested associations between categorical variables (eg, gender, education, and age) and AAI classifications (Poor, Moderate, and Good). Among all parameters, only Social Class showed a statistically significant correlation with AAI (χ² = 7.02, p = .0306), indicating its influence on access to healthcare, lifestyle, and economic status. Age Group (p = .1837), Gender (p = .1127), Education (p = .3548), Marital Status (p = .2300), and Occupation (p = .3761) were not significant, although some descriptive trends suggested higher AAI in younger age groups and men.
Discussion
This section interprets findings in the context of existing literature, highlighting differences in AAI across rural Indian sociodemographic groups. Introduction and Objectives of the Study Sections focus on active ageing assessment and its link to socioeconomic factors, Literature Review Section examines gender differences affecting the security pillar of AAI, and the final part compares prior research with current findings.
Age and Active Ageing
Older individuals, especially those 80+ years, had lower AAI scores, but age group was not statistically significant (p = .1837). This suggests age alone may not predict active ageing in rural areas with limited social safety nets. The presence of vulnerable subgroups underscores the need for targeted policy interventions to improve health access, financial security, and community participation, aligning with Velayutham et al 1 and Medhi et al. 4
Gender and Active Ageing
Although women had slightly lower AAI scores, gender was not statistically significant (p = .1127). Trends suggest that rural women may experience lower active ageing due to gendered constraints, consistent with global findings where gender disparities appear more in income security and employment history.5,6
Education and Active Ageing
Education showed no significant effect on AAI (p = .3548), though those with primary or higher education tended to score better. This may reflect limited rural infrastructure, poor health access, and social dependency, supporting observations by Akila et al 9 and Guntupalli and Chakraborty. 12
Social Class and Active Ageing
Social Class was significantly associated with AAI (p = .0306). Higher social strata performed better across all domains, indicating that resource access and economic prosperity strongly influence active ageing. Other variables showed trends but were not significant, contrasting with Western studies where education and health behaviours are stronger predictors.10,11
Employment and Active Ageing
Current employment correlated with higher AAI scores, though not statistically significant. Never-employed individuals, especially women, had the lowest scores, supporting the view that economic activity enhances autonomy and social participation.8,16 Gendered employment patterns persisted; older women, particularly 70+ years, were less likely to have participated in formal work.17,23
Socioeconomic Gender Disparities
Income sufficiency (χ² = 12.49, p = .002), pension sources (χ² = 18.33, p < .001), and BPL status (χ² = 4.51, p = .034) disproportionately affected women. Financial insecurity due to interrupted work and widowhood limited participation and healthcare, undermining the WHO “security” pillar.7,20 Women also had lower land ownership (24.2% vs 17.1% men, p = .25), reflecting structural inheritance issues.20,21 Marital and employment disparities further affected women: 63.3% were widowed/divorced versus 20.7% men, while men had higher employment probabilities across all ages.9,38 Consequently, men had more stable income and financial security despite the feminisation of ageing phenomenon.
Linking Gender based Disparities to Active Ageing
Although gender itself was not a significant predictor of AAI category, the underlying disparities in income, employment, and access to pensions reveal systemic inequities that cumulatively hinder active ageing for women. Although women are often respected culturally, they face systemic economic marginalisation. Societal attitudes and intra-household power dynamics reduce their agency, especially in claiming land rights or negotiating fair wages.24,40
Many older women are physically and mentally capable of contributing to the workforce, but social expectations continue to confine them to caregiving and household tasks. This contributes to feminised poverty in old age—a global phenomenon not limited to India. Even in high-income countries such as Germany, older women are more likely than men to face income insecurity due to lower lifetime earnings, interrupted careers, and gendered care responsibilities.24,39,40 This supports the argument made by Zaidi et al 6 that gender-neutral ageing policies fail to address the compounded disadvantages women experience over the life course.
In sum, while age, gender, and education showed weak statistical links to AAI, economic, and social disparities—particularly for women—emerged as significant barriers to healthy and active ageing in rural Karnataka. This reinforces the WHO’s call for policy strategies that integrate gender and equity into ageing interventions.
Alignment With Previous Literature
In contrast with previous research focussing on a solitary domain (eg, disability, health status, or participation in isolation) or undertaking macro-level analyses failing to adapt structures to local rural contexts, the present research applies a context-based AAI model. It uses a composite indicator based on the WHO framework and establishes it via field-level validation in rural Karnataka.
As opposed to conceptual criticisms by Guntupalli and Chakraborty 12 or broad health-based evaluations by Medhi et al, 4 this research combines the 3 AAI domains with quantifiable indicators appropriate for rural areas. Additionally, although global models such as that of Bosch-Farré et al 11 and Haque et al 10 are very informative, they are not localised for India’s socio-economic variability. Table 8 provides a formal comparison between the current study and prominent previous works.
Comparison with Previous Literature on Active Ageing.

Theoretical and Practical Implications
With comparison with present Indian elderly policies,41 -43 theoretically, the research attests the applicability of the multidimensional AAI approach in a non-Western rural environment. In practical terms, the findings of the research lend support to specific policy design—specifically highlighting economic interventions such as pension programmes, financial education, and rural asset development as drivers of active ageing improvement. The study shows a large percentage of the elderly with Good AAI—despite infrastructural limitations—indicating factors of resilience that need more intense investigation, such as intergenerational care, cultural traditions, and community engagement in rural India.
These results also highlight the practical benefits of continuation of employment approaches into ageing policy strategies. Facilitating flexible models of employment for older people—especially in rural areas—may improve functional health and socioeconomic participation, with improved AAI results.
Strengths and Limitations
Strengths
This study calculated the Active Ageing Index (AAI) for a rural microcosm population, adapting the framework used by S. B. Nair—who had previously applied it among a Scheduled Tribe group. Instead of relying solely on the standardised UNECE model, which is challenging to implement in India due to limited healthcare infrastructure, rural-urban disparities in access, and minimal employment opportunities for older adults, our approach used contextually relevant components that better capture the realities of ageing in rural India.
By incorporating multiple dimensions—including income sufficiency, land ownership, and marital status—the study provides a comprehensive and multidimensional assessment of active ageing in this population.
The secondary analysis of gender-based differences in socioeconomic factors—particularly those shaping the security component of the AAI—offered deeper insights into how elderly women experience structural disadvantages in areas such as pension access, land ownership, and financial sufficiency. This strengthens the study by showing how gendered experiences intersect with active ageing and by identifying pathways for more equitable ageing policies.
Limitations
Although the study holds important results, the study has a number of limitations that need to be considered:
Cross-sectional data were used in the study, which limits the capacity to draw causal inference across time.
The data were obtained from a single district, which restricts the generalisability of the results to rural or urban districts.
Some potentially affecting variables like digital literacy have not been incorporated in the analysis.
The analysis was based on self-reported health and socioeconomic data, which can cause recall or social desirability bias.
The study does not include a longitudinal design, which would be more appropriate to monitor changes in active ageing over time.
Implications for Future Research
Subsequent studies may extend the localised AAI framework to other Indian states, add longitudinal designs to monitor ageing transitions, and incorporate qualitative methodologies for better capturing intangible aspects such as emotional well-being or subjective social value. Rural-urban comparisons of elderly populations might add further richness to the knowledge of ageing in India. Further research should focus on the long-term monitoring of active ageing indicators and their potential application as practical tools for policy formulation and intervention
Conclusion and Recommendations
This research aim was to measure the levels of Active Ageing Index (AAI) among rural older people and explore its association with sociodemographic variables. Using a cross-sectional analysis on a sample of 355 rural older people within Study area District, these research aims were well realised. The results showed that 53.5% of the participants demonstrated Good AAI, confirming the presence of active ageing indicators among a conventionally underserved group. Notably, Social class was the only statistically significant predictor of AAI (P = .0306). Whereas variables like age, gender, education, marital status, and occupation exhibited directional trends but not statistical significance, the study filled an important gap by operationalising and validating a localised, multidimensional AAI model specific to rural India, thereby filling a lacuna in the literature that tended to be based on piecemeal or urban-biased data. In so doing, the research not only consolidates the theoretical framework of rural ageing in India but also presents actionable empirical baseline data to inform social policy on elderly welfare.
In general, this study provides a significant, evidence-based basis for inclusive geriatric policy formulation and establishes the practicability of measuring and facilitating active ageing in rural India.
In addition, other results from the descriptive analysis reveal that active ageing is shaped by work status. Similarly, presently employed older persons had higher proportions in the Good AAI category than never-employed persons.
While resource availability is not always the primary barrier, gender disparities in India are deeply entrenched in longstanding cultural traditions and social norms. These traditions, though not inherently negative, often assign women a secondary economic role within the household. From an early age, women are encouraged to value domestic responsibilities over economic independence, which limits their awareness of their legal rights and entitlements, particularly regarding land ownership, labour force participation, and social security access.
To promote equity, policy measures must go beyond provision and address empowerment through awareness-building. Women must be educated about their rights and provided with accessible channels to exercise them. The Active Ageing Index is linked to social class, and this study highlights the need for more research on how gender influences active ageing. Women generally live longer but face greater financial and employment challenges in later life. Equal access to men and women in older age of especially the awareness of these economic realities and then .
The following recommendations are suggested to further improve active ageing outcomes in comparable rural settings:
Given that social class, as measured by the Udai Pareekh scale, influences active ageing through education, social networks, and household resources, policy interventions should leverage this dimension to improve ageing outcomes. Awareness programmes on health based government schemes, legal rights, and microcredit initiatives should be tailored to reach lower-class elders, who are often less informed and socially isolated. Village-level interventions, such as community centres, mobile service units, and inclusive Self-Help Group models, can provide both men and women with access to financial support, health services, and social participation opportunities. By targeting awareness and access according to social class, policymakers can ensure that vulnerable elderly populations are empowered to engage fully in Health, Participation, and Security domains, thereby promoting equitable and sustainable active ageing. Monitoring these efforts would not only advance research on the factors shaping gender-based differences in active ageing but also provide evidence to guide more equitable policy interventions.
Elderly women in rural areas often experience compounded disadvantages, including limited economic independence, lower ownership of assets, and reduced access to social security programmes. Whether these facts have an effect on the ageing index can only be ensured when we address these disparities with targeted awareness programmes. These should be implemented specifically for women aged 60 years and above, focussing on legal rights, inheritance, pensions, and social protection schemes. These programmes can be facilitated by dedicated volunteers or community workers, distinct from existing healthcare or SHG activities, and may include incentives to ensure sustained engagement.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251380672 – Supplemental material for Beyond Chronological Age: Active Ageing Index, Social Class, and Economic Realities of Rural Karnataka, India
Supplemental material, sj-docx-1-jpc-10.1177_21501319251380672 for Beyond Chronological Age: Active Ageing Index, Social Class, and Economic Realities of Rural Karnataka, India by Archana Mandal and Mangala Subramanian in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
I would like to thank the Head of Department and the faculty of Community Medicine of Vydehi Institute of Medical sciences, Dr. Maria Archana, Dr. Hugar Siddalingappa, and Mr. Harikrishna Goud for their valuable contributions.
Ethical Considerations
The ethical approval for the study was obtained from the Institutional Ethics Committee (IEC number ECR/747/Inst/KA/2015/RR-18).
Consent to Participate
Written informed consent was obtained, and the anonymity of participants was maintained throughout the study period.
Author Contributions
Dr. Archana Mandal: Conceptualisation, Formal Analysis, Data Curation, and Writing (Draft and Original). Dr. Mangala Subramanian: Conceptualisation, Methodology, Project administration, Resources, Writing (Review), and Supervision. The views expressed in the submitted article belong to the authors and not an official position of the institution. The manuscript has been read and approved by all the authors. The requirements for authorship have been met, and each author believes that the manuscript represents honest work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.