
Abstract
Introduction/Objectives:
The decline in preventive healthcare utilization observed during the COVID-19 pandemic has led to substantial adverse health effects. This quality improvement intervention aimed to alleviate these impacts by implementing a proactive, Automated Patient-Prompting Preventive Services Scheduling and Reminder System (APPPSSRS) coupled with provider-facing education on APPPSSRS and clinical decision tools to improve uptake of preventive care in a Southwest US primary care clinic.
Methods:
Translation of evidence into practice in the development and implementation of the APPPSSRS and provider intervention was guided by the Knowledge-to-Action (K2A) Framework, with continuous feedback between the clinical team and the study leads. Scheduled and cancelled appointments among adults were compared pre-intervention (n = 1860), when the clinic relied on ad hoc and reactive scheduling after missed preventive care, and post-intervention (n = 1900), following implementation of the APPPSSRS: a survey assessed provider adherence and confidence in the decision tools that supported preventive care uptake. Descriptive statistics and chi-square tests were used to analyze outcomes.
Results:
Post-intervention data revealed a small, non-significant increase in preventive care appointment scheduling. However, there was a significant rise in appointment cancellations with patients using the APPPSSRS (χ²(df = 1) = 41.81, P < .001). Cancellations were particularly high among Black and publicly insured patients. Staff reports suggested that many cancellations were due to insurance and other policy changes linked to the end of the Public Health Emergency (PHE). Providers reported high adherence to and confidence in decision support tools.
Conclusions:
The implementation of a proactive APPPSSRS did not yield a significant increase in the uptake of preventive care and was associated with significantly higher cancellation rates, likely in part due to policy changes related to the end of the PHE. Provider education enhanced the use of preventive care supportive clinical decision- making tools. Integrated, multi-modal strategies, including electronic prompting, enhanced self-scheduling tools, and provider education, may need to be combined with structural supports to ensure uptake of preventive services in the post-pandemic landscape.
Keywords
Introduction
COVID-19-Related Health Debt
The COVID-19 pandemic led to an 86% global drop in healthcare utilization, further exacerbating disparities and limiting access to essential services such as vaccinations, preventive screenings, 1 and significant reductions in outpatient visits.2,3 In 2020, the COVID-19 pandemic profoundly impacted the US healthcare system, forcing patients to navigate complex decisions about when and how to resume preventive care services. Many patients faced a dilemma, balancing the risks of leaving their homes with the benefits of routine screenings.4,5
Martin et al 6 reported significant declines in overall healthcare visits, leading to office closures, reduced services, and accumulating “health debt.” 7 Health debt is the cumulative adverse effects of postponed or missed healthcare services. During the pandemic, patients often delayed or skipped preventive screenings, disease management, and chronic care, which can result in worsened health outcomes over time. 7 These behavioral shifts, spurred by the pandemic, undermined gains in chronic disease prevention and early detection, and led to higher morbidity and mortality rates and increased long-term healthcare costs.7,8
The Impact of Health Debt on Health Inequities
The pandemic altered healthcare delivery and access nationwide and led to deepening inequities both in higher rates of mortality among racialized minorities and in preventive care.8,9 A 2020 survey of adults aged 18 years and older found that 40.9% avoided medical care due to fears of COVID-19, with 12.0% avoiding urgent care and 31.5% skipping routine services. 10 Despite the availability of COVID-19 vaccines by December 2020, the pandemic’s impact on preventive care services in the US persisted. 11 Routine healthcare delivery was disrupted, and service uptake remained low,12,13 resulting in dramatic declines in cancer screenings and delayed diagnoses13,14 These changes were especially pronounced in historically underserved groups. 4 Efforts to restore preventive services included virtual care and reopening measures, but pre-pandemic levels of service utilization were slow to return. 15
Approaches to Increase the Uptake of Preventive Services
Quality healthcare involves treating illnesses and providing preventive care to prevent future health complications. 16 Preventive healthcare is crucial in improving population health and addressing health disparities. 16 A comprehensive literature review highlighted the effectiveness of automation in improving appointment scheduling and patient retention.17 -19 Traditional reminder systems are used to notify patients of appointments that have already been scheduled. These reminders are often sent shortly before the appointment, reinforcing a commitment the patient made. This model is effective for ensuring appointment attendance because it builds on a prior decision to seek care.17 -19 However, evidence suggests that personalized and well-timed reminders to schedule preventive care can positively influence health behaviors even when appointments have not yet been made.17 -19 In addition to improving patient adherence to preventive care guidelines, such reminders to prompt patients to schedule appointments have the potential to increase clinic efficiency by reducing staff workload related to scheduling and follow-up.17 -19 This approach may also promote more equitable access to preventive care by reaching patients across different demographics, including those who might otherwise delay or miss services. As such, proactive prompting coupled with scheduling opportunities offers a scalable strategy to reduce disparities in preventive health care access across race, gender, and socioeconomic status. 20
Local Context
Texas, which had the second-highest number of COVID-19 cases in the US, experienced poor health outcomes due to pre-existing healthcare disparities. Minority groups, mainly Hispanic and African American communities, were disproportionately affected. 21 Hispanic Americans represented nearly 40% of cases and 56% of deaths, while African Americans accounted for 16% of cases and 11% of deaths. 21 Additionally, socially vulnerable Texans experienced elevated COVID-19 mortality rates. 22
At the project site, a family care clinic serving approximately 6000 patients annually in southwest Texas, preventive care visits among individuals aged 16 years and older declined by 75% to 85% between 2020 and 2022. This sharp decrease was primarily attributed to concerns related to COVID-19, insurance loss, and socioeconomic barriers such as housing instability. These trends mirrored national patterns and underscored the ongoing challenge of restoring preventive care utilization, prompting the need for quality improvement efforts.
Although substantial evidence supports proactive approaches for appointment scheduling to improve preventive care uptake, the clinic previously scheduled preventive visits in an ad hoc manner, typically when patients presented for other chronic or acute appointments, or through manual staff outreach once patients became overdue. This quality improvement (QI) project aimed to address the resulting health debt from missed preventive care by introducing an evidence-based, proactive patient-facing scheduling system, as well as a health maintenance dashboard, and a clinical decision support tool for providers that supports preventive care. Drawing on best practice evidence, an APPPSSRS was designed to prompt patients to schedule their appointment by delivering personalized and timely messages to patients a few weeks before they were due for preventive care. By prompting patients before they missed care and giving them agency to act, APPPSSRS aimed to foster a proactive, timelier, and more self-directed adherence to preventive care recommendations compared with the previous reactive approach.
The objectives of the QI initiative were to (1) enhance the scheduling and tracking of preventive services; (2) evaluate the feasibility and impact of patient self-scheduling, and transition the clinic’s approach from reactive to proactive care by empowering patients to initiate preventive appointments in line with evidence-based guidelines; and (3) facilitate provider uptake of clinical decision tools that support preventive care uptake.
Methods
An integrative literature review conducted identified evidence-based strategies to enhance patient engagement through APPPSSRS.17 -19 The implementation of the project employed the Knowledge-to-Action (K2A) Framework, which guides each step from knowledge translation to tailored implementation, stakeholder engagement, and long-term integration into clinical practice. 23 This framework entailed continuous feedback between the clinical implementation team and the project leads.
Design
The QI project utilized a pre-/post-intervention design at a single outpatient clinic in the Southwestern US.
Setting
The project was conducted at a comprehensive outpatient family practice owned by a Nurse Practitioner. The clinic provided acute, urgent care, and preventive screenings, including physical exams and chronic care management. The clinical team consisted of 2 nurse practitioners, supported by medical assistants, an office manager, and a medical receptionist, serving approximately 6000 patients annually.
Sample, Inclusion, and Exclusion Criteria
The patient sample consisted of adults aged 16 years and older who had missed 1 or more guideline-based preventive screenings recommended by the US Preventive Services Task Force (USPSTF) 24 in the past year. Exclusion criteria included patients younger than 16 years or older than 80 years, those who had completed screenings within the past year, patients with terminal illnesses, those without mobile phone access, and individuals receiving care exclusively via telemedicine or with cognitive impairments. The provider sample included all 6 clinical and support staff involved in the intervention.
Intervention, Data Collection, and Instruments
Patient-Facing Intervention
A structured text reminder with preventive screening information was sent to each eligible patient in September 2023 through the project’s site EMR system with a link to opt out of future reminders. The message urged patients to schedule their overdue screenings and allowed them to request appointments electronically. These messages included a clear call to action and offered multiple scheduling options, such as through the patient portal or by text messages to the clinic. Patients were also able to use the APPPSSRS system for acute or chronic disease management appointment scheduling, if desired. A designated staff member processed these requests. Education was provided to the provider team and staff on using decision support and health maintenance dashboards to create and monitor preventive screening and wellness appointment reminders post-intervention (see below).
Retrospective chart reviews were used to collect demographic patient data and track preventive screening adherence. Pre- and post-intervention adherence rates were compared using the International Classification of Diseases (ICD-10) 25 and Current Procedural Terminology (CPT) 26 codes billed. Additionally, post-intervention data collection involved assessing the use of the self-scheduling system.
Provider Intervention
Structured in-service training sessions were held to enhance provider engagement with the health maintenance dashboard and the integrated clinical decision support tools. These sessions were designed to help providers effectively access, interpret, and act on the information presented in the dashboard. Particular attention was given to identifying patients overdue for preventive services and appropriately engaging those who had used the system to schedule their appointments.
In addition to these formal trainings, providers participated in interactive electronic health record walkthroughs and live demonstrations during regularly scheduled staff meetings, guiding providers through real-time navigation of the decision support tools and dashboard filters to promote practical understanding and integration into daily workflows.
To support ongoing adoption and accountability, audit and feedback reports were shared with providers at regular intervals. These reports highlighted individual and team-level usage of the dashboard and the corresponding rates of completed preventive services. The feedback served to reinforce provider performance, encourage consistent tool utilization, and promote a culture of continuous improvement in preventive care delivery.
A 2-item questionnaire using a Likert scale was used to evaluate the impact of provider and staff education on self-reported adherence to and confidence in using the clinical decision tool (Appendix A).
Data Analysis and Management
Data were analyzed using SPSS version 29. Descriptive statistics and chi-square tests were used to examine demographic characteristics of the patient sample and to evaluate the prevalence of preventive care appointment scheduling and cancellation pre- and post-intervention. Descriptive statistics were used to examine the use of the electronic system for acute care scheduling post-implementation and provider adherence to the decision-support tools. All data were de-identified and stored securely on OneDrive, accessible only to the study team. Ethical approval was obtained from (the corresponding author’s institution’s – Johns Hopkins University School of Nursing) Project Ethical Review Committee.
Results
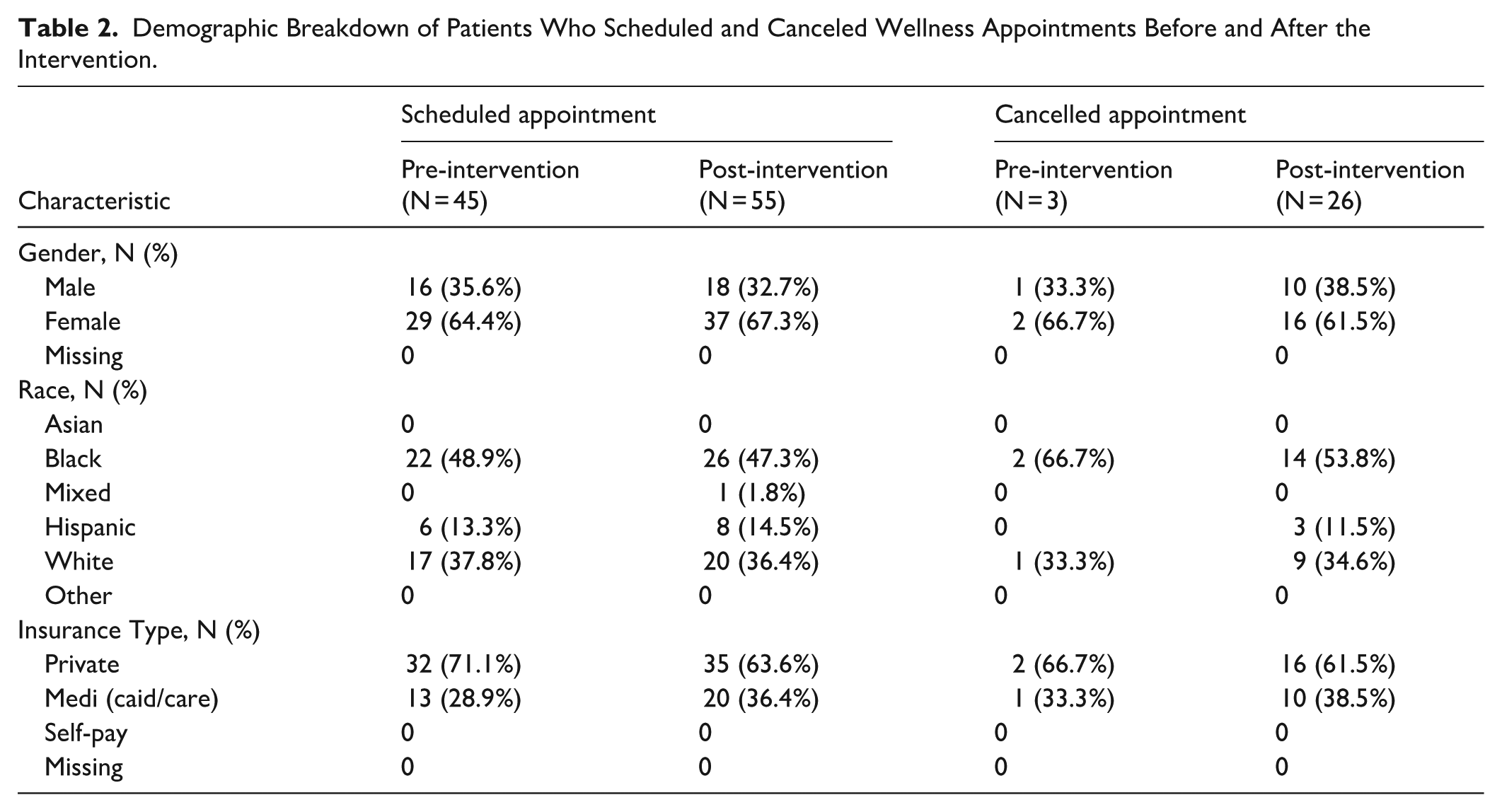
The pre- and post-intervention demographic characteristics of the sample were similar by gender, race, and insurance type (Table 1). Of 1860 eligible patients who missed recommended screening, 1749 received automated reminders for annual wellness examinations with self-scheduling options, with a bounce rate of 111 messages. The percentage of patients who scheduled preventive appointments was slightly higher post-intervention, 2.89%, compared to 2.42% pre-intervention, but this was not statistically significant (χ2(df = 1) = 0.82, P = .37). The demographic characteristics of those who scheduled appointments were similar by gender and race (Table 2). However, there was an increase in the proportion of patients who scheduled appointments who were government-insured (Medicare and Medicaid) patients from 28.9% (n = 13/45) to 36.4% (n = 20/55).
Demographic Characteristics of the Sample.

Demographic Breakdown of Patients Who Scheduled and Canceled Wellness Appointments Before and After the Intervention.
Following the implementation of the APPPSSRS, the cancellation rate, which includes both no-shows and cancellations for preventive appointments, increased significantly compared to baseline. In fall 2022, using the practice’s traditional method of scheduling, the cancellation rate was 6.67%. This rose to 47.28% in fall 2023 after the intervention (χ²(df = 1) = 41.81, P < .001).
Due to the low number of cancellations pre-intervention, formal comparison of pre-post-cancellation rates by demographic characteristics was not possible. Post-intervention, female patients had a lower cancellation rate of 43.2% (n = 16 of 37 scheduled) compared to male patients, whose rate was 55.6% (n = 10 of 18 scheduled; Figure 1). Among racial groups, Black patients had a higher cancellation rate of 53.8% (n = 14 of 26 scheduled) compared to White patients at 45% (n = 9 of 20 scheduled; Figure 2). When compared by insurance type, privately insured patients had a lower cancellation rate of 45.7% (n = 16 of 35 scheduled), while patients with Medicaid or Medicare had a higher rate of 50% (n = 10 of 20 scheduled; Figure 3). Notably, among Black patients with Medicaid or Medicare, the cancellation rate was highest at 60% (n = 6 of 10).

Appointment cancellation by gender post-intervention.

Appointment cancellation by race post-intervention.

Appointment cancellation by insurance type post-intervention.
During weekly meetings with the clinic staff, staff reported that in their conversations with patients, they frequently mentioned challenges related to disenrollment from insurance due to policy changes resulting from the end of the Public Health Emergency (PHE). Privately insured individuals also reported to staff that they faced new challenges due to the end of work-from-home policies that limited flexibility for appointments.
Additionally, as a secondary patient outcome, thirty-one (5.5%; n = 31/563) of patients opted to utilize the system during the intervention period, representing an increase from a baseline of 0%, as the APPPSSRS was not in place before the intervention.
Provider adherence to the decision support tools was high, with 100% (n = 6) acknowledging improvement and 83.3% (n = 5) expressing confidence, while 16.7% (n = 1) remained neutral due to concerns about workflow disruption from technology integrations.
Discussion
The COVID-19 pandemic significantly reduced preventive care visits across the United States, highlighting the need for effective interventions to re-engage patients with healthcare services.2,3 Building on evidence for automated prompting approaches to engage patients in preventive care, this quality improvement (QI) project was developed to examine the impact of an APPPSSRS on preventive care uptake and provider compliance with decision support tools that support preventive care in a primary care practice.
In contrast to previous work,17 -19 our study found that automated reminders to prompt preventive care scheduling alone did not result in a significant increase in the patient-initiated scheduling of preventive appointments. Additionally, after the implementation of the APPPSSRS system, the practice experienced a substantial rise in appointment cancellations, particularly among Black patients and those with government insurance. For the provider-facing intervention, the project demonstrated that provider education contributed to improved adherence to and greater confidence in using decision support tools and health maintenance dashboards that supported preventive care uptake.
This quality improvement (QI) initiative was conducted during a significant change in federal healthcare policy. The Affordable Care Act (ACA) of 2010 increased access to preventive care by mandating coverage for preventive services without additional costs to patients. 27 During the COVID-19 pandemic, the federal Public Health Emergency (PHE) declaration expanded access through temporary exemptions, including continuous Medicaid coverage for low-income individuals. However, the expiration of the PHE in May 2023 ended these exemptions, resulting in disruptions in care access, especially for Medicaid enrollees. 28 Although patient reasons for appointment cancellations were not formally collected for this study, during regular meetings with clinic staff in the implementation phase of the intervention, staff reported conversations with patients indicate that many of the cancellations were linked to disruptions in Medicaid coverage following the expiration of the PHE. These findings suggest persistent barriers tied to social determinants of health that disproportionately affect underserved populations.
A national survey by the Kaiser Family Foundation (KFF) found that nearly one-fourth of adults disenrolled from Medicaid since early 2023 remain uninsured, and approximately one-fifth of previously enrolled individuals reported being disenrolled in the past year. 29 These disenrollment rates created significant barriers to care that this initiative sought to address and may have been responsible for the higher rate of cancellations among those with government insurance. In response to federal policy changes, the clinic staff reported that they actively supported Medicaid patients through the re-enrollment process to help restore access to care. However, our study findings indicate that while such advocacy was helpful, it was insufficient to counteract the broader challenges caused by these systemic disruptions. This is also likely to have implications for health equity, since Medicaid unwinding disproportionately affected racial and ethnic minorities. 30 At the project site, the prevalence of cancellations was higher among Black patients than among white patients. Specifically, Black patients with Medicaid or Medicare insurance had a cancellation rate of 60% (n = 6/10), indicating a notable disparity.
Privately insured patients also had a high, albeit comparatively lower, cancellation rate. Many of these patients also cited difficulties in securing time off work due to reduced schedule flexibility and increased in-person work requirements following the end of remote work policies that were more common during the pandemic. Therefore, the changing policy environment at the end of the PHE affected some of these patients as well, albeit somewhat less so based on lower cancellation rates.
Implications for Practice
This QI initiative emphasizes the need for healthcare practices to adopt more comprehensive, patient-centered, and culturally responsive strategies. Automated prompts to schedule appointments may facilitate initial outreach, but their impact is limited without additional support mechanisms. To effectively improve follow-through, practices should implement integrative approaches such as community engagement, patient navigation programs that address broader structural barriers to appointment attendance, and health education tailored to the needs of high-risk groups.31,32 Furthermore, improving provider engagement with clinical decision-support tools also remains important. While providers may appreciate their utility, concerns over workflow integration may affect adherence, highlighting the importance of offering robust training, continuous technical support, and workflow adaptations to enable providers to use these tools effectively.33,34 To support sustainability, future clinical practices must prioritize system functionality, routine maintenance, and real-time troubleshooting to reduce disruptions in patient care. 35
Implications for Policy
This project underscores the critical influence of healthcare policy on service access, especially for vulnerable populations. The end of the PHE and its temporary protections led to increased Medicaid disenrollment and gaps in care continuity. 36 Policymakers must consider the unintended consequences of policy transitions and ensure safeguards are in place to prevent loss of coverage during systemic changes. Expansion of patient re-enrollment assistance programs, extended coverage grace periods, and public awareness campaigns may mitigate these impacts and support uninterrupted access to preventive services. 37 Policies should also account for structural barriers that limit healthcare utilization for marginalized communities. 38
Implications for Research
Future research should explore multi-component interventions that combine automated reminders with targeted patient support strategies, such as community-based outreach and incentive programs.39 -41 A promising intervention includes incentivizing healthy behaviors among health plan enrollees, such as smoking cessation, weight management, timely immunizations, and prenatal care, to improve health outcomes, enhance prevention efforts, and lower program costs. 41 Research should also evaluate the impact of digital health technologies across diverse populations to determine which features enhance uptake and adherence. 42
Additionally, more work is needed to investigate how healthcare delivery and access can be improved during public health emergencies, particularly for vulnerable populations, to inform future policy decisions promoting health equity, as more pandemics are likely in the future. Studies examining how policy shifts, such as the rollback of public health emergency measures, affect healthcare engagement at the patient level would inform more responsive and equitable health system designs. Lastly, research into implementation science can offer insight into optimizing clinical decision support tool integration within real-world workflows.
Strengths and Limitations
This project used a multi-faceted strategy to improve preventive care, combining patient engagement technology with provider support tools. The integration of health maintenance dashboards, decision support systems, and automated prompting to schedule appointments enhanced both provider compliance and patient access. Notably, 5.5% of patients used the APPPSSRS to schedule preventive appointments, showing early signs of increased patient autonomy. Stratification by race and insurance status revealed disparities in cancellation rates, particularly among Black and Medicaid-insured patients, offering a deeper understanding of equity challenges. Informal reporting of patient-reported reasons for cancellations provided insight into barriers such as loss of insurance or work-related scheduling conflicts. Provider education led to improved use of decision support tools that supported preventive care, and full staff participation enhanced the consistency of implementation.
However, the limited uptake of the system among patients reduces generalizability, and the high rate of cancellations post-intervention raises questions about patient readiness and barriers to follow-through. The system lacked granular behavioral data, such as digital literacy or language barriers, and a systematic collection of reasons for cancellations, which could have guided more targeted outreach. Provider behavior may have been temporarily influenced by awareness of being observed, and the short duration of follow-up limits conclusions about sustained change. External factors, such as policy shifts following the PHE, also likely impacted care access.
Conclusion
This study highlights the complexities of improving preventive care after the COVID-19 pandemic. While automated reminders offer a promising tool to encourage patient engagement, they must be complemented by multimodal interventions that address the underlying barriers to care. As healthcare systems recover from the pandemic’s impact, future efforts should focus on policy reform, provider education, and developing integrative, patient-centered care models that promote preventive health for all.
Footnotes
Appendix A
Provider and Staff Survey – Post Intervention The following Likert-scale survey was administered to assess provider and staff perceptions following the educational intervention:
Acknowledgements
The authors thank the staff and patients of Treat Now Family Clinic for their participation in and support of this quality improvement initiative.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.