
Abstract
Loneliness is considered a critical global public health issue, with its prevalence rising across regions and populations, adversely affecting quality of life among older adults. This quasi-experimental design aimed to determine the effects of Together We Thrive, a culturally adapted, group-based psychosocial program on loneliness, social connection, depression, cognitive function, and quality of life among older adults in Northern Thailand. Fifty participants were randomly assigned to either the experimental group (n = 25) or the control group (n = 25). The experimental group received the 12-week closed-group Together We Thrive program (fixed membership to foster group dynamics) with culturally relevant activities (arts and crafts, folk dance, writing, and storytelling) in groups of eight or nine older adults with two facilitators. The control group attended a one-day educational program. The intervention was refined based on feedback from older adults experiencing loneliness to ensure contextual relevance and acceptability. The cultural adaptation process was further strengthened by active involvement of these older adults. Outcome measures included the 6-item Revised UCLA Loneliness Scale, the Lubben Social Network Scale, the Geriatric Depression Scale—Short Form, the Cognitive Failures Questionnaire, and the WHOQOL-BREF. Assessments were conducted at 3 time points: baseline, post-intervention (12 weeks), and follow-up (24 weeks). Repeated-measures ANOVA revealed significant interaction effects for loneliness (P = .037, η² = .104), social networks (P = .031, η² = .109), and quality of life (P = .026, η² = .114), favoring the experimental group. No significant changes were observed in depression or cognitive function. Results indicated that the program effectively strengthened social connections, reduced loneliness, and improved quality of life among older adults experiencing loneliness.
Keywords
Introduction
Loneliness has emerged as a critical global public health issue, with its prevalence rising across regions and populations. 1 According to the U.S. Department of Health and Human Services (2023), loneliness often goes unrecognized and untreated despite its serious impact. 2 Older adults may be reluctant to seek help due to stigma, embarrassment, or feelings of shame. 3 Among this population, loneliness is particularly common and distressing, with well-established links to physical decline, cognitive impairment, mental health problems such as depression, and all-cause mortality—factors that collectively diminish overall quality of life. 4 Loneliness is defined as a subjective feeling of distress arising from the perceived discrepancy between desired and actual social relationships. 5 Although loneliness can be transient and affect individuals of all ages, adults over the age of 60 years are especially vulnerable to persistent and multifaceted consequences of loneliness. 6 Contributing factors include physical limitations, chronic illnesses, retirement, and family migration. 7
In Thailand, loneliness among older adults is an urgent public health concern, with a national survey reporting that 30.3% experience severe loneliness and 12% live alone8,9; in contrast, one province in Northern Thailand shows disproportionately higher vulnerabilities, with 27.3% of older adults living alone, 22.3% reporting chronic illnesses, and 39.6% diagnosed with depression. 10 These overlapping vulnerabilities underscore the need for targeted psychosocial interventions tailored to this regional context.
One well-established example is a Finnish group-based psychosocial intervention that incorporated guided discussions, reminiscence activities, and collaborative engagement. 11 This intervention significantly improved loneliness, mood, and perceived social support among participants. 11 Notably, the program emphasized the intentional cultivation of positive group dynamics to foster psychosocial growth, mutual support, and meaningful social reconnection. However, such interventions are shaped by cultural contexts. Norms, values, and daily life routines influence how loneliness is experienced and addressed, limiting the direct applicability of foreign-developed models in other cultural settings. 12
The local healthcare organizations in Thailand have implemented initiatives—including senior clubs, recreational therapy, and volunteer home visits—to address loneliness among older adults13 -15; however, most of these increase the quantity of contact rather than the emotional depth and group cohesion required for lasting connection. Moreover, few programs in Thailand are culturally adapted or assess broader health outcomes, such as cognitive function and quality of life. Evidence shows interventions are most effective when they cultivate positive group dynamics (mutual trust, empathy, and belonging) and engage 4 core mechanisms: enhancing social skills, increasing social support, creating opportunities for interaction, and addressing maladaptive social cognition.11,16 The previously mentioned Finnish group-based psychosocial program exemplifies this approach, using guided discussion, reminiscence, and collaborative tasks to improve loneliness, mood, and perceived social support while intentionally nurturing group processes. 11 Yet because norms, values, and daily routines shape how loneliness is experienced and remedied, foreign-developed models require cultural adaptation and evaluation of broader outcomes—such as cognitive function and quality of life—before use in Thailand. 12
To address this gap, the present study aims to determine the effects of Together We Thrive, a culturally adapted, group-based psychosocial program for older adults in a province in Northern Thailand. The intervention was guided by the Geriatric Rehabilitation Nursing Model, 17 which emphasizes collaboration between older adults and trained healthcare professionals, who serve as facilitators of the intervention, in addressing health challenges and promoting well-being. The model highlights shared goals, mutual trust, and emotional support as key processes that foster social connection, reduce loneliness and depression, stimulate cognitive function through active engagement, and enhance overall quality of life.
In addition, this program was developed through a comprehensive review of the literature on effective group-based psychosocial interventions for loneliness among older adults. In particular, the foundational structure and content were adapted from a well-established Finnish model 11 which integrates guided group discussions, reminiscence activities, and shared tasks to enhance social engagement and emotional well-being. The Finnish program demonstrated improvements in loneliness, mood, and perceived social support by intentionally cultivating positive group dynamics. Recognizing that interventions are influenced by cultural context, the original program was modified to align with the values, beliefs, and daily practices of older adults in Northern Thailand. This cultural adaptation process was guided by input from gerontological experts familiar with the local context to ensure relevance and acceptability. To verify program acceptance, a pilot intervention was conducted in a group of 8-9 older adults. A nurse and health volunteer who acted as group leaders delivered the pilot program. Then we conducted the main study to implement the full-scale Together We Thrive program and determine the program effectiveness in improving key outcomes—social connection, loneliness, depression, cognitive function, and overall quality of life—among a larger sample of 50 older adults. It was hypothesized that participation in the 12-week, 12-session intervention would lead to significant improvements across these outcomes.
Methods
Study Design
This quasi-experimental study evaluated Together We Thrive, a 12-week, 12-session, culturally adapted, group-based psychosocial program for older adults with loneliness. The study was conducted in two stages: (1) cultural adaptation of the intervention based on a literature review and expert panel input, and (2) evaluation of the effectiveness of the adapted program.
The study adhered to the TREND (Transparent Reporting of Evaluations with Nonrandomized Designs) statement. 18
Participants
A total of 50 older adults were recruited between January and March 2024 from geriatric clinic records and community centers in Chiang Mai Province, Northern Thailand, where the prevalence of loneliness among older adults is reported to be the highest in the region. Participants were recruited through convenience sampling, with the assistance of clinic nurses who were familiar with the local social and cultural context. Nurses identified potentially eligible individuals during routine clinic visits and briefly informed them about the study. All eligible individuals were invited to participate, and those who expressed interest were provided with detailed study information before giving informed consent. The clinic nurses were trained to administer standardized dichotomous (yes/no) screening tools, including a single-item question—“Do you often feel lonely?” 19 —and the Likert 6-item Revised UCLA Loneliness Scale (Thai version), 20 to identify individuals likely experiencing loneliness. With permission from the original author, the single-item question “Do you often feel lonely?” 19 was translated into Thai using the WHO 21 forward-backward translation method. A blinded bilingual expert conducted the back-translation to ensure semantic and conceptual equivalence. Content validity was evaluated by 5 experts in gerontology and mental health, resulting in a content validity index (CVI) of 1.0. The Thai version was then tested for internal consistency in a sample of 30 older adults reporting loneliness, yielding a Cronbach’s alpha of .95. Additionally, pilot testing with five older adults confirmed the item’s clarity and ease of comprehension. Screening and preliminary assessments were conducted within the community prior to referring eligible participants.
The inclusion criteria were as follows: (1) aged 60 years or older; (2) experiencing loneliness, defined as scoring above the 75th percentile on the RULS-6, which categorizes loneliness levels as low (below the 25th percentile), average (25th-75th percentile), and high (above the 75th percentile) 20 ; (3) ability to communicate in Thai; (4) no impairments in mobility, vision, or hearing; and (5) willingness to participate in the program. Exclusion criteria included: (1) a medical diagnosis of Alzheimer’s disease or other forms of dementia; (2) suspected dementia, indicated by a score below 24 on the Thai Mental State Examination 22 or a cognitive assessment score below 26 23 ; or (3) a diagnosis of schizophrenia, severe depression, life-threatening conditions such as acute heart disease, advanced cancer stage or terminal-stage cancer, or any other condition that could interfere with participation or compromise data reliability as indicated in their medical report.
Sample Size
The sample size was calculated using G*Power 3.1.9.7 for a repeated measures ANOVA with a within-between interaction. An average effect size of 0.35 was selected based on prior evidence from a randomized controlled trial (RCT) by Pitkala et al, 11 which reported a moderate effect (Cohen’s d = 0.45), and a meta-analysis by Jarvis et al, 24 which reported a small effect (d = 0.25) for group-based interventions reducing loneliness as measured by the UCLA Loneliness Scale. Given the similarity in population, intervention type, and outcome measure, this effect size was deemed appropriate for the current study. To ensure adequate sensitivity and minimize the risk of Type II error, a statistical power of 0.95 was used, consistent with recommendations for psychosocial intervention studies where detecting meaningful change is critical. 25 With α = .05, 2 groups, 3 measurement points (baseline, post-intervention, and follow-up), an assumed correlation among repeated measures of .5, and a nonsphericity correction ε = 1, the required total sample size was 24 participants (12 per group). To account for an anticipated 20% attrition rate, based on Pitkala et al, 11 the final planned sample size was set at 28 participants.
A total of 70 potential participants were initially screened for eligibility by clinic nurses. The principal investigator (PI) then conducted further eligibility verification, including a review of participants’ medical records. Of these individuals, 54 met the inclusion criteria and 50 provided informed consent and were enrolled in the intervention (recruitment rate = 92.59%).
Treatment Group Allocation
Eligible participants (n = 50) were randomly assigned to either the experimental (n = 25) group or control group (n = 25) using a computer-generated block randomization sequence with a 1:1 allocation ratio. Randomization was stratified by gender and age group (60-69, 70-79, and 80+ years) to ensure balanced representation across conditions. Group assignments were concealed using sealed, opaque envelopes prepared by a research assistant who was not involved in enrollment or data collection. Following consent and baseline assessment, participants were informed of their group assignment by a coordinator unaffiliated with the outcome measurement. The experimental group received the culturally adapted 12-session Together We Thrive intervention, while the control group attended a one-day health education session and received standard care through local community health centers. Although some participants may have been acquainted within their communities, they rarely had opportunities to meet or interact regularly due to social isolation and weakened networks. Furthermore, the intervention was delivered in structured, closed groups designed to cultivate intentional group dynamics, which differs substantially from casual interactions or usual care. Thus, prior acquaintance across treatment and control groups was unlikely to influence outcomes.
Intervention
Phase 1: Adaptation of the Intervention Program
After receiving permission from the copyright holder, a group-based psychosocial intervention originally developed in English 11 was used as a foundation for program development. The content was culturally adapted following the WHO guidelines to ensure contextual relevance for older adults in Northern Thailand. 21 Two bilingual researchers independently conducted forward translations, focusing on linguistic accuracy and cultural appropriateness. The resulting versions were synthesized into a single draft by the PI, followed by a consensus meeting with the translators to refine consistency and clarity.
A back-translation was then conducted by a linguistic expert unfamiliar with the original program to ensure conceptual equivalence. The draft was reviewed by the PI and translators for alignment with the source material. To enhance cultural relevance, a focus group discussion was held with stakeholders, including eight older adults with loneliness, two community health nurses, three nursing faculty, two local leaders, and six health volunteers with at least one year of experience in older adult health or welfare. Their feedback guided the adaptation of program activities to reflect Northern Thai cultural practices, values, and daily life contexts. The revised version was then reviewed by a panel of five experts—comprising one geriatric psychiatrist, three gerontological nursing faculty members, and one advanced practice nurse specializing in elder care. The panel assessed the program’s safety, relevance, and cultural appropriateness, resulting in the final version used in Phase 2 of the study.
Phase 2: Intervention Implementation
Before evaluating the program’s effectiveness in a larger sample, the PI trained six facilitators—registered nurses—to strengthen their skills in delivering the intervention and monitoring session activities. Each facilitator was instructed to complete semi-structured field diaries for every group session, documenting key observations such as attendance, reasons for absences, session content, group dynamics, and any interpersonal issues. Following the training, the PI conducted a return demonstration, during which facilitators were asked to demonstrate their competency in facilitating loneliness intervention sessions and to clarify any aspects of program delivery as needed. Prior to implementing the full-scale Together We Thrive program, a pilot study was implemented with 8 community-dwelling older adults experiencing loneliness. The pilot phase was conducted between March and May 2024. Preliminary findings demonstrated the program’s feasibility, evidenced by a low attrition rate (12.5%) and high participant satisfaction (mean score: 4.82 out of 5.00)—the program was deemed feasible for full implementation.
The finalized intervention consisted of 12 weekly face-to-face group sessions delivered over a 3-month period between May and November 2024, followed by a 24-week follow-up assessment. Each group was structured as a closed group, meaning that membership was fixed at the beginning of the intervention. No new participants were added during the intervention period, even in cases of withdrawal, dropout, or death. Each group comprised eight or nine participants, one group leader, and one assistant, with two facilitators assigned per group. Sessions lasted 90 to 120 min and followed a consistent structure throughout the program. Group leaders were professional nurses who had received training from the PI team 2 weeks prior to implementation and were provided with a detailed session protocol. Once the intervention began, no new members were admitted ensuring stable group dynamics.
Sessions were held in meeting rooms at community centers. To improve accessibility, transportation was arranged for socially isolated older adults. Each session followed a standardized activity protocol and was led by the same facilitator throughout the 12 weeks to ensure consistency. Facilitators were trained to manage group dynamics, promote participant safety, encourage peer support, and facilitate equal participation to support group maturation.
The first session emphasized person-centered care, trust-building, and collaborative goal-setting. Participants were introduced to the program’s objectives, schedule, and activities. They were encouraged to get to know one another and begin discussing their experiences with loneliness in a supportive environment. Each participant was also invited to set a personal goal related to reducing loneliness in collaboration with the interventionist. Refreshments and lunch were provided at no cost to foster a welcoming atmosphere and support informal social interaction.
Detailed in Supplemental Material 1, sessions 1 through 12 included a variety of culturally relevant and thematic activities, such as arts and cultural activities (eg, flower arrangements and handcrafts using banana leaves), physical activities (eg, traditional folk dancing and stretching), and cognitive training and reminiscence (eg, “My bedroom when I was a child”). Other group-selected activities included cooking local dishes, visiting temples, and participating in Northern Thai duet singing (Joi-Sor). These sessions addressed emotional and social aspects of loneliness and deliberately promoted group cohesion through structured group development processes. Facilitators were encouraged to empower participants; foster peer connections; and guide, rather than direct, group interactions—creating an environment of equality, support, and belonging.
In addition, participants gradually opened up about their loneliness and personal experiences. As group bonds deepened, occasional interpersonal tensions, such as teasing or criticism, naturally emerged. These incidents were managed by trained facilitators using skills taught during the program’s preparatory phase. This ongoing effort to support healthy group dynamics was a core component of the intervention.
In contrast, the control group received routine care through community health center clinics. Participants in this group attended a one-day educational session delivered by clinic nurses that included information about loneliness, dementia, cognitive training, and physical activities for brain health. In addition, this group had the option to attend voluntary community-based activities (eg, senior clubs or recreational programs) that were offered once per month in their communities and facilitated by untrained facilitators during the study period. However, these activities were not structured to promote group dynamics, emotional bonding, or mutual support. Thus, only the experimental group received a structured, guided program explicitly designed to reduce loneliness through group-based psychosocial processes.
At post-intervention (Week 12, Time 2), outcome data were collected by 2 blinded research assistants who were trained in standardized protocols to ensure consistency by the PI. The inter-rater reliability, assessed using the intraclass correlation coefficient, exceeded 0.80, indicating a high level of agreement. Follow-up data were collected at Week 24 (Time 3). By this point, 2 male participants in the control group had withdrawn, resulting in a dropout rate of 4%. In total, 48 of the 50 enrolled participants completed the intervention and follow-up assessments (see Figure 1).
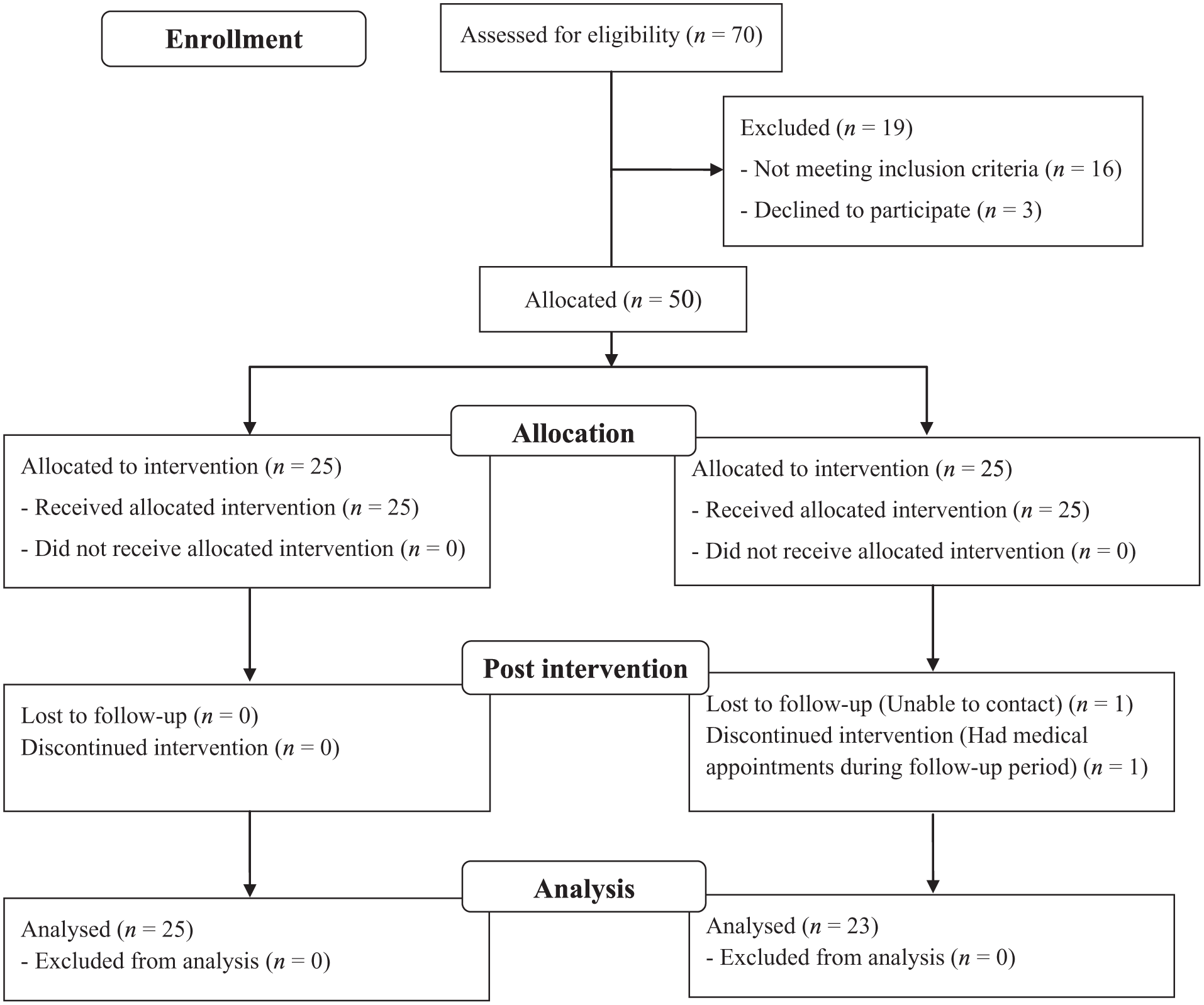
Participant flow diagram.
Intervention Process Monitoring and Fidelity Assessment
Trained facilitators, 6 registered nurses, maintained semi-structured field diaries for each group session to record key observations, including attendance, reasons for absences, session activities, group dynamics, and any interpersonal issues. After the intervention, the PI reviewed these diaries and requested clarification or additional details as needed using a structured fidelity checklist.
The intervention fidelity checklist detailed in Supplemental Material 2 was assessed using a 17-item checklist developed specifically for this study. The tool, titled Fidelity Assessment of the Psychosocial Group Intervention for Reducing Loneliness, evaluated facilitator adherence to the protocol across 3 core components: (1) the introduction/opening phase, (2) the group dynamics-building phase, and (3) the summary/closing phase. Each item was rated on a 5-point scale, ranging from 1 (required full guidance) to 5 (performed independently with confidence). Items addressed critical facilitation tasks such as welcoming participants, introducing group rules and objectives, encouraging emotional sharing, managing group interactions, and summarizing session content. Facilitators completed the checklist after each session, and the PI verified the completeness and consistency of the records. The checklist was validated by a panel of five experts—two gerontological nursing faculty members, one psychiatric physician, one nurse practitioner, and one geriatric psychiatrist—and achieved a content validity index (CVI) of 0.96, indicating good content validity.
In Phase 2, six trained facilitators conducted small group sessions with participants in the experimental group, maintaining a facilitator-to-participant ratio of 1:8-9. Adherence to the intervention protocol was assessed by the PI across all 12 sessions using a 17-item fidelity checklist. The average fidelity scores across all 6 facilitators ranged from 4.76 to 4.98 throughout the 12 sessions, reflecting a consistently high level of adherence to the intervention protocol.
Monitoring and Reporting of Adverse Events
Throughout the intervention period, adverse events were actively monitored and documented to ensure participant safety. Facilitators were trained to observe and report any physical, emotional, or psychological distress experienced by participants during or immediately following group sessions. At the beginning of each session, participants were invited to voluntarily disclose any discomfort or concerns, and a brief well-being check was conducted. If any participant exhibited signs of distress, facilitators provided immediate support and referred the case to a clinic nurse or mental health professional when appropriate.
All reported adverse events were recorded in a structured log maintained by the PI. Events were categorized by type (eg, physical discomfort and emotional distress), severity (mild, moderate, and severe), and relatedness to the intervention (related, possibly related, and unrelated). No serious adverse events were reported during the intervention or follow-up phases. Minor events, such as temporary emotional discomfort triggered by reflective activities, were managed on site and resolved without further clinical intervention.
The study adhered to ethical protocols approved by the institutional review board, and a data safety monitoring process was in place, with weekly reviews of facilitator field notes and participant feedback forms to identify any emerging concerns. Participants retained the right to withdraw from the study at any time without penalty or loss of care.
Control Group
Twenty-five older adults in the control group attended a one-day health education session and continued to receive standard care through local community health centers. In addition, they participated in routine community center activities, which included light physical activity classes, basic education on loneliness, cognitive training, and access to psychological consultation services provided by clinic nurses. These activities, however, were not structured to promote group cohesion or facilitate guided psychosocial processes. In addition, this group had the option to attend voluntary community-based activities (eg, senior clubs or recreational programs) that were offered once per month in their communities and facilitated by untrained facilitators during the study period.
Measurements
Demographic Information
Demographic and health-related data were collected, including data on gender, age, marital status, education level, and presence of chronic diseases.
Loneliness
Loneliness was assessed using the 6-item Revised UCLA Loneliness Scale (RULS-6) developed by Russell. 5 Items are rated on a 4-point Likert scale (1 = Very often/Always to 4 = Never), with higher scores indicating lower loneliness. Scores are categorized as high (3.01-4.00), moderate (2.01-3.00), or low (1.00-2.00) loneliness. The Thai version, translated by Wongpakaran et al 20 with permission, demonstrated excellent internal consistency (Cronbach’s alpha = .99) and a good model fit according to Rasch analysis. 20
Social Network
Social network was assessed using the Thai version of the Lubben Social Network Scale (LSNS-6). 26 The LSNS-6 comprises 6 items, divided into 2 subscales: 3 items assess family connections, and the other 3 assess friendships. 27 Each item evaluates the number of people with whom the respondent (1) maintains regular contact, (2) feels at ease discussing private matters, and (3) can call upon for help. Responses are scored on a 6-point Likert scale ranging from 0 (none) to 5 (9 or more), yielding a total score from 0 to 30, with higher scores indicating stronger perceived social networks. The Thai version has demonstrated strong internal consistency (Cronbach’s alpha = .81) and construct validity among older Thai populations. 26
Depression
The Thai Geriatric Depression Scale—Short Form (TGDS-6), adapted by Wongpakaran et al, 28 was used to assess depressive symptoms over the past month. The scale comprises 6 Yes/No items, with a cut-off score of ≥2 indicating possible depression. It demonstrated strong construct validity (CFA accuracy >0.8), sensitivity (73.29%), and specificity (81.24%). 28
Cognitive Function
Cognitive function was measured using the Cognitive Failures Questionnaire (CFQ) by Broadbent et al. 29 The Thai version includes 25 items rated on a 5-point Likert scale, with scores ranging from 0 to 100; higher scores indicate more frequent cognitive failures. It demonstrated strong content validity (CVI = 0.92) and internal consistency (Cronbach’s alpha = .87), 30 with CFA supporting its construct validity.
Quality of Life
The World Health Organization Quality of Life Brief Scale (WHOQOL-BREF) 31 in its Thai version was used to assess quality of life across 4 domains: physical health, psychological well-being, social relationships, and environment. 32 The WHOQOL-BREF uses a 5-point Likert scale, with higher scores reflecting a better QoL. Each subscale score is determined by summing the responses to the items associated with that subscale. The total quality of life (QOL) score was calculated by summing the scores of the 4 domain subscales—physical health, psychological well-being, social relationships, and environment—along with the 2 general items assessing overall quality of life and general health. Since the number of items varies across domains, domain scores are standardized by averaging the item scores within each domain and multiplying by 4, resulting in a consistent score range of 4 to 20 for all domains. The Thai version of the WHOQOL-BREF demonstrates good internal consistency with a Cronbach’s alpha of .83. 32
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Suan Dusit University, Thailand (SDU-RD-HS 2023-025). All participants were provided with both written and verbal information outlining the study’s objectives, data collection procedures, potential risks, and anticipated benefits. They were informed of their right to withdraw from the study at any time and for any reason, without the need to provide an explanation. Participants were also assured that all data would be kept confidential and used solely for research purposes.
Data Analysis
The data were analyzed using IBM SPSS statistical software, version 22.0, with the alpha level set at <.05. Descriptive statistics of frequency, percentage, mean, and standard deviation were employed to analyze participation and dropout rates. Chi-square and Fisher’s exact tests were applied to compare baseline characteristics between the experimental and control groups. An independent t-test was used to compare the outcome variables between the experimental and control groups at the baseline (Week 0; Time 1). To assess differences in the 6-item revised UCLA loneliness, Lubben social network, CFQ, TGDS-6, and WHOQOL-BREF scores over time, intention-to-treat analysis as a 2-way repeated-measures ANOVA was conducted, with 1 between-subjects variable (group: experimental vs. control) and 1 within-subjects variable (time: pre-intervention, post intervention, and follow-up). Post hoc analysis was performed using the Bonferroni-corrected t-test to examine statistically significant changes. Effect sizes were calculated using partial eta squared (η2), which expresses the sum of squares of the effect in relation to the sum of squares of the effect and the sum of squares of the error associated with the effect. 33 No missing data or extreme outliers were met in either the experimental or control groups. Data were analyzed for 25 participants in the experimental group and 23 in the control group. Histograms indicated visual normal distributions for the 6-item revised UCLA loneliness, Lubben social network, CFQ, TGDS-6, and WHOQOL-BREF scores. Tests for homogeneity of variance between the groups showed no statistically significant differences (P > .05). Mauchly’s test indicated a violation of sphericity (P < .05). While linear mixed-effect models are preferred for unbalanced data and sphericity violations, a two-way repeated measures ANOVA was used with Greenhouse-Geisser correction to ensure valid results. This method was applied for the interpretability, established use in a similar study, 34 minimal group size imbalance, and absence of missing data.
Results
Participant Characteristics
A total of 48 participants completed in the program (25 experimental and 23 control). Although the experimental group was older on average (M = 76.40 vs. 70.35 years), the difference was not statistically significant (P = .981). Most participants were female (92%), with no significant difference in sex distribution between groups (P = .610). The majority had completed primary school (over 87% in both groups), and monthly income was slightly higher in the control group, though not significantly (P = .064). Most participants were widowed (68% experimental, 60.9% control), and marital status did not differ significantly (P = .402). Chronic conditions were common in both groups, with diabetes more frequent in the experimental group (48.0% vs. 26.1%), and hypertension similarly prevalent (44.0% vs. 43.5%). However, no significant differences in chronic disease status were found (P = .838; see Table 1).
Characteristics of the Participants (n = 48).
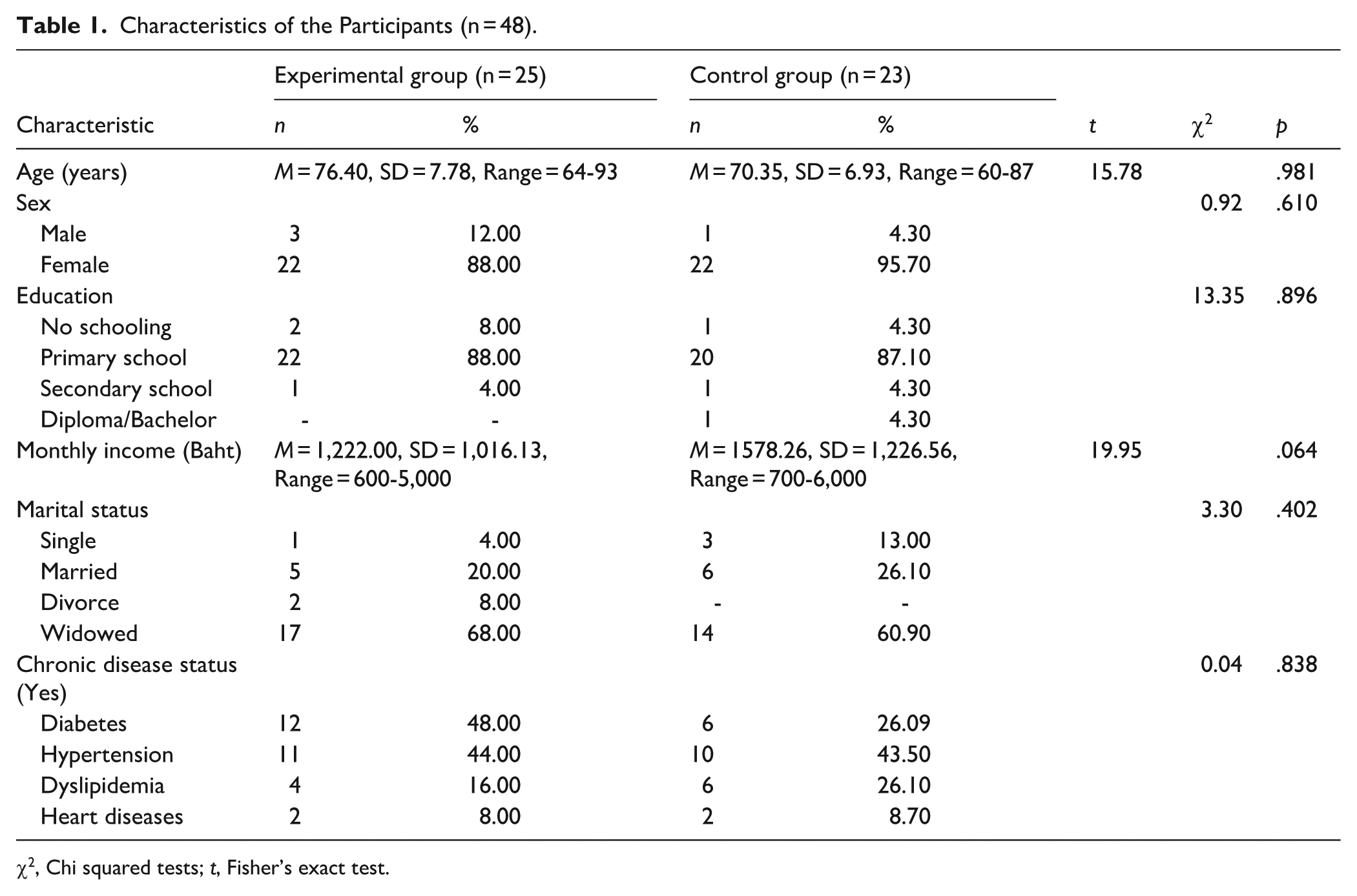
χ2, Chi squared tests; t, Fisher’s exact test.
Outcomes
The results of the 2-way repeated-measures ANOVA (see Table 2) indicated that the mean scores of expected outcomes among participants varied across the 3 time points: baseline (Time 1, Week 0), post-intervention (Time 2, Week 12), and follow-up (Time 3, Week 24). Significant interaction effects between groups were observed for loneliness, F(1.98, 59.40) = 3.49, P = .037, partial η² = .104; social network, F(1.66, 49.79) = 3.67, P = .031, partial η² = .109; and quality of life, F(1.99, 59.68) = 3.86, P = .026, partial η² = .114.
The Interaction Effect (Time × Group) of the Mean Scores of Outcome Variables Between the Experimental Group (n = 25) and Control Group (n = 23) Measured at 3 times: Baseline (Week 0, Time 1), Post-intervention (Week 12, Time 2), and Follow-up (Week 24, Time 3).

p < .05.
However, no significant interaction effects between groups were observed for depression, F(1.93, 57.88) = 0.92, P = .403, partial η² = .030; and subjective cognition decline, F(1.71, 52.99) = 0.34, P = .710, partial η² = .011. These results indicate that changes in these outcomes did not significantly differ between the experimental and control groups (see Table 2).
Post hoc analyses revealed significant differences over time in loneliness, social network, and quality of life scores within both the intervention and control groups. For loneliness scores, participants in the intervention group experienced a substantial reduction from baseline (Time 1; M = 14.52, SD = 4.43), to post-intervention (Time 2; P < .001; M = 8.84, SD = 3.47), with a mean decrease of 6.50 points. This improvement was sustained at follow-up (Time 3; P < .001; M = 8.50, SD = 2.37). In contrast, the control group showed a modest reduction of 3.63 points between Time 1 (M = 14.13, SD = 3.65) and Time 2 (M = 12.04, SD = 3.97; P = .045); however, this change was less than that observed in the intervention group and was not maintained by Time 3 (M = 13.68, SD = 4.66), as loneliness scores increased again (P > .05; see Figure 2).

Comparisons of means the Thai version of 6-item revised UCLA loneliness, Lubben social network score, and WHOQOL-BREF score.
For social network scores, the intervention group showed significant and meaningful improvements from Time 1 (M = 9.08, SD = 5.80) to Time 2 (M = 19.92, SD = 4.22; P < .001; mean difference = 11.44) and from Time 1 to Time 3 (M = 16.88, SD = 5.94; P = .007; mean difference = 8.25). The change from Time 2 to Time 3 was not statistically significant (P = .480). The control group also demonstrated a statistically significant improvement from Time 1 (M = 12.08, SD = 6.74) to Time 2 (M = 15.82, SD = 6.22; P = .004), but with a smaller mean difference of 5.69. This effect was not sustained at Time 3 (M = 10.38, SD = 8.68; P > .05), as scores returned to near-baseline levels (see Figure 2).
In terms of quality of life scores, the intervention group experienced a significant improvement from Time 1 (M = 100.56, SD = 10.41) to Time 2 (M = 114.20, SD = 10.56; P = .011), with a mean increase of 13.63 points, although the improvement from Time 1 to Time 3 (M = 110.13, SD = 11.52) did not reach statistical significance (P = .078). No significant changes in quality of life were observed in the control group across any time points (P > .05; see Figure 2).
Discussion
To our knowledge, this study provides compelling evidence that a culturally adapted, group-based psychosocial intervention—modified from the Finnish Circle of Friends model—can significantly reduce loneliness and improve both social networks and quality of life among older adults in Northern Thailand. These improvements were sustained across the 12-week intervention and at the 24-week follow-up, supporting the effectiveness of guided group processes in achieving lasting psychosocial benefits. Although several recent studies in Thailand have shown that group interventions can reduce loneliness among older adults, few have evaluated their effects on more comprehensive outcomes such as quality of life, a critical determinant of overall health and well-being in this population.
The intervention used in this study was adapted from the Finnish Circle of Friends model 11 and was guided by the Geriatric Rehabilitation Nursing Model. In accordance with this framework, each session was intentionally designed to foster group dynamics—structured, evolving interpersonal processes that promote trust, belonging, and emotional connection among participants. The Geriatric Rehabilitation Nursing Model also emphasizes collaborative goal-setting, which was incorporated through shared planning between facilitators and participants, as detailed in the intervention structure. Importantly, all 12 sessions were culturally adapted to reflect the lifestyle and traditions of older adults in Northern Thailand. For instance, in the arts and crafts activity, the intervention incorporated Buddhist cultural practices, which hold significant meaning in the lives of most Northern Thai people. Participants were invited to create banana-leaf flower offerings, traditionally used in temple rituals, allowing them to engage in meaningful artistic expression that was spiritually and culturally relevant. This contextual adaptation may have contributed to the exceptionally high retention rate (100%) observed in the experimental group, further highlighting the feasibility and acceptability of this approach.
The current findings demonstrate the effectiveness of such interventions within a Northern Thai cultural context, showing that when thoughtfully adapted, group-based psychosocial interventions are impactful across different sociocultural settings. However, there is still limited evidence to show how this group-based psychosocial intervention works for other Asian populations. 35 Overall, the original Finnish Circle of Friends program has been shown to reduce loneliness and improve social networks, quality of life, and cognitive health among older adults across Finnish communities.11,36 Moreover, a more recent adaptation of the original program—called Friends in Nature—Helsinki, which shortened the intervention to 9 sessions—has also demonstrated similar benefits in a different setting within the Helsinki metropolitan area. 37 Consistent with these outcomes, our study found a significant improvement in quality of life among participants in the experimental group for loneliness reduction and quality of life improvement, sustained through the follow-up period.
A key factor contributing to the above-mentioned outcomes is the intentional use of group dynamics as a central mechanism of change. The adapted intervention in this study followed the core principles of the Circle of Friends program, which emphasizes the development of positive group processes—such as mutual trust, peer support, emotional openness, and shared responsibility. 11 These dynamics of the group were cultivated through 12 regular, structured sessions that encouraged participants not only to engage in activities together but also to co-create the group experience. As the group evolved over time, the participants in the experimental group moved from being passive recipients to active contributors, which enhanced their sense of belonging and interpersonal connectedness. This strong group cohesion played a critical role in reducing feelings of loneliness, expanding social networks. Consequently, once loneliness is reduced, it can significantly improve quality of life because loneliness is closely tied to multiple dimensions of well-being—emotional, psychological, and even physical. 8 For example, older adults feel lonely, and they often experience a lack of meaning, reduced self-worth, and a diminished sense of belonging, all of which negatively affect their emotional health. 38 In addition, the closed-group format, trained facilitators, and emphasis on equality and shared leadership enabled participants to establish deep emotional bonds. As group cohesion grew, so did mutual empathy and a sense of collective identity. This aligns with Tuckman’s stages of small group development and supports the theoretical claim that well-facilitated group dynamics can transform temporary interactions into enduring social support systems, even after the formal intervention has ended. 39
Interestingly, the control group did show some initial improvements in loneliness, but the change was not maintained in the follow-up period. A possible explanation for this is that educational activities and unstructured activities conducted by the health volunteers could improve social interaction, but these may not be sufficient for lasting change. This supports previous assertions by Pitkala et al, 40 who noted that interventions that only increase contact without addressing the emotional and cognitive dimensions of loneliness tend to have limited long-term effects.
On the other hand, the intervention did not result in statistically significant improvements in depression, walking speed, or cognitive function. This divergence from some previous findings may be explained by several factors. First, the program was designed primarily as a psychosocial intervention, not as a physical rehabilitation or cognitive training program. As such, the activities—although engaging and emotionally stimulating—were not intensive enough to impact physical mobility or cognitive function. Second, the intervention’s 12-week duration may have been insufficient to yield measurable change in these more complex domains, which often require more prolonged and targeted approaches such as those for cognition in older adults with cognitive decline. 41 For instance, a systematic review reported that the average duration of cognitive treatment in older adults with cognitive decline was approximately 10 weeks, and the number of sessions typically increased to around 12.7 over the course of the intervention. In addition, regarding session length, this review suggests that an average length of about 92 min in older adults with mild cognitive impairment (MCI) can significantly improve cognitive function scores. 41 Unfortunately, our intervention had only 3 themes throughout the 12 sessions (as described in the Methods section) in which we mainly focus on improving social interaction by fostering a group dynamic. Another possible factor is the baseline characteristics of the participants. These findings highlight the need for future interventions to consider integrating additional components targeting physical activity and cognitive stimulation to expand the range of potential health benefits.
Our study has several strengths and limitations when compared to other research aiming to reduce loneliness among older adults facing social isolation. A major strength is the 100% retention rate achieved over the 12-session intervention, which is notably higher than dropout rates reported in previous studies, ranging from approximately 2.5% to 12%.11,36,37 Additionally, our study utilized globally validated outcome measures, enhancing the reliability and comparability of our findings. However, several limitations may affect the generalizability and internal validity of the study findings. First, the use of a quasi-experimental design with non-random group allocation may introduce selection bias and reduce the internal validity of causal inferences. Second, although the a priori sample size calculation indicated adequacy for detecting moderate effects, the final sample size may have limited statistical power to detect smaller effects, and caution is warranted when interpreting the robustness of the conclusions. Third, the absence of participant and facilitator blinding increases the risk of performance bias, particularly because all outcome measures were based on self-report instruments, which may be influenced by social desirability or response expectancy. Fourth, the findings may not be generalizable to all older adult populations, particularly those with physical or cognitive disabilities, as such individuals were not included in the sample. Lastly, the use of a non-probability sampling method limits the representativeness of the study population.
Recommendations for Future Research and Practice
Future research should aim to strengthen the internal validity of group-based psychosocial interventions by employing RCT designs with blinding procedures, where feasible. Larger and more diverse samples—including older adults with physical or cognitive impairments—are also needed to enhance generalizability and examine subgroup-specific effects. To expand the health benefits of such interventions, future programs may consider incorporating structured components targeting physical function (eg, balance and gait training) and cognitive stimulation (eg, memory games and dual-task exercises), especially for participants at risk of cognitive decline. Extending intervention duration or increasing session frequency and length—based on existing cognitive intervention research—may further enhance outcomes related to cognitive and functional health.
From a practice perspective, findings suggest that culturally adapted group interventions grounded in geriatric rehabilitation principles are feasible, acceptable, and effective in reducing loneliness and improving social and emotional well-being in older adults. Therefore, such models should be considered for integration into community health services in other regions. Training local nurses and health volunteers as facilitators could promote sustainability and scalability. Moreover, local policy efforts should support funding mechanisms and intersectoral collaboration to embed psychosocial interventions within existing aging and primary care frameworks. Digital or hybrid adaptations could also be explored to increase accessibility for homebound or rural older adults.
In conclusion, this study demonstrates that a group-based psychosocial intervention embedded in structured group dynamics and culturally adapted to the Northern Thai context can significantly reduce loneliness and enhance social networks and quality of life among older adults. While effects on physical and cognitive health outcomes were not observed, the strong psychosocial benefits suggest that such interventions can play a key role in improving the emotional and relational well-being of older adults, particularly those at risk of social isolation. Future research should explore integrated models that combine psychosocial support with targeted physical and cognitive activities to provide a more holistic approach to healthy aging.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251380614 – Supplemental material for A Group-Based Psychosocial Program for Reducing Loneliness in Older Adults: A Quasi-Experimental Study
Supplemental material, sj-docx-1-jpc-10.1177_21501319251380614 for A Group-Based Psychosocial Program for Reducing Loneliness in Older Adults: A Quasi-Experimental Study by Wachira Suriyawong, Ruksanudt Budda, Korawit Sriprasert, Noppamas Pipatpiboon, Wilawan Tuanrat, Decha Tamdee, Thanida Pumthait and Panawat Sanprakhon in Journal of Primary Care & Community Health
Supplemental Material
sj-docx-2-jpc-10.1177_21501319251380614 – Supplemental material for A Group-Based Psychosocial Program for Reducing Loneliness in Older Adults: A Quasi-Experimental Study
Supplemental material, sj-docx-2-jpc-10.1177_21501319251380614 for A Group-Based Psychosocial Program for Reducing Loneliness in Older Adults: A Quasi-Experimental Study by Wachira Suriyawong, Ruksanudt Budda, Korawit Sriprasert, Noppamas Pipatpiboon, Wilawan Tuanrat, Decha Tamdee, Thanida Pumthait and Panawat Sanprakhon in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors would like to thank our colleagues particularly the registered nurses a who acted as research facilitators, the village health volunteers, and the older people participants who so willingly participated in this study. In addition, we sincerely thank the Publication Support Center, Faculty of Nursing, Chiang Mai University, for their professional assistance with editorial support, which greatly enhanced the clarity and quality of this manuscript. Lastly, we are deeply grateful to the Professor Dr. Daniel Thomas Bressington, visiting professor, for his constructive feedback and insightful suggestions, which significantly strengthened the study design and the interpretation of the findings.
ORCID iDs
Ethical Considerations
This study received ethical approval from the Ethical Review Committee for Human Research in Health Science, Suan Dusit University, Thailand (Study ID: SDU-RD-HS 2023-025). The approved project was entitled “Development of a Psychosocial Addressing Loneliness Program to Enhance Sustainable Health Outcomes among Older Adults Facing Social Isolation,” with Subprotocol 2: “Pilot Testing of a Group-Based Psychosocial Addressing Loneliness Program for Older Adults with Social Isolation.” All procedures were conducted in accordance with the ethical principles of the Declaration of Helsinki and applicable national regulations.
Consent to Participate
Written informed consent for participation in this study was provided by the participants.
Author Contributions
WS, PS, RB, KS, NP, WT, DT, and TP: Made substantial contributions to conception and design, and acquisition of data, or analysis and interpretation of data; WS, PS, RB, KS, NP, WT, DT, and TP: Participated in drafting the manuscript or revising it critically for important intellectual content; PS and WS: Given final approval of the version to be submitted and any revision version; PS, WS, RB, KS, NP, WT, DT, and TP: Agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Council of Thailand (NRCT; Grant # N84A670539; Project code: 191385).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.