
Abstract
Background:
People with complex needs often have unmet biopsychosocial needs that require integrated services through intersectoral collaboration. Few studies have evaluated the factors influencing intersectoral collaboration for health improvement of a vulnerable population between non-profit organizations (NPOs) and primary health care partners in rural areas. The objectives of the study are: (1) to describe intersectoral collaboration between an NPO and its social and primary health care partners in a rural setting; and (2) to identify the elements that facilitate or hinder this collaboration.
Methods:
An instrumental case study was conducted through field research. Data collection included non-participant observation, semi-structured interviews, and analysis of documents. A thematic analysis was then carried out, and a case story was written.
Results:
The case study provides an in-depth account of the case, its context, and the key factors influencing intersectoral collaboration. Fourteen factors were identified as having a significant impact on intersectoral collaboration with the NPO. These factors had positive and negative effects on collaboration efforts. Several of these effects are also factors that had, in turn, effects on collaboration.
Conclusion:
Implementing intersectoral collaborations requires a shared vision, healthy relationships, and transparent, respectful communication, among other important factors. Our study provides leaders of healthcare projects in rural areas with actionable advice to address potential challenges and enhance the effectiveness of their collaborative efforts.
Keywords
Introduction
People with “complex needs” often have unaddressed biopsychosocial concerns. 1 They may face numerous social issues, such as an inability to secure a safe home; pay for food, medicine, or transportation; avoid harmful relationships; and maintain connections with friends, family, and other members of their communities.2,3 To respond effectively to these individuals’ needs, service providers must consider the full range of factors influencing their health and well-being. 4 However, significant barriers to information sharing and care coordination between providers exist, as health and mental health services are often provided in isolation.1,5,6
Primary health care provides a solution that responds to the biopsychosocial needs of a local population by improving access to comprehensive, continuous, and high-quality health and social care.7,8 To achieve this, primary healthcare establishes interventions within and across sectors through intersectoral collaboration.7,8 Allen et al, 9 drawing on Bialek et al 10 and Bryson et al, 11 defined intersectoral collaboration as the “coordinated efforts of governmental and nongovernmental agencies from multiple aspects of society to address public problems.” Such collaborations—bringing together actors from various sectors of society—can more effectively influence key determinants of health, including material disadvantage and psychosocial stressors. 12 Compared to isolated efforts by the health sector, intersectoral approaches are generally more effective, efficient, and sustainable in improving population health outcomes. 13 When collaboration is successful, the pooling of complementary resources, perspectives, and expertise leads to more innovative and impactful solutions. 14 Among the key partners involved in these collaborations are nonprofit organizations (NPOs), which in Canada, are defined as “associations, clubs, or societies that are not charities and are organized and operated exclusively for social welfare, civic improvement, pleasure, recreation, or any other purpose except profit.” 15
Intersectoral collaboration can be challenging because it requires diverse knowledge and skills from various actors and organizations. 16 Alderwick et al, 17 in a systematic review of reviews, identified five dimensions that influence intersectoral collaboration for health improvement: (1) motivation and purpose, (2) relationships and cultures, (3) resources and capabilities, (4) governance and leadership, and (5) external factors. While numerous studies have highlighted individual factors that support partnerships, Alderwick et al 17 noted a lack of evidence on how these elements interact and influence one another within collaborative processes.
Our understanding of intersectoral collaboration to address the health problems of people with complex needs is primarily derived from the experience in urban communities. In contrast, rural collaboration remains relatively understudied. 18 More research is needed to better understand the unique challenges faced by rural areas when implementing intersectoral collaborations. 18 For example, rural settings often contend with limited resources and significant geographic distances between partner organizations. 16 Despite the growing role of the nonprofit sector in delivering health and social services, particularly in response to rising demand and pressure for greater efficiency, 19 collaborative practices within this sector remain largely under-researched. 20
The study had two aims: (1) to describe intersectoral collaborations for health improvement between an NPO and its social and primary health care partners in a rural setting and (2) to identify the factors that facilitate or challenge these collaborations.
Methods
Design and Case Description
An instrumental case study was conducted through field research. 21 The case under study was an NPO serving a vulnerable population and its partnerships within the primary care and community sectors. This case was selected for its unique opportunity to collect data directly in the field during the early stages of the NPO’s development and the formation of its collaborative relationships. Field research provides a valuable framework for studying specific groups and real-world situations, enabling the observation of authentic contexts, interactions, and behaviors as they unfold. 22
Setting and Sampling
Due to the sensitive nature of the situation, we agreed with the participants that we would maintain complete anonymity regarding our research findings. As a result, descriptions of the participating organizations have been kept deliberately brief and general. Furthermore, we have chosen not to include the reference for the statistical data presented below, as doing so could disclose the specific geographic area where the research was conducted and, by extension, compromise the anonymity of the participating organizations.
The study was conducted in a rural region in southern Quebec, a francophone province in Canada, with a population of approximately 23,000 residents. Health indicators in this area reveal significant challenges: over a third of adults reported having at least one chronic illness, around a fifth experienced high levels of psychological distress, and approximately 15% were affected by mood or anxiety disorders. Just over a tenth of adults had a low income. Among those aged 24 to 65 years, nearly 20% had not completed high school and close to 25% were unemployed. Developmental vulnerability was also notable, with more than one-third of 5-year-old kindergarten children showing delays in at least one of the five developmental domains. Additionally, around 17% of the population was not attached to a family physician.
A convenience sampling strategy 23 was used to recruit a NPO providing services to a vulnerable population—defined as individuals at increased risk of developing health or psychosocial problems, or experiencing trauma due to a combination of individual and/or socioeconomic factors. 24 The recruitment process also extended to the NPO’s health and social service partners. One of the authors (CH) initiated contact through her professional network in the healthcare sector to identify existing intersectoral collaborations aimed at enhancing health-promotion services, with the goal of identifying potential participants for the study. However, the COVID-19 pandemic placed considerable strain on healthcare organizations, limiting their capacity to engage in research activities at the time. Despite these constraints, the selected case met the study’s inclusion criteria and demonstrated availability for on-site data collection, making it a relevant and feasible choice for participation.
The seven partners included in the study were a family medicine group (FMG), a healthcare establishment within an Integrated Health and Social Services Center (CISSS), three community sector organizations, and two private sector entities. FMGs bring together general practitioners and other health and social care professionals to deliver comprehensive services to the population. 25 CISSSs, for their part, are mandated to ensure the accessibility, continuity, and quality of services across their regions. They act as a central hubs for individuals facing health or psychosocial challenges, either providing direct support or referring them to appropriate resources within the territorial network. 26 These institutions encompass a range of facilities, including hospitals, local health and social services centers, long-term care homes, day hospitals, and rehabilitation centers. 27
The community organizations recruited included: (1) the local Community Development Corporation, which supports community organizations in its jurisdiction by fostering local initiatives, organizing community engagement activities, participating in consultations and collective actions, offering training, and disseminating relevant information, 28 (2) a community organization dedicated to improving the living conditions of families, and (3) a shelter for women experiencing domestic violence and their children. The two private-sector partners were a physiotherapy clinic and a self-employed doula. Doulas offer physical, emotional, and informational support to women throughout pregnancy, childbirth, and the postpartum period. 29
Participants were recruited using a snowball sampling approach, 30 beginning with the main contact at each participating organization. Individuals involved in collaborative efforts were then identified and invited to participate, ensuring representation across the various sectors.
Data Collection
The qualitative data collection consisted of the following:
(1) Nonparticipant observation of key meetings and activities conducted between July 2022 and June 2023, totaling 32 hours. These observations covered a variety of events, including NPO board meetings (n = 5), the annual general meeting (n = 1), intersectoral partnership meetings (n = 8), and NPO clinical activities (n = 2). During these sessions, the research assistant (ODS) took detailed notes on partnership dynamics, the overall atmosphere, and significant interactions that occurred.
(2) Semi-structured individual interviews were conducted with patients and key partners (n = 22). All participants were adults, and only one identified as male. The sample included two patients with complex needs who had used NPO services, 10 health and social care professionals, seven managers, two members of the NPO’s board of directors, and one support staff member. The interviews explored a range of topics, tailored to each participant’s role and experience. These included: professional or academic background, role and responsibilities, local socioeconomic context, population needs, partnership objectives, the genesis and evolution of the NPO, development of intersectoral collaborations, facilitators and barriers to collaboration, perceptions of the NPO and its partnerships, discrepancies between initial vision and current reality, sustainability of partnerships, availability of human and material resources, the impact of the pandemic on service delivery, key success factors for collaboration, and patient experiences with the services received. All interviews were audio-recorded and transcribed verbatim.
(3) Relevant documents provided by the NPO (n = 7) were also collected. These included the government’s call for projects that led to the NPO creation, its organizational chart, and its governance policy.
The study’s design incorporated an iterative approach to analysis, allowing for the identification of unexpected influencing factors and the emergence of new questions throughout the data collection process. The flexibility enabled us to refine the interview guide and incorporate additional data sources as needed. 31
Analysis
Two authors analyzed the qualitative data from interviews, nonparticipant observations, and documents: ODS, who holds a master’s degree in anthropology, and ÉH, a professor in the Department of Health Science at Université du Québec à Chicoutimi. They employed a combined analytical approach, using both deductive coding, based on the factors influencing collaboration functioning identified by Alderwick et al, 17 and inductive approach to capture emergent themes. 32 One author conducted the initial coding of all materials, while the other validated the coding tree and interpretation of the data, focusing on five interviews with participants most involved in establishing the collaboration. The preliminary results were then presented to and validated by the other authors: MB, IG, MCJ, CL and CH, all professors at the Faculty of Medicine and Health Sciences at Université de Sherbrooke. Data organization and coding were carried out using NVivo 13.
Methodological triangulation contributed to ensuring the validity and completeness of the data. 32 This approach provided a more comprehensive and contextualized understanding of the phenomena under study, thereby enhancing the depth of analysis. In addition, the interpretation of the results presented in the case story was validated by four key leaders, each representing one of the main sectors involved in the partnerships (NPO, community sector, public health, and FMG). 31 A preliminary version of the case story was shared with them for review, and their comments and suggestions were taken into account.
The credibility of the findings was further reinforced through several strategies, including prolonged engagement in the field, persistent observation, triangulation, participant validation (ie, member checking), and peer debriefing. 33
Results
The case story below (Table 1) provides a comprehensive account of the case, its context, and the key factors influencing intersectoral collaboration.
Case Story.
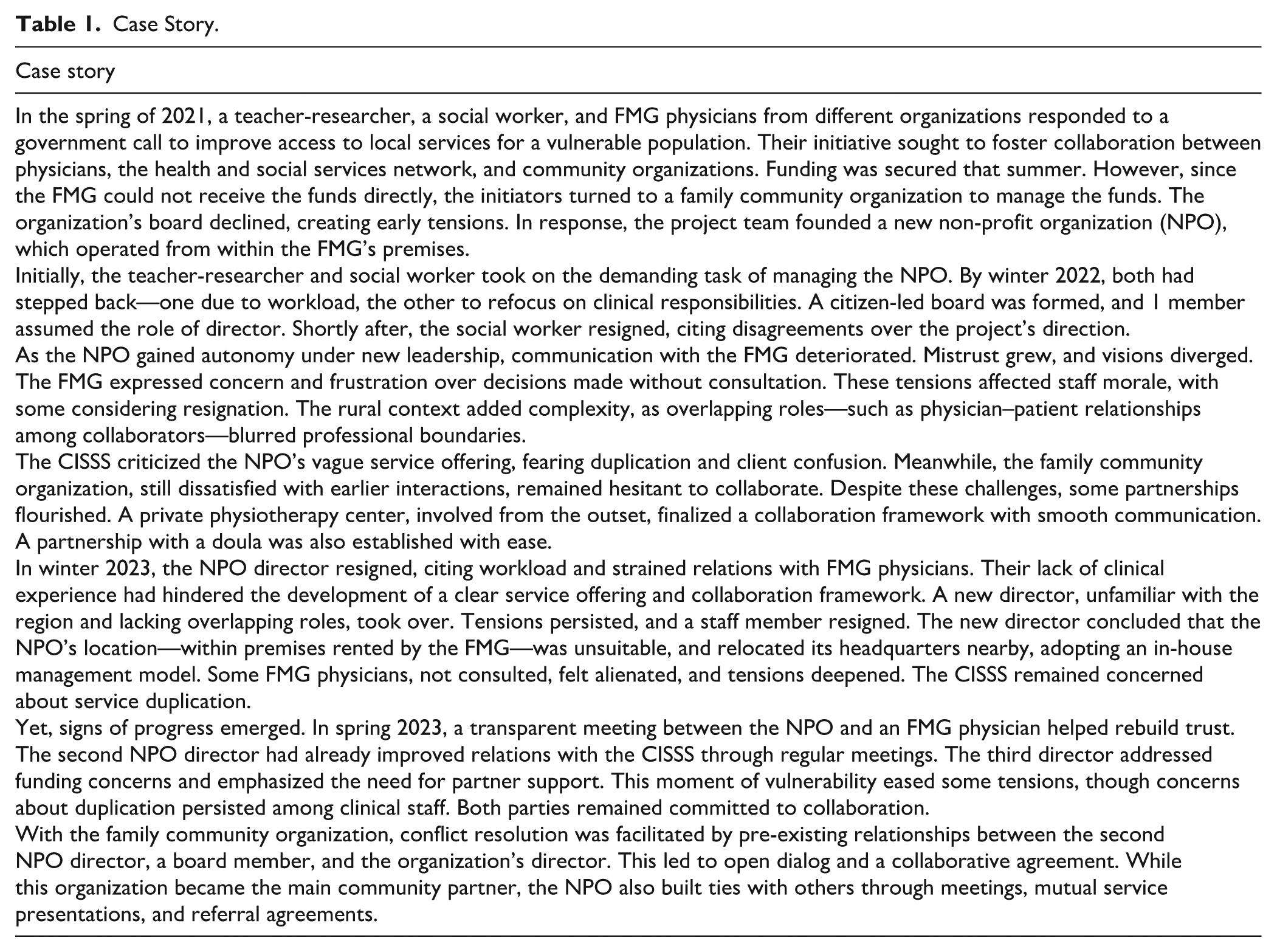
A total of 14 factors were identified as significantly impacting intersectoral collaboration with the NPO. Table 2 provides a comprehensive overview of these factors and their effects, as well as the interrelationships among them. These factors were found to have both positive and negative effects on collaboration efforts. For instance, the quantity of human resources was shown to affect workload, motivation, general atmosphere, and service delivery both positively and negatively. It is important to note that several of these effects are also factors that have, in turn, an impact on collaboration. For instance, the degree of shared vision has been shown to affect the quality of communication and the level of trust, which are also factors that create other effects.
Factors Influencing Collaboration and Their Effects.
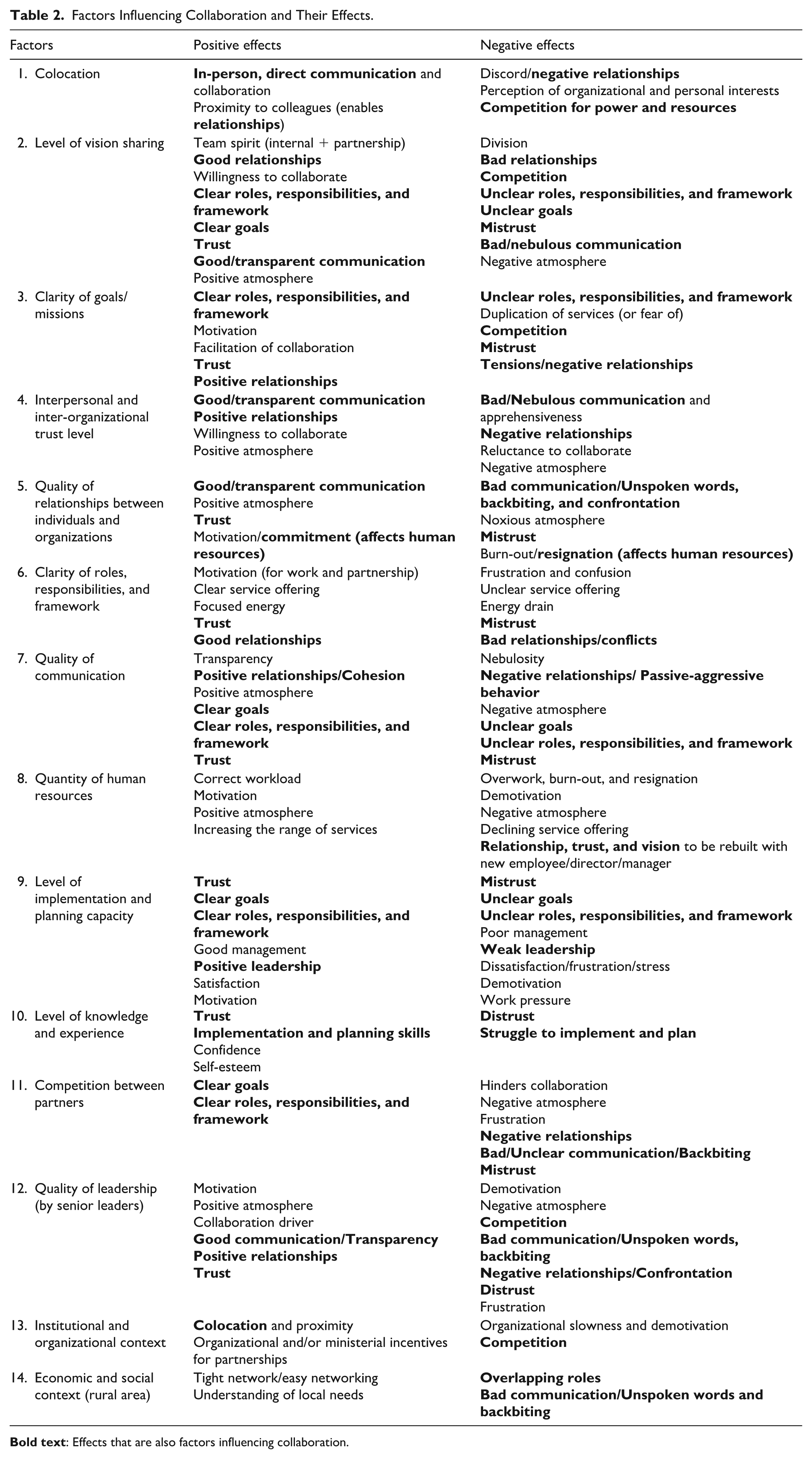
The degree of shared vision has been shown to influence several factors, including the clarity of goals; the clarity of roles, responsibilities, and frameworks; the propensity to collaborate or compete; interpersonal relationships; trust; and communication. It was an important factor with far-reaching effects that had a significant impact on collaboration. Arguably, this was the most salient factor underpinning all the collaborative efforts observed in the study. It was also identified as a fundamental condition for the quality of collaboration.
The level of trust has been shown to influence communication, relationships, atmosphere, and willingness to collaborate. Trust has been identified as a fundamental component of collaboration. Efforts to achieve healthy and effective collaboration are likely to be unsuccessful when trust is lacking, or distrust exists.
The quality of relationships has been shown to significantly impact communication quality, the general working atmosphere, trust levels, and motivation. Harmful relationships, the atmosphere they create, and a lack of recognition of others’ work have led to burnout and resignation. This phenomenon negatively affected the workload of the remaining staff and the quality-of-service delivery.
The development of personal and organizational relationships hinged on effective communication. The quality of this communication significantly impacted several areas, including trust levels, passive-aggressive attitudes, cross-sectoral cohesion, and the clarity of goals, roles, responsibilities, and frameworks. Building effective collaborations required clear, respectful, and transparent communication.
Clarity of goals significantly impacted the clarity of roles, responsibilities, and frameworks. It also raised concerns about the duplication of services, which could lead to a reduction in quality and cause customer confusion. This situation was not conducive to effective collaboration and could foster mistrust and competition.
The clarity of roles, responsibilities, and frameworks was found to significantly impact motivation levels. A lack of clarity had the potential to create a state of frustration and confusion. Additionally, these factors profoundly impacted the understanding of the service offering, which, in turn, could potentially lead to a state of mistrust. Finally, ambiguity was found to require significant energy from both staff and managers alike, as opposed to the focused energy observed when roles, responsibilities, and frameworks were clear.
Competition between partners has been shown to be detrimental. It fostered an unfavorable environment, created mistrust, and led to damaged relationships, ambiguous communication, and backbiting. Competition between individuals and organizations has been shown to undermine collaboration and hinder the achievement of collaborative goals. However, this factor has prompted leaders to define goals, roles, responsibilities, and frameworks more clearly.
Given the spatial and relational proximity of certain staff and the ministerial and organizational incentives to encourage collaboration, the institutional and organizational context had the potential to promote collaboration. However, the project’s implementation and the establishment of collaborations were characterized by slowness, which could be demotivating. Additionally, the context generated competition in service provision, hindering the practical implementation of collaborations.
Social and economic contexts positively influenced the quality of networking and the understanding of local needs. However, it has also encouraged overlapping roles in interpersonal relationships and the ambiguous communication that results from them. The participants offered nuanced perspectives on this rural context, viewing it as both advantageous and disadvantageous.
Discussion
To the best of our knowledge, this is the first case study to identify the factors that influence intersectoral collaboration between an NPO and its social and primary healthcare partners in a rural setting. This study fills a gap in the literature by providing an in-depth, context-sensitive understanding of collaboration dynamics in rural areas, an area that remains underexplored. 17 By highlighting the complexity and interdependence of these factors, our study contributes a more nuanced perspective that complements and extends previous research. Conducting this study through fieldwork enabled us to capture the evolving nature of collaboration in real time, offering rare empirical insights into how partnerships are formed and sustained in practice. Ultimately, the collaborative efforts of all parties involved led to the formation of collaborative relationships. However, the process was not without its challenges. Several factors influenced the establishment and implementation of these collaborations.
Our research shows that a shared vision is essential for effective collaboration. To ensure a productive partnership, those involved must first agree on their overall goals and establish overarching principles that will guide them toward achieving those goals. Mutual understanding is key to effective collaboration. This vision is complemented by more specific goals, roles, responsibilities, and frameworks. However, establishing a clear understanding of the desired outcomes and how to achieve them is fundamental to initiating a collaborative partnership.
Other studies have emphasized the importance of a shared vision in collaborative endeavors. Alderwick et al’s 17 systematic review of reviews supports this, noting that a shared vision is often identified as a key factor in successful collaborations. Reiter et al 34 similarly caution that mistrust may arise when parties lack a mutual understanding of the project’s vision, particularly if differences are not openly discussed during meetings. They stressed the importance of transparent communication to address these discrepancies and foster alignment.
Tsasis’s study of interorganizational collaboration among NPOs 35 also highlights that the absence of a shared vision can lead to competition, especially when collaborators are perceived as overstepping their roles. Tsasis argues that a clearly articulated vision, combined with well-defined roles and complementary goals, supports effective and nonduplicative collaboration. Our findings reinforce and extend these insights by showing how the rural context amplifies the need for trust-building and clarity of vision, given the limited resources and overlapping roles of local actors. We observed that when roles and goals are poorly defined, even well-intentioned collaboration can result in perceived duplication and friction. Conversely, when partners engage in open dialog to clarify and align their visions, collaboration becomes more cohesive and resilient.
The quality of interpersonal and interorganizational relationships also played a significant role in establishing the collaborations observed in our study. Alderwick et al 17 acknowledged the central role of this factor in determining the likelihood of successful collaboration. Among other things, Alderwick et al 17 discussed the impact of relationship history on collaborative efforts, a phenomenon we observed among collaborators. However, our study goes further by examining how these relationships unfold in the context of rural communities, where actors often occupy overlapping roles. To the best of our knowledge, our study is the only one to address the complexity and implications of overlapping roles, which are more common in rural settings, and their impact on intersectoral collaboration.
Trust and communication are widely recognized as foundational to effective collaboration. van Vooren et al 36 observed that prior working relationships help establish trust, while Steenkamer et al 37 noted that their absence can impede intersectoral efforts. Our findings echo these insights, showing that in rural contexts, dense and familiar networks can both support and complicate trust-building, particularly when roles overlap and resources are limited.
Trust influences multiple dimensions of collaborative work,17,18,34 -36,38 -40 and its development is closely tied to the quality of communication. As Alderwick et al 17 and Reiter et al 34 have shown, open, frequent, and transparent exchanges foster mutual understanding and strengthen relationships. Our study confirms these findings and adds that in rural settings, where informal communication channels are often as influential as formal ones, the tone and frequency of exchanges can shape perceptions of legitimacy and value.
Clarity around roles and goals is also essential. van Vooren et al 36 emphasized the importance of articulating these elements early in the process. In our case, uncertainty surrounding the NPO’s mandate created barriers to trust and collaboration, with concerns about service duplication delaying joint initiatives. Ultimately, our findings suggest that respectful, transparent communication is key to resolving tensions and enabling meaningful collaboration.
Limitations
This is a single case study conducted in a well-defined rural area in southern Quebec. Its findings may not be applicable to other regions of Quebec, Canada, or elsewhere in the world. However, several international studies have identified similar influential factors.17,34 -40 Some participants with professional experience outside the studied region also noted that the challenges they faced were not unique, suggesting that conflicts can emerge in any context where strong-willed leaders are present. It is important to acknowledge that the interviews took place during a period of significant interpersonal discord among individuals representing different organizations. The intensity of respondents’ emotions may have shaped their answers, and conducting the interviews at another time might have yielded more neutral or reflective responses. Finally, it is worth noting that only one interview was conducted with a man, and the rest were with women. Including a broader range of male perspectives could have enriched the analysis.
Conclusion
Intersectoral collaboration has been identified as an effective strategy for providing integrated care to vulnerable and populations with complex needs. Although such collaborations can positively impact the health of local communities, their implementation requires a shared vision, strong relationships, and transparent and respectful communication. Our study offers practical insights for rural healthcare project leaders, helping them anticipate and navigate common challenges to enhance the success of their collaborative initiatives. Further research is needed to deepen our understanding of intersectoral collaboration in rural contexts. Such research will contribute to a more comprehensive understanding of the unique characteristics and contextual factors that shape collaboration in these settings.
Footnotes
Acknowledgements
Many thanks to all the organizations and participants involved.
Ethical Considerations
The study was approved by the Ethics Committee of the CIUSSS de l’Estrie.
Consent to Participate
Each participant consented to the research by signing a consent form or verbally, depending on the context of the data collection. When observing large group meetings, consent to take notes was obtained verbally.
Consent for Publication
Not applicable.
Author Contributions
CH and ODS developed the study design with all the authors. ODS collected and analyzed the data. ÉH co-analyzed the most significant interviews with ODS and validated the coding tree and data interpretation. The participants who had been most involved in setting up the partnerships validated the case story. All the authors validated the results. ODS and CH wrote the initial drafts, and all the authors contributed to the final draft. The manuscript was first written in French and then translated and edited using DeepL Pro.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Institut universitaire de première ligne en santé et services sociaux of the CIUSSS de l’Estrie-CHUS.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data cannot be shared openly to protect the study participants’ privacy.