
Abstract
Introduction:
Universal health coverage promotes equity of access to essential health care for all, including migrants. Health systems struggle to balance global commitments to health equity with national concerns for sovereignty and security. Migrants therefore often experience inequitable access to primary care.
Objectives:
To explore migrants’ experience in accessing public sector primary care services in Emfuleni subdistrict, Gauteng, South Africa.
Methods:
A descriptive exploratory qualitative research study purposefully selected migrants and gathered data using semi-structured interviews in English, French and Portuguese. Data was thematically analysed using the framework method assisted by Atlas-ti.
Results:
Fifteen migrants were interviewed. Four main themes were identified. (1) Barriers related to legal status, financial constraints, language issues and misinformation. (2) Coping strategies that included social support, traditional beliefs and alternative practitioners. (3) Healthcare experiences that included good quality care as well as denial of care and delayed care. (4) Psychosocial and emotional effects related to stigmatisation, discrimination and mental health problems.
Conclusions:
This study sheds light on the significant obstacles that migrants have while trying to use government clinics in Gauteng, South Africa. The health system should address these factors through policy, protocols, translation services, training of staff and clear messaging in the migrant community.
Introduction
Migration is a normative characteristic of human society. The Lancet Commission on Migration and Health reported that 1 billion people changed their location in 2018. 1 Most migration is within the country of origin, within low- or middle-income countries (LMIC) and for employment or work. An important subset of migrants are asylum seekers or refugees, often because of conflict, persecution or natural disasters, including climate change. Much attention has been given to migration from LMICs to high-income countries in Europe and North America. Recently migrants have been “demonised” and stigmatised by nationalist politicians, fuelling xenophobia and creating a “moral emergency.” 1
The majority of migration in Africa takes place within the continent, with sub-Saharan Africa accommodating more than 26% of the global migrant population. 2 For example, in 2020, there were more than 11 million internal migrants in West and Central Africa. 2 With 40% of the population under 15 years, the subregion’s increasing youthful demographic will further fuel migration as unemployed young adults look for better opportunities. 3 According to the African Center for Strategic Studies, migration within Africa has been steadily increasing over the past 20 years, driven by factors such as economic challenges, conflicts, oppressive governance, a growing youth population, need for health care and the impacts of climate change. 4 In 2024, around 1 million new migrants were documented, bringing the total number of African migrants to approximately 43 million. 4
Health systems globally have been emphasising universal health coverage (UHC) as a key aspect of the sustainable development goals. 5 This implies access for all to high quality essential care without financial hardship. This movement towards UHC “for all” is meant to ensure health equity and yet migrants are often excluded or forgotten in the discourse. 1 Inequitable access to health care by migrants highlights the tension between commitments to health as a human right and UHC, and to national sovereignty and security concerns, often with underlying prejudice and misinformation amongst the electorate. 1
The most accessible part of the health system, which can respond to most health problems, is primary care. 6 Access of migrants to primary care facilities and services is therefore a key signpost to the degree of inequity in the health system. However, navigating the healthcare system may be difficult for migrants due to a lack of knowledge about the structure and functioning of primary care services. 7 In South Africa, migrants experience challenges in accessing primary care. 8 The challenges stem from systemic issues, discrimination and the attitudes and behaviours of healthcare personnel. 8 Language barriers are also a major issue, leading to breakdown in communication, misunderstandings and suboptimal care. 9 Geographical distance to healthcare facilities was another barrier. 9 Although previous research in South Africa has brought attention to these challenges, little is known about how these obstacles interact with the experiences of migrants, specifically how they perceive the quality of care, whether it is culturally appropriate, and how policies affect their decisions to seek medical attention.
This study aimed to explore migrants’ experience in accessing public sector primary care services in Emfuleni municipality, South Africa. Specific objectives were to explore their health-seeking behaviour, the barriers and enablers to access, the effects of these barriers on health outcomes and the perception of migrants regarding the quality of care received.
Methods
Study Design
This was an exploratory descriptive qualitative study that collected data via individual semi-structured interviews and in-depth accounts of migrants’ access and utilisation of primary care.
Setting
Gauteng is a major metropolitan area in South Africa with high population density that contains the cities of Johannesburg and Pretoria. In Gauteng, this study was conducted in Emfuleni subdistrict, which had a population of 945 650 in the 2022 Census. 10 Gauteng is “a province of migrants” with only 56% of the population born there, 35% coming from other parts of South Africa and 10% outside South Africa. 11 It is estimated that 4% of the population of Emfuleni were born outside of South Africa. In Gauteng, the majority of migrants from outside South Africa come from the Southern African Development Community (SADC) (82%), mostly from Zimbabwe, Mozambique and Malawi. 11 Only 7% come from other parts of Africa, 5% from Europe and 5% from Asia. Male migrants slightly outnumber female migrants (53%) and migrants are mostly of working age (20-49 years; 14% of population born outside South Africa in this age group). 11
In Emfuleni there are 28 public sector primary care facilities, including 23 clinics, 4 larger community health centres (open 24-h) and 1 community day centre (open office hours). All facilities provide acute and chronic ambulatory care across the life course. The larger community health centres have 24-h emergency centres and maternity units. In South Africa most patients will consult a nurse practitioner. Smaller clinics are visited by a doctor and larger health centres may have permanent doctors.
Study Population, Sample Size and Sampling
The study defined migrants as a person or group(s) of persons who, predominantly for reasons of sudden or progressive changes in their context that adversely affect their lives or living conditions, are forced to leave their habitual residence or choose to do so, either temporarily or permanently, and who move outside their country of origin. 12
Both documented and undocumented migrants, originating from various countries outside South Africa, were included. In addition, they had not yet obtained permanent residence or citizenship. Participants were required to be dependent on the public health sector and to have resided in Emfuleni Municipality for at least 6 months. This criterion was chosen to ensure that participants had sufficient time to interact with the local healthcare system and to form meaningful, reflective experiences related to accessing primary care services. Children under 18 years of age were excluded from the study.
Initially, a sample size of 16 participants was planned. This number was deemed sufficient to provide a diverse range of perspectives. However, the final sample size was determined by saturation of data, if the last 3 interviews did not introduce new issues or potential themes.
Initial criterion-based purposeful sampling was used to select participants. The intended criteria included: an equal number of male and female participants as well as equal numbers of those who had and had not accessed primary care. In addition, participants needed to come from at least 4 different countries and 4 primary care facilities serving different communities. To enable maximal variation across the subdistrict a larger community health centre and 3 clinics were included. Eligible migrants were identified at the reception during patient registration. To identify those that had not managed to access primary care, 1 migrant was selected at each facility and asked to identify at least 1 additional interviewee through snowball sampling.
Data Collection
Individual face-to-face semi-structured interviews were conducted with an interview guide that consisted of an opening question and several potential follow-up questions to explore all the intended topics. The guide was developed from the literature on migration, health equity and qualitative research approaches.1 -3 The opening question was: “Can you tell me about your experience accessing primary care services in Emfuleni municipality?” Topics included language and economic barriers, discrimination, cultural differences, social support, legal status and cost of care. Other relevant and unanticipated topics were also explored. Before data collection, the interview guide was piloted, and the data was not included in the study.
The interviews were audio-recorded and lasted approximately 30 to 60 min. They were conducted by the researcher in English and research assistants fluent in Portuguese and French. Interviews took place in a private room at the community health centre or clinic that was convenient for the participant.
Data Analysis
The data were transcribed verbatim and checked for errors against the audiotapes. The researcher conducted the data analysis using ATLAS.ti. French and Portuguese interviews were translated and transcribed into English by the research assistants. The 5 steps of the framework method were followed: 13
Familiarisation—The recordings were listened to, and all the transcripts and field notes were read to identify key issues for coding.
Identifying a coding framework—The key issues from step 1 were refined and converted into a set of codes. The codes were then grouped and categorised.
Coding—All the transcripts were coded using the coding framework.
Charting—The codes were organised into code families within ATLAS.ti, and a report was created for each family to consolidate all the related data
Interpretation—The reports from step 4 were interpreted to identify key themes and subthemes. Illustrative quotations were selected, and relationships between themes were identified.
Trustworthiness
The researcher was a nurse working in the primary care services of the municipality. As a novice researcher, she worked under supervision of RM throughout the study. None of the interviewees were her patients. She conducted the data analysis under supervision, particularly during the construction of the coding index and the interpretation of the data.
The researcher’s mother immigrated to the country many years ago from Lesotho which enabled the researcher to remain open and non-judgmental towards the experiences of migrants. She had no specific personal experience of being a migrant and was also mindful of the need to bracket any assumptions or presuppositions from the process. Two research assistants were used, for French and Portuguese. The first assistant CL was fluent in English and French, and an early career researcher and co-supervisor on the study. The second assistant was fluent in both English and Portuguese, a medical doctor and family physician and an honorary lecturer for the University of Witwatersrand’s Family Medicine department. The credibility of the findings was enhanced by attention to bracketing, a number of different data collectors and review of the process by the supervisor.
Findings
The characteristics of the 15 participants are shown in Table 1. Participants from Zimbabwe, Zambia and Malawi were able to speak English, the participants from Mozambique spoke Portuguese and the participants from Congo spoke French.
Characteristics of the Participants.

The following themes are described below:
Barriers to health care
Coping and support factors
Health care experiences
Psychosocial and emotional effects
Barriers to Health Care
Most of the migrants did not have valid documentation of their legal status. Some did not have passports or their passports had expired, or did not have work permits:
I was using passport that time, then my passport got lost. [30-year-old female from Zimbabwe]
Migrants also expressed difficulty communicating with healthcare providers because of language barriers. They could not speak local languages, and their English was not perfect:
I will try my broken English. [23-year-old female from Zimbabwe]
For migrants, language issues made it difficult for them to comprehend critical health information. Many expressed feeling alone, especially in social and professional contexts, where they were unable to participate in conversations and support systems due to language barriers. These experiences frequently carried over into their relationships with healthcare providers, when they needed assistance from others to understand medical directives:
Someone who understands you can’t speak his or her language but she or he will keep on talking her language then at the end there is communication breakdown. [male 48-year-old from Malawi]
Most of the migrants realised that to cope and survive in South Africa they needed to learn to speak one or more of the local languages, which was not easy, but they were determined to learn. Some learned isiZulu and some Sesotho depending on the community they lived in:
You know that time that nurse said that she can’t help me, it made me want more, to do more research about the language, to want to speak it. [28-year-old female from Zimbabwe]
One participant resorted to ignoring South Africans who expected her to speak their language because there was no way she could learn all the languages. She articulated that when she was in Polokwane, she was expected to speak in Sepedi, when she was in Cape Town she was expected to speak Xhosa, even now in Gauteng she was expected to speak Sesotho. She felt overwhelmed and frustrated, and language became a source of stress:
Even if I go to the hospital and they start like, ah, why are you saying this one and use this language, I just ignore. [28-year-old female from Zimbabwe]
Financial difficulties prevented some people from maintaining their documentation. They could not apply for work permits as this was expensive, and new passports could cost over R3500 (~US$193). Those with expired visas had to buy more days at the border for R300 (~US$17) per month:
I can buy the days for R300, it’s R300 per month. [28year-old female from Zimbabwe]
One respondent mentioned that travelling to the primary care clinic incurred a cost of about R50 (~US$3) which added to the financial strain they faced. The overall costs of transport became overwhelming:
It’s almost R50, it’s not easy, because I have to find money to go there. [30-year-old female from Zimbabwe]
Secondary care at hospitals was also a source of financial stress. For example, a 34-year-old man from Mozambique recounted an ordeal involving his pregnant partner, whose ectopic pregnancy required urgent medical intervention. The hospital demanded a payment of approximately R10,000 (~US$550), a sum he described as overwhelming:
One day she was pregnant, and the baby was outside the uterus so, she was admitted to the hospital, and that sad story is the only time I felt in trouble because they requested that I pay, I don’t remember well, but like R10000 for her to be discharged from the [public sector] hospital after the operation. That was a lot of money. [Male 34-year-old from Mozambique]
Pregnant migrants when attending antenatal care at a hospital paid R70 (~US$4) just to open a file and R385 (~US$21) per visit to see a doctor. One participant said she paid all that money with her first pregnancy and said if with her second pregnancy, she was referred to the hospital again, she was not going to go:
Now, when I gave birth, they said the sugar is fine, its normal, but if it was not, I was not going. [31-year-old female from Zimbabwe]
Anecdotes from other people were used by migrants to inform their healthcare choices. These stories, which were frequently based on misinformation, increased anxieties about being denied care, paying excessive costs or facing legal consequences. For example, despite the fact that this was not always the case, some migrants thought they would be denied entry if they did not have proper documentation:
Some, they say if you don’t have the papers, you’ll be delayed or some they say they’re gonna send you back home. [30-year-old female from Zimbabwe]
Coping and Support Factors
This theme explores the various ways in which migrants responded to challenges, adversity and stress when accessing the healthcare facility. A female participant from Zimbabwe described her first visit to the clinic for antenatal care as stress-free. She explained how her sister helped her through the process because she knew the healthcare setting well, which made it much easier for her to get around. This emphasised the critical significance of familial support in reducing the anxiety of new experiences and accessing healthcare services:
For my first time when I came here, I was coming for the first time for the pregnancy. So I did come with my sister. She was the one who knows everything here. So she’s the one who was showing me, go there, go there, go there. So, it was easier for me. [31-year-old female from Zimbabwe]
Another female participant described how the staff at the antenatal clinic taught her how to care for the baby, even though they used a language she did not understand, she would ask some of the mothers and they would translate for her. This facilitated understanding and fostered a sense of comfort and belonging in a foreign environment:
Like the time I was pregnant, you know when you are pregnant, they teach you how to raise the baby. They normally speak with your language so they advise that you must speak that language because you are here in South Africa, so you have to understand. So sometimes when they speak with your language, I ask someone. [Female 30year-old from Zimbabwe]
Traditional customs and cultural beliefs had a substantial impact on how people sought medical attention. Before using clinics or hospitals, some migrants indicated that they preferred spiritual or traditional healers, including sangomas. Although others acknowledged that they later sought professional healthcare when conventional ways failed, many saw these practices as strongly ingrained in their cultural identity:
When we had COVID, many preferred the steam (moulounge) instead of seeing the doctor. So it’s very important that it depends on one disease to another that led us to choose a traditional therapist or a doctor. [Male 38-year-old from Congo]
That’s what I believe in, sangomas and what, you know, it’s our culture, we do believe in those things. [Male 48-year-old from Malawi]
Many migrants’ lives were significantly impacted by their spiritual beliefs. Several individuals talked about how they relied on prayer and believed in divine intervention to deal with health issues. Religion frequently influenced their health seeking behaviour, but it did not completely discourage people from seeking medical assistance:
For church I do, I am a Christian, so I believe also in prayer that whenever you pray God changes the situation. [female 31-year-old from Malawi]
Self care practices also came across in most of the interviews with the migrants. They resorted to self-medication and private doctors instead of going to the clinic:
If I’ve got money. If I see maybe it’s headache, I go to pharmacy to buy some medicine. [39-year-old male from Zambia]
When my baby is sick I come to the clinic. But myself I go to the doctor. [26-year-old female from Mozambique ]
Normally I often go to the Congolese doctors’ clinics in Johannesburg, I have never had a problem there with them. [46-year-old male from Congo]
Health Care Experiences
Several participants were positive about the treatment they received. They received all the care and attention they needed with great empathy and understanding of some of their language barriers. The registration process was smooth. Some expressed their gratitude for being treated well and not differently because they were migrants. One even compared the treatment she received in South Africa to being the best, unlike her home country:
Just that the clinic are nice because when you go there you will get a treatment and unlike in my country, so I wish to stay here forever. [30-year-old female from Zimbabwe]
Well, honestly to me, I must say I’m grateful. I wouldn’t say that I’ve been treated like somehow, I don’t know, but I just thank God I’ve been treated well, like any person. There was no difference . . . I didn’t see any difference like because I just came or these are . . . the South Africans, I didn’t see the difference to me. [31-year-old female from Malawi]
I find the health services in SA to be of good quality but very scarce, that is why there are long queues everywhere. I notice that local native residents also go through the same system and experience the same frustrations. [34-year-old male from Mozambique]
Fear of being treated poorly or differently because of their migrant status led many to avoid healthcare facilities. Some feared being denied care or required to pay fees they could not afford. Others delayed seeking care until necessary, fearing bad experiences based on stories shared within their communities:
According to people’s expectations or experiences, I had a lot of questions that if I go there, how am I going to be treated there, what am I going to do, I’m a foreigner. I had a lot, yeah, a lot of them. I was even scared, especially there at Sebokeng, I was even scared because the other lady was telling me that she had a bad experience about Sebokeng, but so that’s why I was so scared. [Female 28-year-old from Zimbabwe]
Children were not immune to this atmosphere of division. A Zimbabwean woman described a painful encounter where her child was not allowed to play with a local child in the clinic’s waiting room after hearing that she spoke Shona:
She want to play with the baby but her mother, she don’t want my baby to play with that baby. I was feeling bad that day and I cry too much and I said, if it’s my it’s my baby’s date I can’t come again this side. [23-year-old female from Zimbabwe]
Some migrants were discriminated against and refused help by the health care professionals because of the way they looked, the way they were dressed, the way they talked and even the way they did their hair:
But they are not willing even to help just because maybe the way you look, even maybe the way you dress and then they say, something like that. [44-year-old male from Malawi]
A significant source of frustration was lengthy waiting times, and migrants were sometimes disriminated against and made to wait longer:
When they look at you, they feel like you are not from South Africa. So, they can leave you unattended until maybe they wish to say okay now we can help you and something like that. [44-year-old male from Malawi]
Another migrant in labour was seen and checked at 7 am and was never attended to again until 3 pm. She described her traumatic labour experience, highlighting the disregard she received from medical professionals. She felt abandoned, even though she had called for help several times when the personnel did not follow up with her following an initial assessment:
In the morning Thursday, I was having pains, and that sister was on the duty. I said, sister, may you please come to check me. She come and check me, then she said I’ve got 2cm. I said okay. My sister, it was the first and only last she checked me around 7am, the whole day. She didn’t come and check me. [31-year-old female from Zimbabwe]
Psychosocial and Emotional Effects
This theme explores the psychological, social and emotional effects of migrants’ experiences. It is critical to understand how these factors can impact health outcomes, behaviour and daily functioning.
Most of the migrants expressed having felt lonely and alienated, as they were far from home and most of them did not have families to support them. They missed their countries but there was nothing there to live for. They tried to fit into the community by learning their language but still, they felt like they did not belong:
Yeah, still I should say it’s not something like I’m comfortable enough here. Still, here and there, because you see, even if you learn . . . not Zulu or Sotho being not my mother tongue, somewhere somehow, they will really show that he is not from here. [44-year-old male from Malawi]
Migrants experienced stigma everywhere, at health facilities and in the communities in which they lived. They were referred to as foreigners and they were looked down on, and some people told their children not to play with their children as if they had a contagious virus. One woman recalled when a healthcare provider expressed her hatred for foreigners, and implied that they were the reason they were experiencing shortages of services like electricity and water, and if she had the power, she would send them back to their countries:
Then, there was a sister, I don’t know the name. She said, now I hate foreigners. We are struggling electricity, we are struggling water, it’s because of you. You are occupying everywhere. If I was the President, I was going to make a plan with each and every foreigner, it’s going to go back. [Female 31-year-old from Zimbabwe]
One mother’s experience of seeking medical help for her 4-month-old baby was overwhelming and distressing for her. She entered the facility feeling anxious and uncertain, as her child had developed a rash. Upon explaining her situation to the staff, she was met with dismissive remarks. They questioned her decision to bring such a small baby to the clinic leaving her feeling judged and unsupported. She was told to go back home and give her baby milk:
Then this lady, she said, ah, you must go back and give the baby milk, oh, that day, I was crying the whole day. [30-year-old female from Zimbabwe]
One migrant expressed that she experienced anxiety, frustration and a sense of helplessness, when she was asked to produce a transfer letter from her country before she could be assisted with her chronic treatment:
Yeah, at first I was like, because it was like just too much, like the stress would be like, how am I going to do this? I’m here already, I can’t go back home to get those things. But there at clinic, they need the transfer letter, so what am I going to do? [37-year-old female from Zimbabwe]
Discussion
Summary of Key Findings
The main factors influencing migrants’ access to and utilisation of public sector primary care are summarised in Figure 1. Factors are categorised into barriers to primary care, coping and support factors, healthcare experiences and psychological and emotional effects. Health care experiences were a mix, with some respondents reporting good quality and empathic care, while others reported having care denied or delayed.
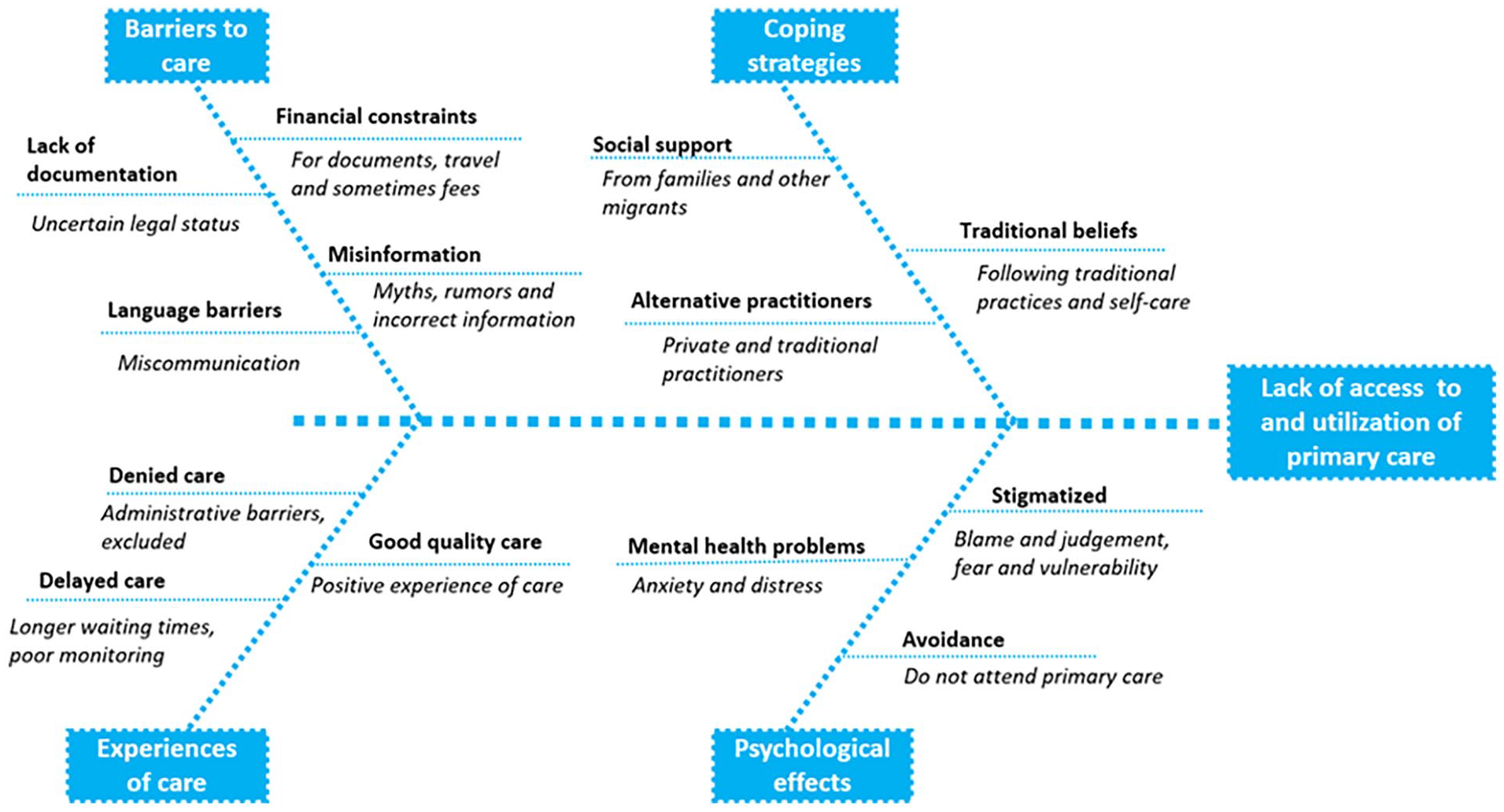
Summary of key findings.
Discussion of Key Findings
The absence of legal documents frequently presents significant obstacles for migrants seeking healthcare. 14 Undocumented migrants are sometimes denied services or required to pay excessive costs, even for basic care, which discourages them from seeking prompt medical help.14,15 This problem is made worse by the high expense of obtaining or renewing documentation, like work permits and passports, which further excludes people. 15 These difficulties draw attention to the systemic disparities in migrant patients’ access to healthcare. The Constitution of South Africa, the National Health Act and The Refugees Act all affirm that everyone, including refugees and asylum seekers with or without permits, have the right to access health care services, including primary care. 16 The Immigration Act in contradiction expects health care workers to report illegal foreigners to Home Affairs. 16
Communication is hampered by language barriers, which may lead to incorrect diagnosis or inadequate treatment. 17 To grasp medical advice, migrants frequently turn to interpreters or other patients, which can result in misinformation. 17 Enhancing trust in healthcare systems and reducing these problems may be possible with better access to multilingual services and interpreters. 17 Many migrants could not completely comprehend health-related material due to language limitations, which resulted in the dissemination of false information and incorrect interpretations of medical recommendations. The specifics of health education sessions or treatment plans given by medical professionals are frequently difficult for migrants to understand. 17 In addition, religious and cultural practices have a big impact on how migrants seek health care. 2 Many people delay access to official healthcare services by first using spiritual practices and traditional healers. 2
Economic constraints significantly influenced migrants’ access to healthcare, often hindering their ability to seek and receive adequate services. 2 Migrants frequently settle for low-paying jobs in industries such as construction, domestic work, agriculture or as shop attendants.2,18 These occupations subject them to lost wages when they take time off work to visit primary care centres.2,18 Due to these financial strains, migrants frequently choose not to receive essential medical care, which worsens their health outcomes.2,8 Access to services is further discouraged by unclear communication on costs, fear of deportation or discrimination at health facilities.7,14,15 Without financial and legal assurances, care may not be truly accessible, even when it is technically available. 14
Migrants with permanent or temporary residence or anyone from the SADC region should be means tested at public sector health facilities in the same way as South African citizens. 16 There are documented examples of state facilities demanding prior payment, even for medical emergencies, and this reveals a gap between official policy and lived experience.14,15
Discrimination is still a major problem, with migrants frequently facing unfavourable opinions and unfair treatment in medical institutions.8,14,15 Xenophobia and stigma, such as being held responsible for resource shortages, make people feel alienated and deter migrants from getting care.8,14 Fostering inclusive healthcare environments requires anti-discrimination training and policies that support equity. 19 The primary care experiences of migrants differed greatly. Some experienced long waiting times and neglect, especially during emergencies, while others reported excellent interactions characterised by empathy and prompt assistance. These conflicting experiences highlight the necessity of patient-centred treatment and consistent quality. 18
Strengths and Limitations
Migrants came from various backgrounds, age ranges and nationalities, which enhanced the study by offering a broad range of viewpoints. The research offers an in-depth insight into the socio-cultural elements impacting healthcare access by examining communication challenges, cultural traditions and the significance of social support networks. This study looked beyond just clinical or logistical obstacles to explore the intricate connection between culture, language and healthcare encounters.
Migrants who were more open to sharing their healthcare experiences may not accurately reflect the larger migrant community. For example, undocumented migrants living in severe poverty, who are especially marginalised, may have been less inclined to take part. Their specific struggles might have been missed. Nevertheless, the findings are likely transferable to similar public sector primary care sectors in Gauteng and other parts of South Africa.
Language barriers could have impacted the data collection process. Individuals who lacked fluency in the interview languages (English, French or Portuguese) may not have been able to effectively convey their experiences. Participants’ recollections of healthcare encounters may not be precise, resulting in potential over- or under-reporting of important challenges or positive experiences.
Even though the migrants were interviewed during the weekends with the interviewer wearing casual clothes, they were still conducted in a healthcare facility which might have made the migrants feel intimidated and more cautious.
Recommendations
District health services should adopt migrant-inclusive policies to ensure equitable healthcare access. Streamlining registration processes, reducing reliance on legal documents and addressing discriminatory practices will improve outcomes and reduce emergency care strain. Current contradictory policies require alignment to enhance consistency.
Adequate resourcing is critical for facilities in high-migrant areas, including funds for translation services. Collecting information on migrant healthcare needs will inform targeted service adjustments and policy changes.
Healthcare managers should implement continuous education programmes on cultural competence, empathy and migrants’ legal rights. This includes language training and strategies to address deportation fears and systemic inequities. Managers must be accountable for improving intake processes, reducing wait times and ensuring equitable patient treatment.
Collaborating with non-government organisations and community groups can bridge gaps in culturally and linguistically appropriate care. Healthcare workers need training in cultural sensitivity and how to address language barriers. Using interpreters, communication aids or technology-driven translation tools are essential for accurate and empathetic care. Reducing stigma and discrimination is critical. All migrants require compassionate care to encourage timely healthcare-seeking behaviour and reduce misinformation.
Migrant organisations should advocate for equitable healthcare policies and collaborate with NGOs and healthcare providers to address systemic barriers. Creating support networks and peer programmes can assist with language interpretation, understanding procedures and navigating healthcare systems. Educating migrants about their healthcare rights and services will enable informed decision-making and reduce misinformation.
Research should expand to include undocumented migrants and those living in informal settlements, utilising both qualitative and quantitative methods. Longitudinal studies can track changes in healthcare access and outcomes over time. Intervention-based research is crucial to evaluate strategies like language programmes, policy reforms and healthcare training to reduce barriers and improve migrant healthcare access.
Conclusions
In Emfuleni, South Africa, migrants still experience inequitable access to primary care which limits the attainment of UHC. Barriers to care include uncertain documentation and legal status, financial constraints, misinformation and language barriers that lead to miscommunication. Migrants cope by support from family and other migrants and by turning to traditional beliefs and practitioners. Although some migrants report good quality of care and positive experiences others report discrimination by being denied care or having care delayed. As a result of their experiences migrants may feel stigmatised, anxious or distressed and may avoid future contact with primary care services. Migrant-inclusive health services should attend to the issues through clear policy and protocols, training of health professionals, translation services and clear messaging regarding the rights to health care.
Footnotes
Acknowledgements
Thanks to Dr Victor Figueroa a medical doctor and family physician and an honorary lecturer for the University of Witwatersrand’s Family Medicine department. He conducted and translated the Portuguese interviews. Thanks to Prof Ilse Ruyssen from Ghent University for her advice and feedback during the research study.
Ethical Considerations
Ethical approval was given by the Health Research Ethics Committee at Stellenbosch University (S23/07/166).
Consent to Participate
All participants gave written informed consent.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Flemish Interuniversity Council (VLIR-UOS) TEAMS Grant (ZA2022TEA526A103)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data may be available on reasonable request to the authors.