
Abstract
Background:
Chronic nonspecific low back pain (CNLBP) is a prevalent, disabling condition worldwide. Tuina, a traditional Chinese manual therapy, has shown potential benefits, but evidence remains limited.
Objective:
This study evaluated the effectiveness and safety of Tuina therapy in managing CNLBP in a U.S. population.
Methods:
A prospective, single-blind, randomized controlled trial was conducted at Mayo Clinic Rochester campus (February 2020-April 2024). 204 participants with CNLBP were randomized into 3 groups: Tuina (N = 68), physical therapy (N = 68), or a combination of both (N = 68). Each group received 6 treatments over 2 months. The primary outcome was pain intensity (VAS); secondary outcomes included disability (ODI), quality of life (SF-36), and adverse events. Additionally, participants completed a satisfaction survey at the end of the trial. Research Electronic Data Capture (REDCap) was used for survey data collection. Data was assessed by analysis of variance (ANOVA) for the multiple repeated measurements, Kruskal-Wallis tests, while Chi-square tests, and Bonferroni correction in SAS software.
Results:
185 subjects completed the study. Significant decreases in VAS, ODI, and SF-36 Overall Physical scores were found from baseline, to post treatment and follow-up in all groups (P < .05), while there were no significant differences in VAS, ODI, or SF-36 outcomes between the Tuina group and the other 2 groups. There were 4 adverse events observed in the trial, 1 in the Physical therapy group and 3 in the Mixed group. Only 1 transient low back pain after Tuina therapy was observed in the Mixed group but did not require treatment. The high percentage of patients who received the Tuina program was extremely helpful (n = 94/126, 77.0%). The willingness to recommend was significantly higher for Tuina compared to physical therapy (Mixed group [N = 59/62, 95.2%], Tuina group [N = 57/64, 91.9%], and physical therapy group [N = 31/59, 59.6%] (P < .05).
Conclusion:
Tuina therapy showed comparable benefits to physical therapy and combined treatment of both in improving pain, function, and quality of life in patients with CNLBP. With high patient satisfaction and a favorable safety profile, Tuina appears to be a safe and acceptable non-invasive treatment option. Further studies are needed to validate these findings in the future.
Background
Chronic nonspecific low back pain (CNLBP) is a prevalent and often disabling disorder characterized by persistent lower back pain without a specific underlying pathology identifiable through conventional diagnostic methods. It typically lasts longer than 12 weeks and is not attributable to a known cause, thereby complicating effective management strategies. 1
CNLBP is a major cause of work absenteeism and long-term disability, contributing to significant healthcare costs and loss of productivity. 2 Epidemiological studies estimate that about 60% of adults experience CNLBP in their life time. 3 According to World Health Organization, in 2020, low back pain affected 619 million people worldwide and it is expected that the case number will increase to 843 million by 2050, mainly due to population expansion and aging. 4 In the United States, the total annual cost of managing low back pain exceeds $100 billion, with a substantial portion mainly attributed to indirect expenses such as lost wages and reduced productivity. 5 Addressing this public health challenge requires comprehensive and multidisciplinary approaches to enhance patient outcomes and reduce the overall burden on society.
Physical therapy is commonly used in the management of CNLBP. It encompasses a range of techniques, including exercise therapy, manual therapy, and patient education, aimed at reducing pain and improving function. Physical therapy has a robust evidence base supporting its effectiveness, and it is often recommended as a first-line treatment for CNLBP by clinical guidelines. Despite its benefits, physical therapy may not be always effective for all patients.6,7 In a 2018 review, Cuenca-Martínez et al 7 evaluated the effectiveness of traditional physiotherapy in the management of CNLBP, they found it to be largely ineffective. This highlights the need for more comprehensive, multidimensional research to improve treatment strategies. Therefore, there is increasing interest in more complementary and alternative therapies to enhance treatment outcomes.
Tuina, a traditional Chinese therapeutic massage technique, involves various manual techniques such as kneading, rolling, pressing, and stretching to stimulate acupuncture points, meridians, and soft tissues. 8 Tuina has gained increasing recognition for its potential benefits in managing chronic low back pain. Despite its growing popularity and anecdotal reports of effectiveness, the scientific evidence supporting Tuina remains limited.9,10 Some clinical studies and systematic reviews have shown positive outcomes, suggesting that Tuina can effectively alleviate pain and improve functional outcomes in patients with CNLBP. However, the overall quality of the evidence is low, and further rigorous studies are needed to fully determine its efficacy and mechanism of action.9,10
Although CNLBP is highly prevalent and various interventions are recommended in clinical practice, to our knowledge, no previous, scientifically rigorous randomized controlled trials (RCTs) have specifically examined the combined effects of physical therapy and Tuina on CNLBP patients in the USA. The systematic review in 2023 examined previous RCTs on the effects of physical therapy and Tuina in patients with CNLBP, however, the applicability of these study results is constrained by methodological limitations, high heterogeneity, and small sample size. 9 This present study was designed collaboratively with clinicians and scientists from the Jinan University, Guangzhou, China, and Singapore General Hospital, Singapore as a large-scale, single-blinded RCT. Each of the 3 sites (China, Singapore, and USA) conducted a clinical trial following the co-developed protocol, independent of the other 2 sites. This allowed for differences in clinical practices (e.g., physical therapy) while maintaining fidelity to the treatment intervention. Therefore, the present trial was conducted to assess the effectiveness of Tuina compared to physical therapy on U.S. patients with CNLBP. In addition, this study also explored the effectiveness of Tuina combined with physical therapy as an intervention modality for CNLBP, comparing it with Tuina and PT management alone. Within this article we report on the finding from the clinical trial conducted in the United States site only.
Methods
Study Design and Setting
This study was a prospective, randomized, controlled trial conducted with a blinded assessor at Mayo Clinic Rochester campus from February 2020 to April 2024. The protocol was created via a collaborative effort involving clinicians and researchers from Mayo Clinic, Singapore General Hospital and Jinan University, Guangzhou, China.
Participants
Potential participants were recruited through advertising posted on an employee intranet site, as well as referrals from clinical providers. Additional outreach included promotion in community centers, local clinics, and on social media platforms. Names of interested individuals meeting the screening criteria were forwarded to the principal investigator, who reviewed medical records and determined eligibility. Those individuals meeting all the inclusion and exclusion criteria were invited to participate and were consented for the study. Enrollment took place from March 18, 2021, to August 21, 2023. Study participation concluded on January 27, 2024.
Inclusion Criteria
Those who meet the following criteria are eligible to participate in the study. The specific diagnostic criteria for CNLBP are as follows:
(1) Pain and discomfort of unknown etiology between the costal margins and inferior gluteal folds with or without referred pain to the lower limbs), lasting for more than 12 weeks (measured by patient past history and lumbar physical exam).
(2) There may be waist muscle weakness, stiffness, limited mobility, or reduced spinal coordination. The symptoms of pain are lessened or disappeared after bed rest. While the symptoms of pain are aggravated after bending over, sedentary, or standing for a long time (measured by patient past history and lumbar physical exam).
(3) Physical examination showing an increase in muscle tension or a significant localized tenderness point (trigger point) in the painful area, with negative straight leg raising test, and no signs of nerve root lesions.
(4) Patients with Radiographic results of MRI, CT, and X-ray within 1 year. If a potential candidate may be eligible, but imaging within 1 year is not available, the study will fund a screening lumbar x-ray which will be reviewed for eligibility by Dr. Bauer or Dr. Brault.
(5) Female patients who are of childbearing potential and are likely to become pregnant during the treatment phrase must have a negative pregnancy test (human chorionic gonadotropin (HCG) urine test).
Exclusion Criteria
Those who meet any of the below exclusion Criteria shall be excluded from the study.
(1) Patients with low back pain associated with nerve root compromise (measured by patient past history, clinical examination of dermatomes, myotomes, and reflexes).
(2) Patients with severe skin diseases (e.g., skin cancer, erysipelas, severe eczema, severe dermatitis, severe psoriasis, and severe hives lupus) (measured by patient past history and lumbar physical exam).
(3) Serious spinal pathologies such as fractures, tumors, inflammatory, and infectious diseases (measured by patient history and lumbar physical exam).
(4) History of Lumbar Spine Surgery (measured by patient history).
(5) Serious cardiovascular or metabolic disorders, such as heart failure, severe osteoporosis (measured by patient history).
(6) Patients are diagnosed with cognitive issues such as major depression, and moderate to severe dementia, severe psychiatric diseases (such as schizophrenia, bipolar affective disorder, paranoid psychosis) (measured by patient history).
(7) Women who are pregnant, or who are of childbearing potential and are likely to become pregnant during the treatment phase but are not willing to use a reliable form of contraception, will also be excluded. Reliable forms of contraception include oral contraception, diaphragm or condom (with spermicide), injections, intrauterine devices, surgical sterilization, and abstinence.
Suspension Criteria
Subjects may discontinue from the study if he/she decides to stop at any time, for the following reasons:
(1) The subject has any adverse reaction to the intervention such as broken skin, bleeding and seldom syncope, fractures, etc.
(2) The subject wishes to withdraw from clinical study.
(3) The subject wishes to attend other interventions, which may create a bias result in the study, such as attending chiropractic or other massage therapy or non-traditional spinal treatment.
Those who meet any of the above suspension criteria shall be suspended, however all subjects’ responses will be recorded to determine reasons for suspension from the study.
After signing consent, subjects completed baseline assessments, including questionnaires, urine pregnancy test (females of childbearing potential only), and lumbar spine x-ray, if previous lumbar spine x-ray had not been completed within the past year. X-ray and pregnancy tests were reviewed for eligibility by the study Principal Investigator. All participants completed a baseline spinal range of motion (ROM) measurement and traditional Chinese medicine patterns. (An analysis of the traditional Chinese medicine scores derived from this assessment will be reported separately in a future manuscript.) Participants who did not meet the eligibility criteria or declined to provide consent were not enrolled in the study. Their screening information was recorded for documentation purposes, but they did not take part in any study activities.
Randomization, Allocation, and Concealment
Eligible participants were randomly assigned in a 1:1:1 ratio to receive Tuina (Tuina group), physical therapy (Physical therapy group), or a combination of the 2 treatments (Mixed group) using computer-generated block randomization through a web-based block randomization system (Research Electronic Data Capture [REDCap]). The randomization sequence was generated by an independent statistician not involved in the trial, using SAS software (version 9.4; SAS Institute Inc.). All data entered REDCap were password-protected, with access restricted to authorized investigators. System access was monitored and logged to ensure data security. Allocation concealment was maintained using sequentially numbered, opaque sealed envelopes.
Sample Size
The sample size was determined based on the anticipated mean difference in the Visual Analogue Scale (VAS) score 11 for CNLBP between the experimental and control groups. Referring to a prior similar pilot study, 12 the mean (SD) differences in VAS scores before and after treatment were 1.9 (0.9) for the Tuina group, 1.4 (0.8) for the Mixed group, and 1.4 (0.85) for the Physical therapy group. The within-group standard deviation (SD) was assumed to be consistent across groups. A pooled SD of 0.85 across groups (0.9^2 + 0.8^2)^0.5 is used. This resulted in a required sample size of 57 participants per group to achieve a level of 0.8, assuming a significance level of α = 0.05 (2-sided), leading to a total of 171 participants. To account for a potential 15% dropout rate, the sample size number was increased to 68 participants per group, totaling 204 participants. Outcome assessors were blinded to the participants’ assigned treatment groups to ensure unbiased assessment.
Blinding
To ensure unbiased outcome assessment, the study assessor responsible for evaluating outcomes and entering data into the case report forms was blinded to the random allocation, as blinding participants or practitioners was not feasible due to the treatment’s nature. An independent statistician, who was also blinded to the identities of the treatment groups, conducted the statistical analysis.
Statistical Analysis
Demographic characteristics were reported for the 3 treatment groups with either mean and standard deviation for continuous variables or percentages for categorical variables. The mean and standard deviation of the outcome scores is reported at the pre, post, and follow-up time points. Kruskal-Wallis tests were utilized to compare differences between groups for continuous variables, while Chi-square tests were used to compare groups for categorical variables. A repeated measures ANOVA model was used to look at differences between groups and over time for the outcomes of interest. The ANOVA model included group (Tuina, Physical therapy, Mixed), time point (Pre, Post, and Follow-up), and the interaction between group and time. P-values for the between subject value (group), within subject value (time), and interaction term are reported. Comparisons across groups were performed using ANOVA with P-value less than 0.05 considered statistically significant. When the overall comparison was found to be statistically significant, subsequent pairwise comparisons were performed with a Bonferroni correction used to account for multiple testing. Analyses were completed in SAS (SAS Institute Inc., version 9.4).
Study Interventions
Tuina
Tuina was conducted by trained and experienced TCM practitioners. The selected Tuina techniques applied are as follows:
1) Enhancing the flow through energy channels: Applying rolling techniques from the lower back to the legs (10 min).
2) Pushing on the back and lumbosacral region: Applying palm pushing techniques along with the Governor Vessel from the upper back to the lower back and sacral area (2 min).
3) Plucking to relieve spasms: Utilizing bilateral large thenar plucking techniques along the erector spinae muscles of the back and lumbosacral region (4 min).
4) Pressing certain acupoints to mitigate pain: Applying firm pressure to specific acupoints on the back, lumbosacral, and leg regions—selected based on syndrome differentiation—until the patient experiences sensations of soreness and distention, to alleviate pain (6 min).
5) Applying assisted with traction to the lower lumbar spine: Grasping the patient’s ankles with both hands and gradually increasing the pulling force (1 min).
6) Performing a spinal adjustment to enhance joint alignment and improve spinal function: gently twisting the patient’s waist by applying controlled pressure to the shoulder and opposite hip, moving slightly beyond the point of resistance in a rocking motion (2 min).
7) Twisting the lower back to relax the lumbar muscles: With the subject lying supine and knees drawn toward the chest, the practitioner holds the knees together with 1 hand and supports the heels with the other, gently rotating the lower extremities clockwise and counterclockwise 3 to 5 times to mobilize the lumbar regio (1 min).
8) Scrubbing the back and lumbosacral region: using the thenar and hypothenar base of the palm to scrub along both sides of the Bladder Meridian on the back and lumbosacral area. Transverse scrubbing is applied to the lumbosacral region until a warm local sensation is achieved (3 min).
9) Concluding the treatment with rhythmic patting: applying steady percussive taps to the lower back, lumbosacral region, buttocks, and lower limbs (1 min).
Physical Therapy
Physical therapy was conducted by licensed Physiotherapists with at least 1 year of experience in managing low back pain. The treatment protocol included:
1) Assessment: Comprehensive evaluation of the subject’s condition.
2) Education: Providing advice on ergonomic postures and positions for work, home, and daily activities to support ongoing therapy post-treatment.
3) Manual therapy: Utilizing manipulative techniques to alleviate discomfort in the lower back.
4) Aerobic exercise: Instructing patients to engage in aerobic activities independently as part of a home exercise regimen.
5) Flexibility and core-strength exercises: Developing a personalized program of exercises and soft tissue stretches aimed at strengthening the core muscles supporting the spine and surrounding tissues.
Tuina Combined with Physical therapy
Three sessions of Physical therapy and 3 sessions of Tuina were provided within a 2-month period.
Participants in all 3 study groups received therapy once a week or every other week based on their individual needs, with each session lasting between 30 and 60 min, for a total of 6 sessions spread out over a 2-month period.
Outcomes
Baseline demographic data, physical examination findings, and all outcome measures were assessed by an evaluator blinded to treatment allocation. Data collection for the trial group was conducted at baseline, after 2-month treatment, and 3-month follow-up, totaling 3 measurement points. Survey data were collected using the REDCap system.
Primary Outcome
The primary outcome was the intensity of lower back pain as rated by VAS pain score between 0 (no pain) and 100 (worst possible pain). Participants were instructed to mark their perceived pain level on a 10-centimeter horizontal line, scored from 0 to 10, using circular markers both before and after the intervention. VAS is a validated tool known for its high test-retest reliability. 13
Secondary Outcomes
The secondary outcomes included the Oswestry Disability Index (ODI), 36 Item Short Form (SF-36), Safety and Satisfaction. The evaluation of disability was made based on Oswestry Disability Index (ODI), 14 a condition-specific tool consisting of 10 questions that assess pain, personal care and daily activities, and each question is described on a 6- score scale ranging a score from 0 means no pain to 5 means worst pain, with a total possible score ranging from 0 to 50 scores. The higher score indicates a higher level of functional disability. The participants’ health status was measured with Short Form 36 (SF-36), which ranges from 0 to 100, with a lower score indicating greater level of functional disability. The questionnaire is a multidimensional multi-item scale containing sections on physical functioning (PF), role physical (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role emotional (RE), mental health (MH), and health transition (HT). SF-36 scoring method yields 8 scale scores with physical component summary (PCS) and mental component summary (MCS). 15 Satisfaction was assessed using a survey questionnaire, “Would you recommend this treatment to family members or friends?”, and participants who experienced Tuina therapy also answered, “Overall I would rate Tuina program as, n (%).” Safety outcomes were evaluated by and noted through the whole trial. Compliance and adherence were evaluated by the rate of treatment attendance.
Results
Of the 822 participants who expressed interest in the study, 204 consented and were enrolled. Among the enrolled, 3 were excluded as screen failures due to ineligible x-rays (2) and potential for injury if randomized to Tuina (1). A total of 201 went on to be accrued to the study. Among the 201 accrued to the study, 16 withdrew from the study for various reasons: 4 dropouts from the Tuina group (1 pregnancy, 2 working location change, and 1 chiropractic therapy), 4 dropouts from the Mixed group (1 lack of transportation, 1 child medical visits, 1 chiropractic therapy, and 1 felt Tuina was not helping), and 8 dropouts from the physical therapy (2 felt physical therapy was not helping, 1 felt disappointed without Tuina therapy, 2 discontinued intervention due to family death, 2 chiropractice, and 1 busy schedule). Therefore, the study sample consisted of a total of 185 participants (Tuina group = 64, Physical therapy group = 59, and Mixed group = 62), including 137 female (74.1%), 47 males (25.4%), and 1 sex unknown (0.5%) were enrolled in the study. A flow chart detailing participant inclusion is presented in Figure 1.

Flow chart.
VAS Score
Baseline VAS scores of Tuina group, Physical therapy group and Mixed group were 3.5 (1.9), 3.1 (1.7), and 3.4 (2.2), respectively, showing homogeneity (P > .05) (Table 2). According to our findings, there was a significant decrease in VAS scores from baseline, to post treatment and follow-up in all groups (P < .001). The greatest decrease was observed in the Tuina group. There was no significant difference between the 3 groups or the interaction between group and time (P > .05).
ODI Score
Baseline ODI scores of Tuina group, Physical therapy group and Mixed group were 20.7 (8.6), 16.4 (7.9), and 21.8 (10.4), respectively, showing homogeneity (P > .05). The ODI outcomes decreased for all 3 treatment groups significantly. The greatest decrease was observed in the Mixed group. No significant difference was found between the 3 groups (P > .05). For the ODI outcome, both time and the interaction showed a statistically significant difference (P < .05).
The SF-36 Survey
The SF-36 survey was split into 2 overall outcomes—mental and physical scores. For the overall physical score there was a highly significant change in time (P < .001), with scores decreasing from baseline for all groups (P < .05). For the overall mental scores there was significant interaction between time and treatment group (P < .05). The Mixed treatment group had the biggest change, with an increase in score between baseline and post time points (Tables 1 and 2).
Demographics.
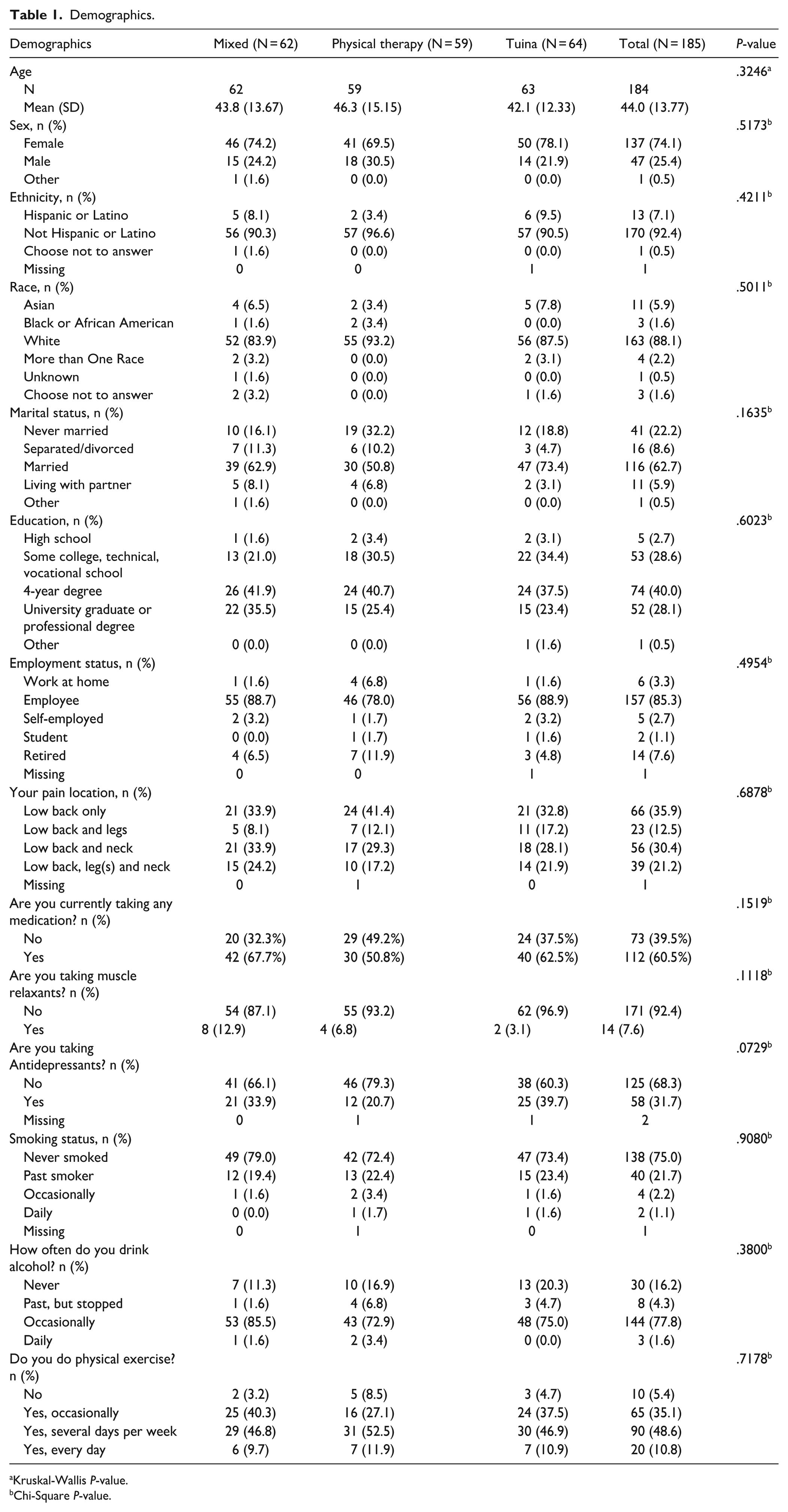
Kruskal-Wallis P-value.
Chi-Square P-value.
Survey Outcomes.

Results from repeated measures ANOVA interaction between group and time.
Results from repeated measures ANOVA group differences.
Results from repeated measures ANOVA time differences.
End of Study Satisfaction Survey
End of study satisfaction survey was reported in Table 3. A significant difference in the number of subjects who said they would recommend Tuina treatment to family or friends was found in the Mixed group (n = 59/62, 95.2%), Tuina group (n = 57/64, 91.9%), and Physical therapy group (n = 31/59, 59.6%). A high percentage of patients who received Tuina rate Tuina program as extremely helpful (n = 94/126, 77.0%) (Table 3).
End of Study Satisfaction Survey—Recommend.

Chi-Square P-value.

Safety and Compliance
In addition, 4 adverse events (AEs) were reported during the trial: 1 hip fracture after baseline in the Physical therapy group; 1 back pain resulting from playing volleyball, 1 cholecystectomy, and 1 instance of transient low back pain following the second Tuina session in the Mixed group. No serious AEs were reported in this trial. The dropout rates were 5.9% in the Tuina group, 6.1% in the Mixed group, and 12.0% in the Physical Therapy group.
Discussion
Tuina is frequently used to manage chronic low back pain, though the specific mechanisms underlying its therapeutic effects remain unclear. Research indicates that its efficacy may be related to the regulation of tissue plasminogen activator and plasminogen activator inhibitor-1 levels, as well as its potential to alleviate sciatic nerve crush injuries.16,17 The World Health Organization (WHO) has endorsed massage as a first-line, non-surgical treatment for chronic primary low back pain in adults in primary and community care settings. 18 However, additional high-quality evidence is needed to clarify Tuina’s effectiveness and underlying mechanisms.
This is the first study to evaluate the effect of Tuina for patients with CNLBP among populations in U.S.A. This study evaluated the effect of Tuina in patients with CNLBP compared to physical therapy and a combination of both treatments. The study findings showed significant improvements in VAS for pain intensity, ODI for daily functional disabilities and SF-36 overall physical scores across all 3 groups from baseline. However, when comparing the 3 groups, there was no significant difference found between Tuina and the other groups for any of the outcomes. Notably, AEs associated with Tuina therapy were few and minimal, and participant satisfaction was higher with Tuina. Overall, these findings suggest that Tuina could be a valuable non-invasive alternative or adjunct treatment for CNLBP. The results in this study are in line with previous reports indicating that massage can reduce symptoms of pain and functional disabilities of patients with chronic LBP only in the short-term follow-up. 19
Given the widespread prevalence of CNLBP and the significant social and economic burden associated with it, effective management is a priority. Massage therapy has been widely recommended as a treatment option for CNLBP and is generally associated with high satisfaction among patients. The fact that the Tuina treatment includes a substantial component of massage may partly account for the high compliance and adherence observed in this trial. 20 The low dropout rate and high participant satisfaction in our study are key findings, as patient engagement with treatment recommendations may play a significant role in long term adherence and recovery.
Adherence to treatment regimens is crucial for effective management of chronic low back pain, yet patient adherence tends to be low. 21 In this study, the Physical therapy group experienced a relatively high drop-out rate, resulting in a lower number of participants, which may have introduced bias into the experimental results. Interestingly, while both Tuina and physical therapy produced statistically significant pain reduction, participants showed a strong preference for Tuina, as reflected in their willingness to recommend it. Several factors may contribute to this preference. First, Tuina remains relatively novel in the United States, which may have sparked curiosity and led to a more favorable impression. Second, many participants had likely undergone physical therapy in the past, which may have influenced their expectations if they were randomized to that group. Furthermore, the Tuina protocol in this study incorporated a variety of techniques, which increased physical contact and more dynamic manipulation of muscles and fascia and thus may have been perceived as a more “active” form of therapy. The extended hands-on time and human touch involved in Tuina may also have contributed to its favorable reception among participants.
This trial did have several limitations. A primary limitation was the limited participant enrollment pool. While recruitment efforts included advertisements on an employee intranet site and referrals from clinical providers, additional outreach through community centers, local clinics, and social media may have introduced selection bias. Individuals who responded to advertisements and were referred to might differ systematically from the general population, potentially being more motivated, health-conscious, or having specific health concerns, thus possibly limiting the generalizability of the findings. Second, the study used a per protocol analysis, including only participants who completed the assigned intervention and outcome assessments. This was necessary due to the small sample size, participant dropouts, and interruptions in treatment delivery. While this approach allowed for evaluation of treatment efficacy among adherent participants, it might have introduced bias and reduced external validity. Although most AEs were unrelated to the intervention and did not result in withdrawal, this lack of analysis remains a limitation. In addition, no comparative analysis was conducted between completers and dropouts due to the small number of dropouts and incomplete data, limiting the assessment of potential attrition bias. Lastly, standard physical therapy, which includes manual techniques, was used as a control, potentially underestimating the specific effects of Tuina. Further studies should employ intention-to-treat analysis and include dropout comparisons to strengthen the validity and generalizability of the findings in the future.
Conclusion
This randomized controlled trial found that Tuina therapy offered comparable improvements in pain intensity, functional status, and quality of life for patients with CNLBP when compared to standard physical therapy or a combination of both therapies. Although no significant differences were observed among the treatment groups, patient satisfaction and recommendation with Tuina was notably high, and AEs were minimal and non-serious, supporting its potential as a safe and acceptable non-invasive treatment option.
However, the study’s findings should be interpreted with caution due to several limitations, including a limited participant pool, use of per protocol analysis, limited enrollment, treatment disruptions, the absence of a dropout comparison, and the use of standard physical therapy—which includes manual techniques—as the control condition. Future studies should address these issues to better evaluate Tuina’s clinical effectiveness in managing patients with CNLBP.
Footnotes
Acknowledgements
We would like to express our gratitude to The HEAD Foundation, Singapore, for their financial support of Dr. Bauer.
Ethical Considerations
This study was approved by the Ethics Committee of Mayo Clinic (IRB#20-003549) on July 10, 2020. All participants provided written informed consent prior to enrolment in the study. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Author Contributions
BKT, BAB, JXC, and CTIC conceived the research. BKT, BAB, JXC, CTIC, JY, XZ, and QYM designed the study. BAB and JSB performed the investigation. JNS recruited patients and served as study coordinators. JY, AD, and MAJ performed the intervention. MJM, SEB, and JJC were involved in data acquisition. BAB supervised the study. ITC and KMF conducted analysis and interpretation of data. BAB and JY wrote the original draft. All the authors revised and edited the manuscript. All authors approved the final version of the manuscript for publication.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the HEAD Foundation, Singapore.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Requests for access to the data in this trial may be directed to the corresponding author.