
Abstract
Introduction:
The coronavirus disease 2019 (COVID-19) pandemic disrupted healthcare systems and increased the need for home healthcare. This study examined how the pandemic influenced the characteristics and outcomes of newly initiated physician-led home visit care in Japan, particularly focusing on patients with cancer.
Methods:
We conducted a multicenter retrospective study using medical records from 6 home care clinics and hospitals in Ibaraki Prefecture, Japan. Patients who began physician-led home visit care between April 2019 and March 2023 were included. We compared patient characteristics, care duration, and outcomes between the pre-pandemic (April 2019 to March 2020) and pandemic (April 2020 to March 2023) periods. To examine changes before and during the pandemic, we conducted logistic regression analysis using the pandemic indicator as the exposure and home death within 1, 3, and 6 months as the outcome, adjusting for patient factors. We also examined the interaction between cancer status and the pandemic period.
Results:
A total of 1922 patients were included. The number of patients initiating home visit care slightly increased after the onset of the COVID-19 pandemic. The proportion of patients with cancer significantly increased during the pandemic (pre-pandemic: 37.5% vs. during-pandemic: 43.0%, P = .046). Home deaths within 1 month significantly increased during the pandemic compared to the pre-pandemic period (odds ratio (OR) [95% confidence interval (CI)]: 1.87 [1.33-2.63]). However, in the model including the interaction term, the main effect of the pandemic indicator alone disappeared, while the interaction between cancer and the pandemic showed a strong association with home death (OR [95% CI]: 9.33 [5.29-16.47]). Similar results were observed for home deaths within 3 and 6 months.
Conclusions:
Our findings suggest that home visit clinics adapted to the increased demands for home-based end-of-life care, particularly for patients with cancer during the pandemic. These findings highlight the need for strategic support and resource planning to manage surges in home-based care during health crisis.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has caused significant disruptions in healthcare services. Demand for home healthcare has increased in countries such as the United States, France, and Spain, driven by hospital bed shortages, infection control measures, and advances in telemedicine.1 -3 This shift in care delivery has also been associated with a rise in home deaths. A previous systematic review reported that, among 29 countries examined, 23—including the United States, the United Kingdom, and France—experienced an increase in home deaths during the COVID-19 pandemic. 4
In Japan, despite relatively low COVID-19 mortality, 5 hospital bed shortages and staff limitations led to a healthcare crisis. 6 Strict visitor restrictions at hospitals and care facilities also prompted changes in home healthcare use. 7 In this context, previous studies suggested increases in home deaths and requests for physician-led home visit care during the pandemic.8 -12 Unlike in many other countries where home healthcare is primarily delivered by nurses or multidisciplinary teams, home-visit care in Japan is predominantly provided by physicians. “Physician-led home visit care” refers to regular, scheduled visits to patients’ homes conducted directly by physicians. Under this model, physicians not only offer routine medical care but also play a central role in providing end-of-life care at home. Therefore, documenting the changes on these visit patterns is essential for assessing the workload imposed on home-visit physicians during the pandemic.
However, previous studies have only shown overall trends without detailing patient backgrounds, care duration, or household situations. In particular, patients with and without cancer differ substantially in disease trajectory, prognostic predictability, and the type of care, making it essential to compare these 2 groups separately. Indeed, patients with cancer are often reported to experience a more predictable decline, which facilitates advance care planning and decision-making regarding the preferred place of death, including the option to die at home. 13 However, previous studies have not examined whether pandemic-related changes differed by cancer status. Moreover, information on family caregivers, who often face significant burdens, is not captured in previous studies.
To address this knowledge gap, this study aimed to clarify the characteristics, care duration, and outcomes of patients who newly started physician-led home visits before and during the pandemic, including household and caregiver information. We also performed a more detailed analysis by categorizing patients into cancer and non-cancer groups. This study will provide a more nuanced understanding of how the pandemic has affected home healthcare in Japan. The findings offer valuable insights for healthcare planning, resource allocation, and improving coordination between home and hospital care in future crises.
Methods
Home Healthcare and Long-Term Care in Japan
In Japan, home healthcare refers to physicians conducting regular home visits, which are reimbursed under a health insurance scheme. 14 Physician-led home visits are initiated for patients unable to attend outpatient clinics. These patients may have previously received outpatient care at the same facility or been referred from other medical institutions. Physicians are required to make regular home visits, typically once or twice a month, depending on the patient’s medical condition. These patients often also use home-visit nursing care and home help services. According to the Ministry of Health, Labour and Welfare (MHLW), physician-led home visit care serves 4 main roles: supporting hospital discharge, providing daily and palliative care, responding to emergencies, and delivering end-of-life care. 15
In addition to health insurance, Japan introduced a mandatory long-term care insurance system in 2000. 16 It covers all citizens aged ≥65 and those aged 40 to 64 with age-related conditions. Services are provided based on a standardized certification system, with care levels ranging from mild (support levels 1-2) to severe (care levels 1-5), assessed by physical and cognitive function.17,18
Study Design, Setting, and Participants
This study was a multicenter retrospective analysis utilizing medical records from 6 enhanced Home Care Support Clinics/Hospitals (HCSCs) in the Ibaraki prefecture. Enhanced HCSCs are clinics or hospitals that play a pivotal role in delivering home healthcare, meeting specific criteria, such as providing a 24-h home visit system upon patient request and employing at least 3 full-time physicians.15,19 Ibaraki prefecture is characterized by a relatively small number and uneven distribution of physicians.20,21 The study participants were patients who initiated physician-led home visits between April 2019 and March 2023. Exclusion criteria encompassed patients under 18 years of age, those residing in facilities, and patients who received only end-of-life home visits without prior care. In this study, we extracted data only for patients who met all inclusion and exclusion criteria at the time of data extraction. Therefore, there was no stepwise selection process during the analysis, and the final study population reflects the total number of eligible patients. The participants were followed up until March 2024.
Data Collection
The following data were collected for each patient: age (categorized as <65, 65-74, 75-84, 85-94, ≥95 years), sex, long-term care need levels (categorized as care support levels 1 to 2, care need levels 1 to 3, care need levels 4 and 5, and Unknown/No application), relationship of the main caregiver with the patient (categorized as spouse, child, child-in-law, other, equally shared care by 2 or more caregivers, no caregiver, or unknown), and household composition (categorized as living alone, couple-only household, 2-generation household, 3-generation household, other, or unknown). For all categorical variables, missing values were deemed “unknown” and included in the analysis. The main medical diagnoses were also collected and categorized as cancer, dementia, stroke, respiratory disease, fractures, neurological diseases, arthritis, spinal cord injury, senility, or other. All demographic information was obtained at the time of the initial home visit.
Additionally, we extracted the duration of physician-led home visit care and the clinical outcome. The duration of home visits was calculated from the start and end dates of home visits and categorized as <1 month, 2 to 3 months, 4 to 6 months, 7 to 12 months, or >1 year. Clinical outcomes were classified as “died at home,” “hospitalization,” “continue,” or “other/unknown.” The “other/unknown” category included cases such as transitioning back to outpatient care, transfer to another clinic or hospital, admission to a facility, or death outside the home. All clinical outcomes, including home death, were confirmed based on documentation in the medical records. For patients who were hospitalized and later resumed home visits, the outcome and duration were determined based on the last home visit.
Statistical Analysis
First, we analyzed the trends in the total number of patients who newly initiated physician-led home visit care, as well as the trends among cancer and non-cancer groups, for each quarter (January-March, April-June, July-September, and October-December) from April 2019 to March 2023. Second, we examined the total duration of home visits and the outcomes at 3 months for patients who started home visits in each quarter.
Next, we divided the observation period into 2 distinct intervals: the pre-pandemic period (April 2019 to March 2020) and the during-pandemic period (April 2020 to December 2022). April 2020 was designated as the start of the pandemic period, as the initial state of emergency was declared on 7 April, which led to significant changes in the healthcare system and daily life. 22 We compared patient characteristics, duration of home visits, and outcomes at 1, 3, and 6 months between the pre-pandemic and during-pandemic periods, using Mann-Whitney U tests for continuous variables and Chi-square or Fisher’s exact test for categorical variables. Furthermore, patients were stratified into cancer and non-cancer groups to account for differences in background characteristics and outcomes. Additionally, to further clarify caregiver dynamics, we examined patients’ age and caregiver relationship patterns by patient sex, cancer status, and pandemic period.
Finally, we conducted logistic regression analyses to assess the association between the pandemic period and home death within 1, 3, or 6 months. Model 1 was unadjusted; Model 2 was adjusted for age, sex, care need level, caregiver relationship, household composition, and cancer; and Model 3 added an interaction term between cancer and the pandemic period to Model 2.
To further examine whether the impact of the pandemic varied by underlying conditions, we conducted additional logistic regression analyses to assess interactions between the pandemic period and each major chronic disease category (dementia, stroke, respiratory disease, cardiac disease, neurological disease, senility, and others). Similar to Model 3 in the main analysis, we constructed separate models for each condition, including an interaction term between the condition and the pandemic indicator, while adjusting for the same covariates used in Model 2. The outcomes were defined as home death within 1, 3, or 6 months after the initiation of home visit care, consistent with the main analysis.
All statistical analyses were conducted using a 2-sided approach, with the significance level set at P < .05. We used Stata statistical software (version 17.0; StataCorp, Texas, USA) for the analysis.
Ethical Approval
This study was approved by the Ethics Committee of the University of Tsukuba (approval no. 1958) in accordance with the Declaration of Helsinki. Given that medical records were used retrospectively, the requirement for informed consent was waived by the ethics committee.
Results
We identified 1922 individuals who newly started physician-led home visit care between April 2019 and March 2023. Figure 1 illustrates trends in the total patient population and separately for patients with and without cancer. The total patient population showed an upward trend beginning in the second quarter of 2020, coinciding with the onset of the COVID-19 pandemic in Japan. The cancer group exhibited a slightly greater increase following the pandemic than the non-cancer group. Appendix 1 presents the trends in each medical institution.

Trends in newly started physician-led home visits: total, cancer, and non-cancer patients.
Figure 2 depicts the duration of continued care, and Figure 3 presents the outcomes at 3 months after the initiation of home visit care. Since the first quarter of 2020, there has been a noticeable increase in the proportion of patients completing home visit care within a short duration, particularly within 1 month, and an increase in those receiving end-of-life care at home.
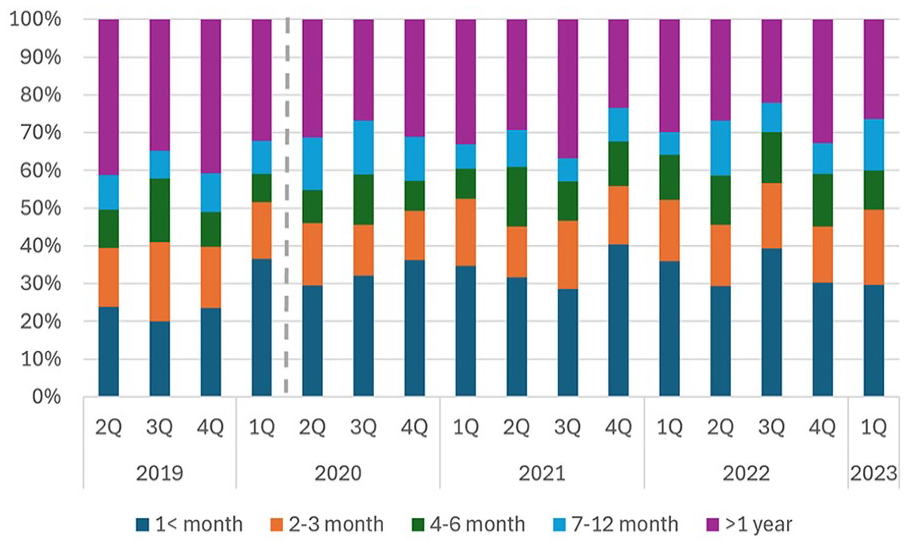
Trends in the duration of home visit care for patients who started physician-led home visits in each quarter.

Trends in outcomes at 3 months for patients who started physician-led home visits in each quarter.
Table 1 summarizes the characteristics and outcomes of the patients, comparing the pre- and during-pandemic periods. No significant differences were observed in age groups, sex, care need levels, caregiver relationships, or household composition between the 2 periods. In both periods, the most common demographics included patients aged 85 to 94 years, those with care need levels 4 and 5, spouses as primary caregivers, and 2-generation households. The proportion of patients with cancer significantly increased during the pandemic (pre-pandemic: 37.5% vs. during-pandemic: 43.0%, P = .046), while the proportion of patients with dementia (15.2% vs. 11.3%, P = .033) and stroke (9.1% vs. 6.0%, P = .028) decreased. The duration of care also shifted during the pandemic, with a significant rise in cases lasting <1 month and a reduction in cases lasting over 1 year. Outcomes revealed a notable increase in home deaths at 1, 3, and 6 months after the initiation of home visit care during the pandemic, accompanied by a corresponding decrease in hospitalizations.
Characteristics and Outcomes of Newly Started Physician-led Home Visits Before and During the COVID-19 Pandemic.

Abbreviation: SD, standard deviation.
Before pandemic period: from April 2019 to March 2020; During pandemic period: from April 2020 to March 2023.
To compare the pre-pandemic and during-pandemic periods, Mann-Whitney U tests were used for continuous variables, and Chi-square tests were used for categorical variables.
Appendix 2 shows the results stratified by cancer status. Patients with cancer were generally younger, had a higher proportion without long-term care certification, were more likely to have a spouse as their primary caregiver, and were more likely to live in couple-only households. These characteristics remained consistent across the pre- and during-pandemic periods. Across the entire study period, 53.3% of patients with cancer completed care within 1 month, compared to 16.1% of patients without cancer. Home deaths increased in both groups during the pandemic, with a greater rise observed among cancer patients.
Appendix 3 presents patients’ age and caregiver relationship patterns by patient sex, cancer status, and pandemic period. Among patients without cancer, females were consistently older than males across both periods. In contrast, among patients with cancer, age differences were minimal before the pandemic, but females became slightly younger than males during the pandemic. Spouse caregivers were more common for male patients, while child caregivers were more frequent for female patients, regardless of cancer status or pandemic period.
Table 2 presents the logistic regression results, with full variable details in Appendices 4 to 6. In both the unadjusted (Model 1) and adjusted (Model 2) models, home deaths within 1 month significantly increased during the pandemic (odds ratio (OR) [95% confidence interval (CI)] for Model 1: 1.91 [1.40-2.60]; Model 2: 1.87 [1.33-2.63]). However, in Model 3, which included the interaction term between pandemic indicator and cancer, the main effect of the pandemic indicator disappeared, while the interaction between cancer and the pandemic became significant (OR [95% CI]: 9.33 [5.29-16.47]), exceeding the main effect of cancer alone (OR [95% CI]: 4.42 [2.27-8.60]). Similar trends were observed for home death within 3 and 6 months.
Results of the Logistic Regression Analysis Examining the Impact of the COVID-19 Pandemic and Cancer on Home Death Within 1, 3, and 6 Months After Initiating Physician-led Home Visit Care.

Data are presented as odds ratios (95% confidence intervals).
Model 1: unadjusted (crude). Model 2: adjusted for patient factors (age category, sex, long-term care need levels, relationship of the main caregiver with the patient, household composition, and cancer). Model 3: Included an interaction term between the pandemic period and cancer, in addition to Model 2 adjustments.
Pre-pandemic period: from April 2019 to March 2020; During-pandemic period: from April 2020 to March 2023.
The results of the additional analyses assessing interactions between the pandemic period and other chronic conditions are demonstrated in Appendix 7. The main effect of pandemic indicator alone remained significantly associated with increased home deaths within 1, 3, and 6 months even after including interaction terms in each chronic condition, and none of the interaction terms with these conditions showed a significantly positive association. Notably, the interaction terms for dementia, stroke, and neurological disease were significantly negative, indicating a lower likelihood of short-term home death during the pandemic among these patient groups (Appendix).
Discussion
This study investigated the characteristics of patients receiving physician-led home visit care during the COVID-19 pandemic in Japan, using data from medical records. Our findings revealed an increase in the number of patients utilizing home visit care, particularly among patients with cancer. Moreover, in the multivariable analysis, we found that the interaction between cancer and the pandemic indicator had the strongest association with home deaths occurring shortly after starting home visit care. This pattern was not observed for other chronic conditions, suggesting that cancer patients were disproportionately affected in their end-of-life care by the pandemic.
Although previous studies suggested a surge in the demand for home visits and end-of-life care at home during the pandemic,8 -12 quantitative evidence was lacking. Our study provides empirical evidence of the increased utilization of home visit care and home-based end-of-life in shorter care duration, particularly for patients with cancer, during the COVID-19 pandemic. One possible reason is that during the COVID-19 pandemic, many palliative care units were converted into COVID-19 wards, 7 potentially limiting inpatient options. Another significant factor may be the visitation restrictions in hospitals, 7 which encouraged a shift toward home-based care, even for patients with severe conditions and limited prognoses. This allowed patients to spend meaningful time with their families during their final days rather than facing isolation in hospitals. Notably, from the first quarter of 2020, even before the state of emergency, there was a marked increase in patients with shorter home visit durations and those who died at home within 3 months of starting home care. In Japan, various hospitals had already implemented visitation restrictions from February to March 2020, following the initial outbreak. Furthermore, patients who initiated home visit care in January 2020 reached their 3-month outcome in April 2020, coinciding with the declaration of the state of emergency, indicating that their care decisions were already influenced by the pandemic. In contrast to cancer, newly initiated home visits for patients with dementia and stroke decreased during the pandemic, and short-term home deaths also declined, supported by negative interactions between the pandemic indicator and these conditions. These findings may reflect a pandemic-driven shift toward prioritizing urgent end-of-life care for patients with cancer, while home visits for chronic conditions focused more on stable cases.
Our study found that both patients with and without cancer commonly lived in 2-generational households. However, their primary caregivers differed: patients with cancer were typically cared for by spouses, while patients without cancer were more often cared for by their children. This may be because patients with cancer tend to be younger, with spouses more capable of caregiving, and because having a spouse is associated with higher rates of home death among patients with cancer. 12 A stratified analysis showed that male patients were more often cared for by spouses, while female patients were more often cared for by children, regardless of cancer status or pandemic period. Among patients without cancer, this pattern may be attributed to the older age of female patients, which likely reduces the probability of having a living spouse and increases reliance on children for care. In contrast, among patients with cancer, female patients were slightly younger than males, suggesting that factors beyond age—such as gender norms and caregiving expectations—may also shape caregiving roles in the home. While this study did not identify changes in caregiver relationships during the pandemic, the shift toward home-based end-of-life care may have reflected caregiver availability and preferences. Further research is needed to better understand how caregiver dynamics influence care decisions.
Our findings may be partly explained by Japan’s physician-led home-visit care system. Because physicians play a central role in home-based care delivery, including initiating advance care planning and managing symptoms directly, this structure may have facilitated the observed shift toward home-based end-of-life care among patients with cancer. In addition, all medical institutions that participated in this study were enhanced HCSCs, which play an important role in home healthcare in Japan. 19 However, even within these clinics, the average number of full-time physicians is reported to be fewer than 3. 23 Consequently, the increased demand for home visits and end-of-life care at home for patients with cancer, coupled with the need to manage febrile patients during the pandemic, may have imposed a substantial burden on these clinics. Under such extraordinary circumstances, it is essential to allocate medical resources effectively and implement measures to reduce the burden on home healthcare physicians who respond to increased demand.
This study has some limitations. First, as data were obtained from 6 institutions in a single prefecture, generalizability may be limited. However, the observed trends in home deaths align with national patterns,9 -12 suggesting broader applicability. Second, patients who initiated home visit care earlier had inherently longer follow-up periods, which could have led to an extended duration of recorded care, particularly if care was resumed after hospitalization. Nonetheless, the consistent increase in home deaths shortly after care initiation remains robust. Finally, it is difficult to attribute all observed changes solely to the COVID-19 pandemic. The pre-pandemic period spanned only 1 year, and unmeasured factors such as institutional practices or physician availability may have influenced the results. However, prior studies with longer observation periods reported a marked increase in home deaths after the pandemic began,9 -12 supporting our interpretation. Moreover, the consistent rise in newly initiated physician-led home visits across all institutions reinforces the reliability of the observed trend.
Conclusion
Our study identified a significant increase in the initiation of home visit care among patients with cancer during the COVID-19 pandemic, along with a higher proportion of patients receiving end-of-life care within a short period. Medical institutions, such as HCSCs, likely adapted to meet the growing demand for home-based care. These findings highlight the importance of strengthening physician-led home care systems during extraordinary circumstances such as a pandemic, particularly for patients with cancer. To support this shift, targeted strategies—such as the timely allocation of cancer-related resources to home-visit physicians and enhanced support for family caregivers in the home setting—are essential in preparing for future public health emergencies.
Footnotes
Appendix
Results of Logistic Regression Models Assessing Interaction Effects Between the Pandemic Period and Each Chronic Condition on Home Death Within 1, 3, and 6 Months.

| Outcome: home death within 1 month after initiating physician-led home visit care | Outcome: home death within 3 months after initiating physician-led home visit care | Outcome: home death within 6 months after initiating physician-led home visit care | |
|---|---|---|---|
| Variable | OR (95% CI) | OR (95% CI) | OR (95% CI) |
| Dementia | |||
| During-pandemic period (vs. pre-pandemic period) a | 1.77 (1.27-2.47) | 1.59 (1.19-2.11) | 1.71 (1.30-2.24) |
| Dementia (vs. non-dementia) | 0.12 (0.02-0.92) | 0.27 (0.10-0.79) | 0.29 (0.11-0.75) |
| During-pandemic period a × dementia | 0.48 (0.24-0.98) | 0.34 (0.18-0.63) | 0.37 (0.21-0.64) |
| Stroke | |||
| During-pandemic period (vs. pre-pandemic period) a | 1.88 (1.35-2.62) | 1.58 (1.20-2.09) | 1.68 (1.29-2.20) |
| Stroke (vs. non-stroke) | 0.49 (0.11-2.16) | 0.23 (0.54-1.00) | 0.19 (0.05-0.83) |
| During-pandemic period a × stroke | 0.37 (0.14-0.97) | 0.32 (0.15-0.70) | 0.37 (0.19-0.74) |
| Respiratory disease | |||
| During-pandemic period (vs. pre-pandemic period) a | 1.82 (1.30-2.53) | 1.56 (1.18-2.07) | 1.65 (1.26-2.16) |
| Respiratory disease (vs. non-respiratory disease) | 0.44 (0.10-1.98) | 0.35 (0.10-1.24) | 0.29 (0.08-1.00) |
| During-pandemic period a × respiratory disease | 1.04 (0.53-2.04) | 0.85 (0.47-1.51) | 0.99 (0.58-1.69) |
| Cardiac disease | |||
| During-pandemic period (vs. pre-pandemic period) a | 1.95 (1.39-2.73) | 1.68 (1.27-2.23) | 1.79 (1.36-2.33) |
| Cardiac disease (vs. non-cardiac disease) | 1.33 (0.43-4.18) | 0.99 (0.35-2.79) | 0.75 (0.27-2.12) |
| During-pandemic period a × cardiac disease | 1.14 (0.61-2.15) | 0.80 (0.45-1.40) | 0.75 (0.44-1.28) |
| Neurological disease | |||
| During-pandemic period (vs. pre-pandemic period) a | 1.92 (1.39-2.67) | 1.67 (1.27-2.20) | 1.79 (1.37-2.33) |
| Neurological disease (vs. non-neurological disease) | 0.75 (0.09-6.48) | 0.36 (0.04-3.03) | 0.67 (0.14-3.35) |
| During-pandemic period a × neurological disease | 0.21 (0.05-0.93) | 0.10 (0.02-0.45) | 0.30 (0.12-0.74) |
| Senility | |||
| During-pandemic period (vs. pre-pandemic period) a | 1.95 (1.40-2.72) | 1.74 (1.31-2.30) | 1.82 (1.39-2.38) |
| Senility (vs non-senility) | 1.42 (0.39-5.16) | 1.78 (0.66-4.81) | 1.36 (0.51-3.65) |
| During-pandemic period a × senility | 1.09 (0.56-2.11) | 0.84 (0.47-1.50) | 0.98 (0.58-1.65) |
| Other | |||
| During-pandemic period (vs. pre-pandemic period) a | 1.87 (1.34-2.61) | 1.57 (1.18-2.07) | 1.69 (1.29-2.21) |
| Other (vs. non-other) | 0.56 (0.13-2.53) | 0.28 (0.06-1.22) | 0.31 (0.09-1.10) |
| During-pandemic period a × other | 0.90 (0.46-1.75) | 0.87 (0.50-1.52) | 0.81 (0.47-1.38) |
Abbreviations: CI, confidence interval; OR, odds ratio.
Pre-pandemic period: from April 2019 to March 2020; During-pandemic period: from April 2020 to March 2023.
Each model included an interaction term between the pandemic period and each chronic condition, adjusting for age category, sex, long-term care need levels, relationship of the main caregiver with the patient, and household composition.
Acknowledgements
ORCID iDs
Ethical Approval
This study was approved by the Ethics Committee of the University of Tsukuba (approval no. 1958) in accordance with the Declaration of Helsinki.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
YS, RG, JH, and TM contributed to the conceptualization and methodology of the study. SN, SM, NK, TI, SH, and NK contributed to developing the research framework for data collection at each medical institution. YS, SF, MI, and TK were involved in data collection. YS conducted the data analyses and drafted the original manuscript. All authors contributed to revising the manuscript and approved the final version. YS is the guarantor.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Yuumi Memorial Foundation for Home Health Care; however, no specific grant or award number was provided. The funder played no role in the conception, design, implementation, or reporting of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available upon reasonable request.