
Abstract
Introduction:
Despite strong evidence supporting the benefits of water fluoridation in preventing dental caries, limited research exists on U.S. adults’ knowledge, attitudes, and behaviors regarding fluoride and tap water intake. This study examined the knowledge, attitudes, and behaviors regarding fluoride and tap water intake of Green Hill, Alabama adults.
Methods:
A convenience sample of 291 adults was surveyed concerning their knowledge, attitudes, and behaviors about fluoride in water and toothpaste, and water consumption preferences.
Results:
There was a high level of knowledge about fluoride’s role in cavity prevention, with 92.4% correctly identifying its benefits. However, 18.3% were unaware that fluoride does not help maintain healthy gums. Regarding attitudes, 14.5% strongly agreed and 28.3% agreed that fluoride in drinking water was beneficial, while 29.1% strongly supported and 53.5% supported its inclusion in toothpaste. A preference for bottled water over tap water was noted by 84.4% of participants, with 36.9% citing distrust of tap water quality as a primary reason. Bivariate analysis found a positive perception of fluoride in tap water correlated with better knowledge, while education level and fluoride awareness influenced attitudes.
Conclusion:
Additional research is necessary to explore reasons underlying adults’ water consumption habits and fluoride perceptions.
Introduction
People have opportunities to receive fluoride from a variety of different sources, but years of research has shown that having optimal levels of fluoride in the water is the easiest, most equitable and most cost-effective way for people to prevent caries, and is actually cost-saving. 1 It has also been shown that water fluoridation is associated with lower dental caries rates. 2 Weyant et al 3 also recommended that both self-applied (eg, toothpaste and mouthrinse), and professionally-applied topical fluorides are critical for caries prevention. Despite 80 years of research demonstrating fluoride’s safety and important role in caries prevention, recent publications, including a National Toxicology Program Monograph 4 and article by Taylor et al, 5 a federal judge’s decision in a lawsuit against the Environmental Protection Agency (EPA), 6 and statements by the Department of Health and Human Services Secretary Robert Kennedy, Jr.7,8 have raised concerns about possible associations of fluoride exposure and cognition and neurodevelopment. However, Levy 9 emphasized the many methodological problems with the publications on which the judge’s decision mostly was based.
Among the studies conducted on knowledge, attitudes, and behaviors toward fluoride or water intake, very few were focused on adults and most of these2,10 -14 were conducted outside the United States. Therefore, it cannot be assumed that the same results would have been found if the studies had been conducted in the US. Of the studies on knowledge, attitudes, and behaviors toward fluoride, many were targeted toward adults with young children.15 -17 This is appropriate since prevention in childhood means that the parents are critical since they are the main ones determining oral health and other preventive and risk behaviors. 18 While these studies are necessary and provide evidence that oral health professionals need to continue educating parents on the benefits of fluoride to assist in preventing childhood caries, adults without children are often overlooked when it comes to education on the benefits of fluoride for themselves. Although most of these individuals probably have been educated at some point in their lives about the importance of fluoride, many of them probably did not understand the content or had forgotten that information.
Roberts-Thompson et al 12 reported that older adults in Australia were more likely than younger adults to hold erroneous views on methods for cavity prevention, such as fluoride use. But the gaps in knowledge do not stop there. Curiel et al 19 identified a positive correlation between higher health literacy scores of American adults and acceptance of water fluoridation. Regarding water intake, Rosinger 13 reported that there was an increase, between 2005 and 2018, in plain water intake (bottled plus tap water combined) in the United States, but it was due to the increased intake of bottled water and not tap water. Additionally, they stated that 51% of adults reported drinking no tap water on a given day in 2017 to 2018. 13 Data from a Turkish survey conducted by Birant et al 14 showed that 89% of people with only a high school education and 64% of people with a college education did not even know about the different types of self-applied or office-based applications of topical fluoride available. Furthermore, Horowitz et al 20 reported that very few US adults even understood the importance of fluoride. The results from these studies, coupled with the increased nationwide fear of fluoride, make it more important than ever that additional research be conducted to better understand the many gaps in knowledge, attitudes, and behaviors toward fluoride that exist among adults, to provide guidance concerning how they can be addressed, in addition to identifying the reasoning behind adults’ water intake preferences. Overall, these deficiencies leave a major gap in our understanding of these factors, which leads to the purpose of this study, to investigate the knowledge, attitudes, and behaviors concerning fluoride and tap water intake of adults living in Green Hill, Alabama.
Methods
This study received ethical approval from the University of Iowa IRB (approval # 202204349) on June 7, 2022 and May 31, 2023. This is an IRB-approved study, all patient information was de-identified. For informed consent, a cover letter was attached to the survey which explained that by completing the survey, the subjects were providing consent for their responses to be used in this study. The cover letter also stated that all results of the survey would be kept anonymous.
A convenience sample of adults who lived in the Green Hill, Alabama community was surveyed for this study. Inclusion criteria were subjects had to be 18 years of age or older and live in a household within the Green Hill Water Department supply district. Subjects were recruited through advertisements on social media and flyers displayed in local businesses with a QR code to scan. Surveys were completed online through Qualtrics. As part of the instructions to the survey, subjects were informed that an incomplete survey would be viewed as their decision to have their responses removed from the study. Originally, 377 adults agreed to participate in the study, but after elimination of incomplete responses, 291 subjects were included in the analyses.
The survey consisted of 30 questions, covering demographics, knowledge, attitudes, and behaviors concerning fluoride, and tap water intake. Subjects selected which region of the community they lived in from a map (Figure 1), which allowed them to be grouped based on the level of fluoride in the tap water in their household (0.7, 0.35, or 0.1 mg/L).

Study community regions with different levels of fluoride in household tap water (0.7 mg/L (red, 9%), 0.35 mg/L (gray, 67%), and 0.1 mg/L (blue, 24%)).
In addition to considering individual questions, 2 composite variables were created across a few questions each. The first dependent variable was concerning subjects’ knowledge about fluoride. Participants answered 5 questions, and for each question, they were asked to select either yes or no. The responses to each question were analyzed individually and as a composite score, which had a possible range of 0 to 5 correct answers. The next dependent variables were about participants’ attitudes toward fluoride. Subjects answered 3 questions. However, this time, they responded by choosing how much they agreed or disagreed with each of the questions based on a 5-point scale, from 0 meaning strongly disagree to 4 meaning strongly agree. The responses to each question were analyzed individually and as a composite score, which allowed for a possible range of 0 to 12.
Descriptive statistics were generated. Bivariate analyses assessed associations of several possible explanatory variables (perceptions of fluoride in tap water, preference for tap water over bottled water, consideration of presence of fluoride when purchasing toothpaste, region within the community, highest education level, age, and gender) separately with the composite variables for knowledge concerning fluoride and the composite variable for attitudes toward fluoride. P-values less than .05 were considered statistically significant. SPSS version 29 was used for all analysis.
Results
The main results for individual variables and our knowledge and attitude composites are summarized first, followed by presentation of the main bivariate results. The mean age of respondents was 44.2 ± 15.6 years and 77.6% were female. For the highest level of education, 16.7% reported a high school diploma or less, 47.9% reported some college or a 2-year college degree, and 35.4% reported a 4-year college degree or more. The large majority (84.4%) preferred bottled water over tap water, 61.2% reported that the presence of fluoride had no effect on their tap water consumption, 76.2% reported using tap water in making other beverages (tea, coffee, Kool-Aid®, lemonade, etc.), 70.5% reported brushing their teeth at least twice a day, 82.3% reported going to the dentist for a checkup and/or cleaning at least once during the previous year, and 67.0% reported having no fillings or teeth extracted due to cavities during the previous 24 months. Among those who chose not to drink (or drink very little) tap water at home, 36.6% reported the reason was due to their lack of trust of the source of the water and 57.3% because the water tasted funny/smelled bad. For the highest level of education, 16.7% reported a high school diploma or less, 47.9% reported some college or a 2-year college degree, and 35.4% reported a 4-year college degree or more As seen in Figure 1, 9% reported living in the red region of the community with 0.7 mg/L fluoride in their household tap water, 67% in the gray region with 0.35 mg/L fluoride, and 24% in the blue region with 0.1 mg/L fluoride.
Descriptive results for individual questions regarding subjects’ knowledge and attitudes concerning fluoride are shown in Tables 1 and 2, respectively. Subjects generally were knowledgeable about the basics of fluoride, with 71%-92% reporting the correct answers for 4 of the 5 questions (Table 1). However, only 18.3% answered correctly that fluoride does not help maintain healthy gums.
Descriptive Results Concerning Individual Knowledge Questions about Fluoride.

Correct answers are shown in bold.
Distribution of Results Concerning Individual Attitude Questions about Fluoride.
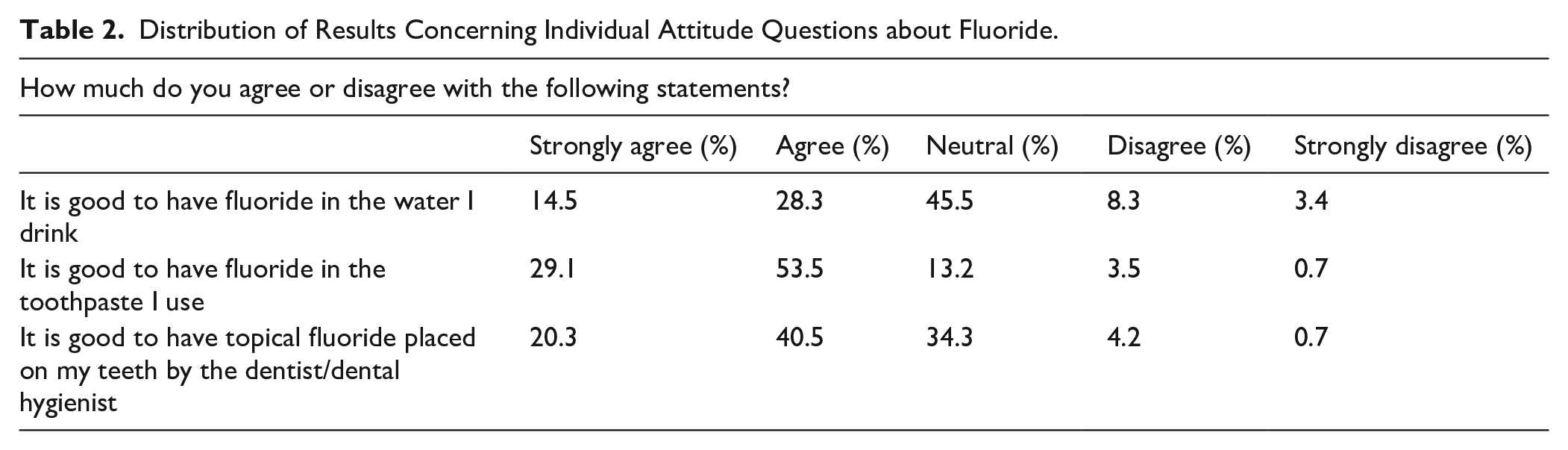
Table 2 shows the results regarding subjects’ attitudes toward fluoride. Concerning the statement that it was good to have fluoride in the water they drink, approximately 12% of subjects disagreed or strongly disagreed, 46% were neutral, and 43% agreed or strongly agreed. The large majority of subjects (83%) agreed or strongly agreed that it was good to have fluoride in their toothpaste and approximately 61% agreed or strongly agreed that it was good to have fluoride placed on their teeth by a dentist or dental hygienist.
Bivariate analyses showed that a more positive perception of fluoride in tap water was positively associated with a higher composite knowledge score (P = .016). Preference for tap water over bottled water was associated marginally with a higher attitude composite score (P = .076). Considering the presence of fluoride important when purchasing toothpaste was associated with a higher attitude composite score (P < .001). Higher education level was positively associated with a higher attitude composite score (P = .009). Considering the presence of fluoride in tap water important was positively associated with a higher attitude composite score (P < .001). Region within the community, highest education level, age, and gender were not significantly associated with composite knowledge score (all P > .10). Additionally, region within the community, age, and gender were not significantly associated with composite attitudes score (all P > .10)
Discussion
Overall, at least 70% of responses to each of 4 of the 5 statements about knowledge of fluoride from Table 1 were correct. The only statement that did not reach this threshold was the one that stated fluoride helps maintain healthy gums. Only 18.3% of subjects answered this statement correctly. Regarding attitudes toward fluoride from Table 2, no more than 8.3% of subjects disagreed and no more than 3.4% of subjects strongly disagreed with any of the statements about fluoride. It is worth noting that there was no overlap between the variables that were significantly associated positively with the composite knowledge score and those that were significantly positively associated with the composite attitudes score. The composite knowledge score was significantly associated positively with positive perception of fluoride in tap water, while the composite attitudes score was positively associated with preference for tap water over bottled water, considering preference of fluoride important when purchasing toothpaste, and considering presence of fluoride in tap water important. From a descriptive standpoint, a large majority of subjects preferred bottled water over tap water and one-third of subjects reported not trusting the source of the tap water as being a reason as to why they choose not to drink tap water (or drink very little).
The study had several limitations. These include the use of a convenience sample in a small geographic region, small sample size, limited marketing of the survey, the inability to validate the results, and the survey being conducted mostly online.
The study also had several strengths. Having the survey anonymous probably led to less desirability bias. Additionally, the removal of participants with incomplete responses and the extended timeframe to survey subjects were additional strengths to the study.
Comparing our results to those from other studies was difficult due to the paucity of similar studies, but our results were not consistent with the few existing studies that showed substantial gaps exist in adults’ knowledge and attitudes when it comes to fluoride. Although gaps were identified in this study, they do not appear to be as evident or as substantial as similar studies. The results from this study showed more similarities with previous studies on tap water versus bottled water consumption. For example, Horowitz et al 20 reported that very few adults in the United States understood the importance of fluoride. However, Table 1 demonstrates that most adults from this study understood the importance of fluoride, except for the statement that fluoride helps maintain healthy gums. Table 2 indicates that a majority of all surveyed adults have basic knowledge of fluoride and its role in cavity prevention, which differs from what Roberts-Thompson et al 12 reported from their study of Australian adults. Lastly, Rosinger 13 reported that 51% of adults did not drink tap water on a given day, which is generally consistent with this study’s results of 55% of adults not drinking tap water on a given day. Additional research is needed to expand and diversify our sample and delve deeper into why some adults don’t drink tap water at home. Identifying the reason behind this is even more important today with greater general distrust of the American people with government and health authorities21,22 and the recent publications4,5,23 and the EPA lawsuit 6 concerning fluoride and lower IQ. Lastly, if we want to continue improving oral health through preventive measures, we as healthcare professionals must become more proactive regarding the benefits of fluoride.
Footnotes
Acknowledgements
None.
Ethical Approval
This study received ethical approval from the University of Iowa IRB (approval #202204349) on June 7, 2022, and May 31, 2023.
Informed Consent Statement
This is an IRB-approved study, all patient information was de-identified and patient consent was not required. Patient data will not be shared with third parties.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Iowa College of Dentistry Student Research Program.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data can be shared upon request and explanation of rationale for the request from qualified individuals.
Any Other Identifying Information Related to the Authors and/or Their Institutions,Funders,Approval Committees,etc. That Might Compromise Anonymity
None.