
Abstract
Introduction:
This study examines the association between the age of hypertension onset and the risks of cardiovascular diseases (CVD) and mortality.
Methods:
Two retrospective cohort studies were conducted using electronic medical records from public healthcare systems in the UK and Hong Kong (HK). Adults (≥18 years) who attended public health services between January 1, 2008 and December 31, 2013 were included in the study. Patients diagnosed with CVD before baseline or who transferred out of practice before baseline in the UK cohort were excluded. Hypertension onset was defined as a diagnosis of hypertension (≥140/90 mmHg) or the prescription of anti-hypertensive medication. Patients were categorized based on hypertension onset and divided into 6 age groups based on onset age. Propensity score fine stratification weights were applied to ensure balance between groups. Multivariable Cox proportional hazards regression a was used to assess risks of CVD, cardiovascular mortality, and deaths.
Results:
The UK cohort included 481 791 new-onset hypertension patients and 3 893 134 controls, while the HK cohort included 552 594 new-onset hypertension patients and 2 548 914 controls. Hypertension was associated with increased CVD and mortality risks, which decreased with older onset ages. In the UK cohort, hypertension onset at ≤39 years had the highest risks for CVD and deaths, with adjusted hazard ratios (HR = 4.30, 95% CI [3.98, 4.65] and HR = 2.86, 95% CI [2.64, 3.10]). For patients with hypertension onset at ≥80 years, risks were lower, with adjusted HR = 2.56, 95% CI [2.45, 2.68] for CVD and HR = 1.11, 95% CI [1.09, 1.14] for deaths. Similar trends were observed in the HK cohort.
Conclusion:
Younger age of hypertension onset is associated with higher risks for cardiovascular events and mortality, highlighting the need for early screening and intensive interventions in younger adults to improve long-term blood pressure control and reduce cardiovascular complications and deaths, alleviating the chronic disease burden on the public healthcare system over the long term.
Introduction
Hypertension is a major risk factor for cardiovascular diseases (CVD) including stroke, heart failure, and mortality. While the majority of patients with hypertension are diagnosed at 40 years or later, 1 the prevalence of hypertension or pre-hypertension among children and young adults has progressively increased globally from 2000 to 2015.2 -4 It is estimated that between 4% and 30% of young adults (<40 years) worldwide has hypertension.5 -8 Essential hypertension is the predominant form of hypertension among young individuals. However, secondary hypertension, which has a specific underlying pathological cause, accounts for 5% to 30% of cases in this age group. 9 The complications of hypertension such as heart disease, stroke, kidney failure, and retinal damage, are particularly concerning, as they not only diminish quality of life but also contribute to long-term health issues and increased healthcare costs, emphasizing the importance of early detection and management. Meanwhile, the incidences of CVD among the population aged 18 to 50 years have also shown a steady increase over the last 2 decades, 10 although the awareness and treatment level for hypertension remained low among young adults. 11
Studies investigating the prognosis of hypertension with age have shown an attenuated risk for cardiovascular outcomes related to high systolic blood pressure (BP) with increasing age (≥ 70 years) among patients with hypertension. 12 However, these results may not be fully extrapolated to hypertension that begins at a younger age as older individuals often have other co-existing comorbidities. Age with prevalent hypertension may also not also be truly indicative of the age of hypertension onset. The association between early-onset hypertension, defined as <55 years based on international guidelines (NICE) 13 and the risk of cardiovascular events was first reported in the Johns Hopkins Precursor Study in 1987, where the risk of cardiovascular complications declined with an increasing age of hypertension onset from 40 to 49 to 60 to 69 years, irrespective of the initial severity and hypertension control. 14 Recent evidence had similarly reported a graded relationship between the age of hypertension onset and decreasing risks of target-end organ damage,15,16 cardiovascular events, and mortality 17 among individuals with hypertension. Among 2680 middle-aged individuals in the CARDIA study, those with a hypertension onset age <35 years had significantly greater odds (odd ratios ranging from 1.12 to 2.94) of target-end organ damage compared to normotensive individuals, while those with hypertension onset age ≥45 years did not observe increased odds by midlife. 15 These observations were subsequently confirmed in a follow-up study where a self-reported hypertension onset age at <35 years were associated with greater odds for hypertension-medicated organ damage, relative to individuals with a self-reported onset age of >45 years. 16 Finally, in a prospective study including 71 245 participants in the Kailuan study, early-onset hypertension (<45 years) was related to nearly doubled the risk of cardiovascular diseases and mortality, with hazard ratios suggesting a 2 to 3 fold increase for those diagnosed before age 45 years compared to those with onset age ≥65 years. 17 However, most prior studies are in part limited by a relatively small cohort in a single population, as well as a lack of thorough matching of patient characteristics apart from age and sex, limiting the statistical power to detect the association between age of hypertension onset and the risks of adverse events18,19 compared to individuals with normal blood pressure, especially among subcategories of cardiovascular endpoints and in the younger age ranges (<45 years). Given that cardiovascular disease (CVD) and mortality are significant long-term risks, especially in younger populations, it is crucial to understand the implications of hypertension onset at an early age. This research aimed to investigate the associations between the age of hypertension onset and subsequent cardiovascular events and mortality using electronic medical records from the United Kingdom and Hong Kong.
Methods
Study Design
This was a retrospective cohort study based on electronic medical records in United Kingdom and Hong Kong, China. In the UK cohort, medical records were extracted from IQVIA Medical Research Data, which is also known as the Health Improvement Network (THIN) and covers 6% of the UK population. The database has been applied in various previous studies20,21 and proved to be representative of the UK general population. 22 In the HK cohort, data was extracted from the Hong Kong Hospital Authority (HA), which is the regulatory body of all public hospitals in Hong Kong, including 43 hospitals and institutions, 49 Specialist Out-patient Clinics (SOPCs), and 73 General Out-patient Clinics (GOPCs). The validity and coding accuracy of the records have been evaluated and applied in previous studies.23 -25 In the UK, 87% of the population is Caucasian, 26 while in the HK, 90% of the population is Chinese. 27 Similar inclusion and exclusion criteria were used for both cohorts. Individuals who attended public health services between January 1st 2008 and December 31st 2013 were included in the study. Hypertension onset was defined as any diagnosis of hypertension or prescription of anti-hypertensive drug. In both UK (NICE) guidelines and Hong Kong guidelines,28,29 a cut-off of 140/90 mmHg measured in the clinic is recommended for the diagnosis of hypertension. In UK cohort, hypertension diagnose records were extracted based on Read Codes, summarized in Supplemental Table 1. In the HK cohort, International Classification of Primary Care, second edition (ICPC-2) codes of K86 and K87, and the International Classification of Diseases, Ninth Edition, Clinical Modification (ICD-9-CM) of 401*, 402*, 403*, 404*, or 405* were used to define hypertension. In both cohorts, the first date of hypertension diagnosis or prescription of anti-hypertensive drug was set as the baseline for each patient. Patients were first divided into 2 groups based on if they have new onset of hypertension or not (controls) between January 2008 and December 2013. Patients in the control group included those with any health service attendance between 2008 and 2013 but have not been diagnosed with hypertension nor have been prescribed any anti-hypertensive drugs. The first date of any consultation was set as the baseline for the patients in the control group. Patients were excluded from this study if they are: (i) diagnosed with CVD on or before baseline, (ii) aged less than 18 years at baseline. Additionally, for the UK cohort, patients who transferred out of the practice before baseline, and with less than 1 year of acceptable quality data were also excluded. Each patient was followed until the date of an outcome event, death, transferred out of the practice (for the UK cohort only), or the end of data availability (UK cohort: December 31st 2019; HK cohort: December 31st 2018), whichever was earlier.
This study was approved by the Hong Kong Hospital Authority and IQVIA Medical Research Data (IMRD) to use data for this study. All extracted data were anonymous, and no direct patient contact was required, thereby posing minimal ethical concerns. Informed consent from individual participants was not required because the data used in this study were anonymized. The IMRD incorporated data from THIN, a Cegedim Database. The IMRD contains routinely collected patient data from participating general practitioner practices in the UK. Informed consent from all patients to have their included included in the IMRD is obtained and patients have the option to opt out of the data collection at any time. References to THIN were intended to describe the data asset licensed by IQVIA. This study has been conducted and reported in accordance with the STROBE guidelines to enhance the clarity and reproducibility of the findings.
Outcome Measures
The main outcome event of this study was the first CVD incident after baseline, which included coronary heart disease (ICPC-2 K74, K76, K82; ICD-9-CM 411.x-414.x), stroke (ICPC-2 K89-91; ICD-9-CM 430.x-438.x), and heart failure (ICPC-2 K77; ICD-9-CM 402.01, 402.11, 402.91, 428.x) in the HK cohort. In THIN, the Read Codes for CVD definition was based on previous studies (31-33). Secondary outcomes included the individual subtypes of CVD, CVD mortality, deaths. Information on mortality was collected from the Hong Kong Death Registry. The Read Codes for diseases definition are summarized in Supplemental Table 1.
Baseline Characteristics
Baseline characteristics included age, sex, smoking status, drug use (anti-diabetic drugs and lipid-lowering agents), comorbidities (diabetes mellitus, atrial fibrillation, peripheral vascular disease, amputation, dementia, chronic lung disease, connective tissue disease, peptic ulcer disease, liver disease, chronic kidney disease, hemiplegia, leukaemia, malignant lymphoma, and cancer).
Statistical Analysis
Patients were categorized into 6 groups based on their age of hypertension onset (18-39, 40-49, 50-59, 60-69, 70-79, and ≥80 years old). Since the onset of hypertension is relatively infrequent in the younger age groups, a multivariable models adjusting for a number of confounders may result in overfitting and biased estimates. 30 Therefore, fine stratification weights were used to adjust for confounding through conditioning on the propensity scores. Specifically, a multivariable logistic regression adjusted for age, sex, smoking status, comorbidities, use of lipid-lowering agents and anti-diabetic drugs, was used to estimate the propensity score (predicted probability of being in the group of onset hypertension). Patients were stratified based on the fifty quantile categories of propensity score and weighting was conducted within each stratum. The standardized mean difference (SMD) was used to measure the balance of baseline covariates between the onset hypertension group and control group, with a SMD of less than 0.2 indicating sufficient balance. 31
Descriptive characteristics were presented as mean and standard deviation for continuous variables, and frequency and proportion for categorical variables. The incidence rate for each outcome was calculated for each group and the corresponding confidence interval (CI) was estimated based on the Poisson distribution. The association between the age of hypertension onset and the risk of each outcome after adjustment of patients’ baseline characteristics was examined by a multivariable Cox proportional hazard regression. The associations were also examined in subgroup analysis stratified by gender.
Multiple sensitivity analyses were carried out to strengthen the reliability of the results. First, patients with less than 1-year follow-up were excluded. Second, in the control group, patients who had a diagnosis of hypertension within 1 year after baseline were excluded. Third, patients in the control group who had diagnosis of hypertension after baseline were excluded. Forth, one-to-one matching based on propensity score were used. Fifth, patients diagnosed with hypertension after baseline in the control group were censored. Lastly, competing risk model adjusting mortality as the competing risk were used. 32 All data processing and analyses were performed using Stata 15.1. All significant tests were 2-tailed with significant level of P < .05.
Results
For the UK cohort, a total of 4 374 925 patients were included, of which 481 791 had new-onset hypertension and 3 893 134 were in the control group. For the HK cohort, a total of 3 101 508 patients were included, of which 552 594 had new-onset hypertension and 2 548 914 were in the control group. Baseline characteristics of patients with and without hypertension after weighting by age groups are shown in Table 1. The SMD for all covariates in all age groups were less than 0.2 after weighting, indicating good covariate balance. Descriptive statistics of the baseline characteristics and other clinical parameters before weighting can be found in Supplemental Tables 2 and 3.
Baseline Characteristics of Patients With and Without Hypertension in Different Age Groups After Weighting.

Abbreviations: HT, hypertension; SMD, standardized mean difference.
All parameters are expressed in either number (percentage) or mean (SD).
Results from the 2 cohorts are comparable. In the UK cohort, the median follow-up period was 11.4 years, during which a total of 70 200 CVD events, 8963 CVD mortality, and 106 647 deaths were recorded. In the HK cohort, the median follow-up period was 9.1 years, with 129 092 CVD events, 12 927 CVD mortality, and 161 580 deaths documented.
The incidence rates and the corresponding confidence intervals for CVD, CVD subtypes, CVD mortality, and deaths in each group are shown in Table 2. The incidence rate of CVD and deaths were higher among patients with new-onset hypertension compared to the control group across all ages of hypertension onset, with incidences increasing progressively with each decade increase in the age of hypertension onset in both cohorts. For example, in the UK cohort, the incidence rate of CVD among patients diagnosed with hypertension at ages 18 to 39 years was 0.96 (95% CI [0.90, 1.02]), compared to 0.18 (95% CI [0.17, 0.19]) in the control group. Among patients aged 60 to 69 years, the incidence rate of CVD was 11.65 (95% CI [11.40, 11.90]) for those with new-onset hypertension and 3.18 (95% CI [3.12, 3.25]) for those without.
Incidence Rate of Cardiovascular Diseases, Subtypes of Cardiovascular Diseases, Cardiovascular Mortality, and All-cause Mortality in Different Age Groups After Weighting.

Incidence rate (cases/1000 person-years) with 95% confidence interval based on Poisson distribution.
Hazard ratio with 95% confidence interval adjusted by age, gender, smoking status, diabetes mellitus, atrial fibrillation, peripheral vascular disease, amputation, dementia, lung disease, cumulative trauma disorder, peptic ulcer, liver disease, chronic kidney disease, hemiplegia, leukaemia, malignant lymphoma, cancer, the use of anti-diabetic drugs, lipid-lowering agents, and weighting.
The risks of all outcomes, represented using hazard ratios (HRs) adjusted for baseline characteristics are shown in Table 2 and Figure 1. Consistent with the observations in incidences rates, the risks of all outcomes were significantly higher in patients with new-onset hypertension compared to the control group. However, the increase in risk estimates for patients with new-onset hypertension decreased along the age spectrum for all outcomes. For instance, in the UK cohort, patients aged 18 to 39 years with new-onset hypertension exhibited greater risks of all adverse outcomes, with HR = 4.30, 95% CI [3.98, 4.65] for CVD and HR = 2.86, 95% CI [2.64, 3.10] for deaths. The HRs for CVD and deaths decreased gradually, ranging from 2.56 to 3.51 for CVD, and 1.11 to 1.74 for deaths among patients aged ≥50 years. Result from the HK cohort demonstrated a similar pattern. The HR (95% CI) of CVD in patients with new-onset hypertension was 5.04 (4.65, 5.47) at ages 18 to 39 years and decreased to 1.85 (1.79, 1.92) at age ≥ 80. Patients with new-onset hypertension at ages 18 to 39 years were at higher risk of mortality compared to those with new-onset hypertension at ages ≥80 (HR = 3.64, 95% CI [3.39, 3.91] vs HR = 1.27, 95% CI [1.25, 1.29]).
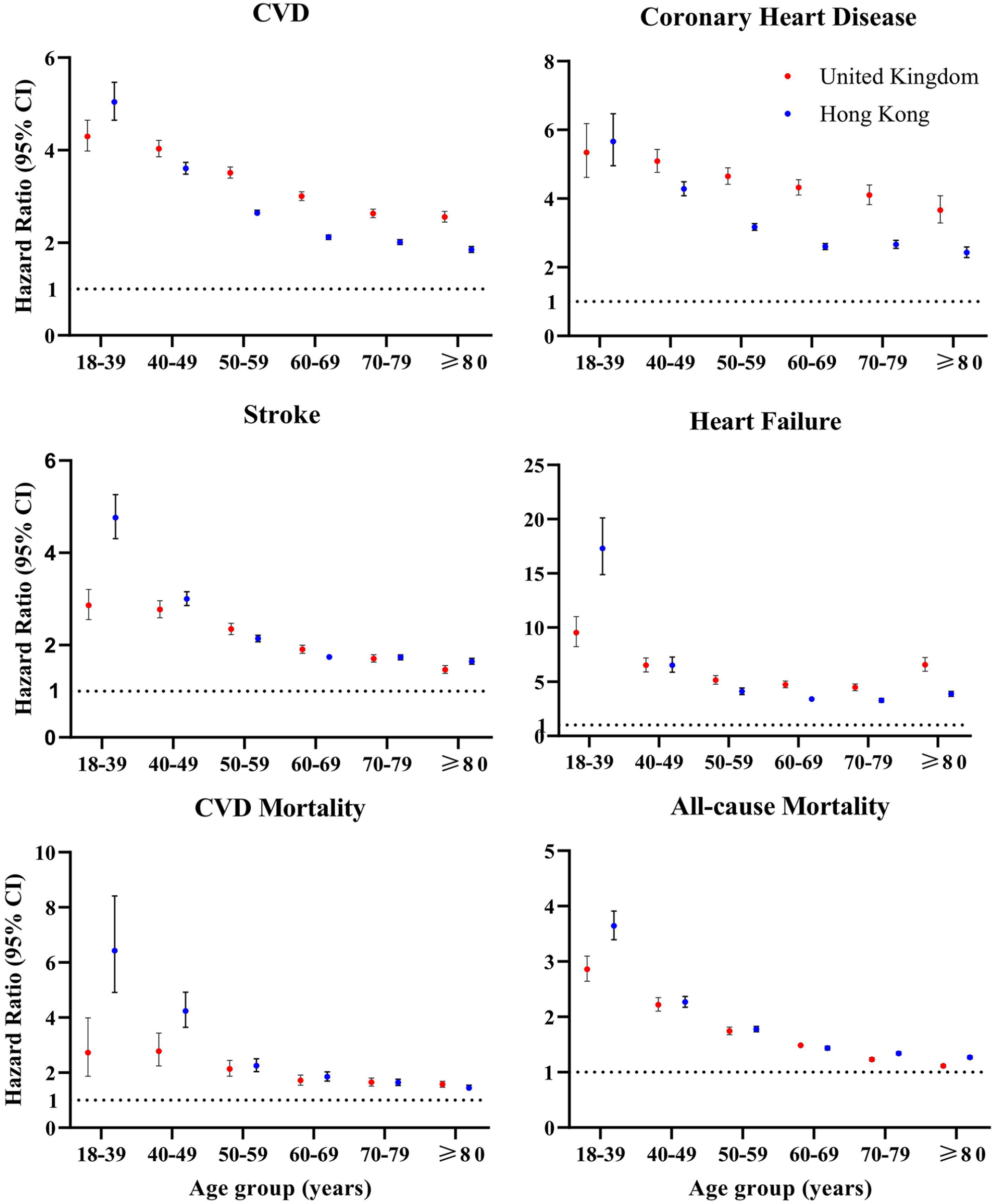
The associations between onset of hypertension and cardiovascular disease/mortality in different age groups using Cox regression. Hazard ratio with 95% confidence interval adjusted by age, gender, smoking status, diabetes mellitus, atrial fibrillation, peripheral vascular disease, amputation, dementia, lung disease, cumulative trauma disorder, peptic ulcer, liver, chronic kidney disease, hemiplegia, leukaemia, malignant lymphoma, cancer, the use of anti-diabetic drugs, lipid-lowering agents, and weighting. CVD was defined by coronary heart disease, heart failure, and stroke.
The association between the age of hypertension onset and adverse outcomes, stratified by sex is shown in Figures 2 and 3. Subgroup analyses revealed observations largely consistent with the main analysis. The risk of heart failure was significantly higher among female patients with hypertension compared to the control group among patients aged ≥50 years in the HK cohort. Similarly, in the UK cohort, female patients with hypertension exhibited an increased risk of CVD mortality, but only in the age groups 50 to 59 and 60 to 69 years.
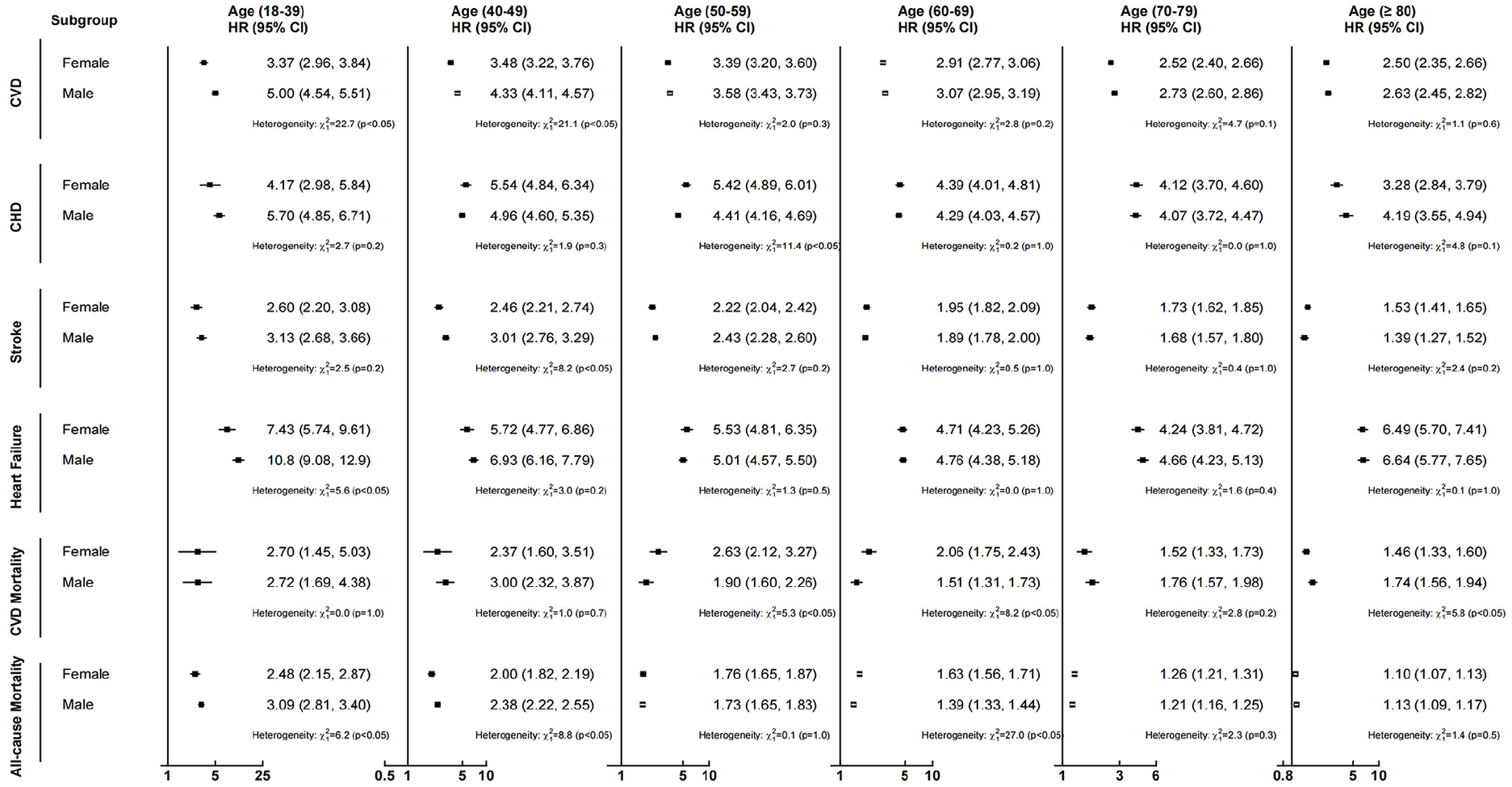
Associations between new onset HT and risk of CVD and mortality within subgroups stratified by gender in the United Kingdom. Hazard ratio with 95% confidence interval adjusted by age, gender, smoking status, diabetes mellitus, atrial fibrillation, peripheral vascular disease, amputation, dementia, lung disease, cumulative trauma disorder, peptic ulcer, liver, chronic kidney disease, hemiplegia, leukaemia, malignant lymphoma, cancer, the use of anti-diabetic drugs, lipid-lowering agents, and weighting. CVD includes coronary heart disease, heart failure, and stroke.

Associations between new onset HT and risk of CVD and mortality within subgroups stratified by gender in Hong Kong. Hazard ratio with 95% confidence interval adjusted by age, gender, smoking status, diabetes mellitus, atrial fibrillation, peripheral vascular disease, amputation, dementia, lung disease, cumulative trauma disorder, peptic ulcer, liver, chronic kidney disease, hemiplegia, leukaemia, malignant lymphoma, cancer, the use of anti-diabetic drugs, lipid-lowering agents, and weighting. CVD includes coronary heart disease, heart failure, and stroke.
Sensitivity analyses were conducted with patients having at least 1-year of follow-up (Supplemental Figure 1), excluding patients in the control group diagnosed with hypertension 1 year after baseline (Supplemental Figure 2), excluding patients diagnosed with hypertension after baseline in the control group (Supplemental Figure 3), one-to-one matching based on propensity score (Supplemental Figure 4), censoring patients diagnosed with hypertension after baseline in the control group (Supplemental Figure 5), and adjusting for mortality as a competing risk using the Fine and Gray Method (Supplemental Figure 6). All these analyses yielded results consistent with the primary analysis.
Discussion
Hypertension diagnosed at a younger age is associated with greater risks for cardiovascular diseases, and death, while the incremental risk associated with new-onset hypertension attenuated with the age of diagnosis. For instance, hypertension diagnosed before 40 years of age is associated with greater risks of CVD, CVD mortality, and overall deaths compared to individuals with normal blood pressure. Conversely, the CVD risk related to hypertension onset at ≥ 80 years is approximately 1 to 2-fold higher than in controls. These results emphasize the importance of identifying younger high-risk individuals and implementing early interventions to prevent premature morbidity and mortality.
Observations from this study are largely consistent with previous findings from the Framingham Heart Study, 19 the community-based CARDIA (Coronary Artery Risk Development in Young Adults) study, 33 the Korean National Health Insurance Service cohort study, 34 and the Kailuan cohort study. 17 Analyses from the CARDIA study 33 and a large population-based cohort in Korea 34 demonstrated that the risks of incident CVD events and deaths by middle age among adults with hypertension before 40 years was up to 1.2 to 3.5-fold greater, compared to those who maintained normal blood pressure. Recent studies17,19 comparing multiple age categories based on the age at hypertension onset consistently reported approximately 2.2 to 2.6-fold greater risks of cardiovascular events including stroke, coronary death, or deaths in patients with onset age <45 years relative to those without hypertension. The risk gradually attenuated with an increasing age of hypertension diagnosis, with some studies reporting little to no differences in risks for coronary deaths in patients with hypertension onset age of ≥65 years. 19 While certain methodological differences, including different stratification for age groups, racial differences of participants, and incomplete adjustments for potentially important cofounders, for example, blood lipids or glucose levels exist between the present and earlier studies, consistent trends in the observations reinforce that early hypertension onset results in poorer prognosis than late onset. It should also be noted that differences in the magnitude of risks between prior and the present study may also be depend on confounding factors, especially age and comorbidities associated with CVD and mortality in control patients. Nevertheless, this study extends existing evidence to include multiple cardiovascular endpoints in a large population-based cohort with matched characteristics between case and controls.
While chronological age is one of the strongest risk factors for hypertension, a distinction must be made between prevalent hypertension at an older age and hypertension that begins later in life. Results from this study therefore do not contradict previous large-scale studies that reported significantly higher risks of cardiovascular complications in older patients (>60 years) with existing hypertension,12,35 but rather characterize the impact of the age at which hypertension started. It is also important to distinguish whether results were reported as absolute or relative risks, 12 as younger hypertension patients would have a lower absolute risk but a higher relative risk for cardiovascular diseases and mortality, whereas the opposite is observed for older patients. This is consistent with the findings in this study, where lower relative risk of adverse clinical outcomes was observed with advancing age, but the absolute risks (ie, incidences) increases with age. These observations underscore the importance of a life course approach in managing hypertension given the higher relative risks in younger patients.
Several potential mechanisms have been proposed for the pathophysiology linking higher CVD and mortality risks and an early hypertension onset age. Patients with young-onset hypertension may have a higher prevalence of overlapping risk factors including obesity and high dietary sodium intake.19,36 -38 A recent analysis from the CARDIA study suggested that patients who were Black, with a higher BMI, and higher total cholesterol levels had 5.08, 1.57, and 1.34 greater odds of new-onset hypertension (<35 years) respectively, relative to not developing hypertension. 39 Conversely, higher HDL-cholesterol was related to lower odds of early-onset hypertension (OR = 0.71, 95% CI [0.57-0.89]). 39 The contribution of genetic background has also been suggested to be particularly important for young-onset hypertension,13,19 as parents with early-onset hypertension predicted incidences of hypertension and cardiovascular mortality in offspring, but not among those with late-onset hypertension. 19 Several genes central to the regulation of blood pressure pathways, including NPPA, AGT, LPL, and DCP1 have been implicated in influencing blood pressure or conferring susceptibility to young-onset hypertension.40,41 Exposure to high blood pressure from early life may result in premature cardiac and vascular changes. Thickening of arteries, increased arterial stiffness as well as reduced endothelial function have been reported in youths and adults with hypertension, contributing to elevated risks for coronary heart diseases and heart failure later in life.7,42 -44 Increased odds of left ventricular hypertrophy, coronary calcification, and diastolic dysfunction were also shown to be associated with early onset hypertension in the prospective CARDIA cohort study.15,45 Collectively, the impact of early-onset hypertension on CVD risk is likely related to a long-term exposure to high blood pressure in from adulthood and leading to cumulative physiological damages. 46
Existing clinical guidelines do not currently provide specific management guidelines for patients with early-onset hypertension.13,47,48 However, patients with early-onset hypertension are usually asymptomatic 49 and have a higher chance of having masked hypertension than the typical hypertension patient population. 47 As a result, the diagnosis and treatment of hypertension in the younger population are often delayed. 7 The importance of having comprehensive guidelines for early-onset hypertension, including both early detection and subsequent interventions, should not be neglected, as elevated blood pressure tracks strongly into later life and has been consistently shown to predict greater risks for morbidity and mortality. 50 Given the key role of genetic predisposition in early-onset hypertension, incorporation of polygenic risk scores as part of risk assessment models may improve early identification of high-risk individuals in the future.13,19,41,51,52 Adopting healthy behavioural changes and addressing risk factors such as obesity and a suboptimal cardiometabolic risk profile should be emphasized in the initial stages in managing young-onset hypertension.7,53 In addition to the debate on the necessity of using anti-hypertensive medications in young-onset hypertension, 54 the rationale for treatment such as the timing of intervention, target blood pressure, and choice of medications, remains controversial. Future trials examining the safety and effectiveness of the antihypertensive medications in early-onset hypertension is therefore warranted.47,55,56
Strengths and Limitations
This is a large retrospective cohort in the UK and HK public healthcare systems. The substantial sample size provided sufficient statistical power to determine the association between the age of hypertension onset and various subtypes of outcomes. Hypertension was defined based on multiple blood pressure measurements, anti-hypertensive drug prescription, and a clinical diagnosis documented through ICD/ICPC codes or Read Codes, which may offer greater reliability than self-reported measures. However, there are limitations to this study. Secondary causes of hypertension were not assessed, although patients with secondary hypertension typically comprise approximately 5% to 10% of all cases. 57 While the age of hypertension diagnosis recorded in electronic medical records is used as the proxy for age of hypertension onset in this study, the age at diagnosis may not accurately reflect the true age of onset. The true age of onset can only be determined from repeated measurements beginning from a healthy state, which may not be available from electronic medical records. Blood pressure records used in this study were likely recorded during healthcare visits for reasons apart from hypertension management, therefore, we could expect that the diagnoses made were incidental findings, and the age at diagnosis is likely to lag behind the true age of onset. Consequently, based on our current findings, the HRs reflecting the association between age of onset and adverse outcomes may be slightly underestimated in terms of their magnitude. Data on family history of hypertension and other lifestyle factors such as physical activity and dietary habits were not collected, which may be important confounders in the association between blood pressure and cardiovascular outcomes. As is common with electronic medical records, a significant proportion of the cohort did not have measurements for anthropometry and clinical measurements at the time of hypertension diagnosis (Supplemental Table 3), potentially due to both random and non-random factors. 58 However, comparison of clinical measurements among individuals with and without hypertension using available data (Supplemental Table 3) suggested that the differences in clinical parameters between groups were modest and gradually diminished with age. This study is limited to 2 cohorts from the UK and Hong Kong, which may restrict the generalizability of our findings to broader populations. However, our results align with those of previous studies conducted in the US, Korea, and Chinese cohorts, indicating that these outcomes might be applicable to populations with similar demographic characteristics, such as predominantly Caucasian or Asian individuals in developed countries. By incorporating additional patient characteristics, including smoking status and comorbidities, we enhanced the matching of patients and controls, thereby controlling for variations across different populations. Nonetheless, the relevance of these findings to populations with differing characteristics, particularly in low-to-middle-income countries, warrants further investigation. Finally, the retrospective design of this study precludes any causal inferences.
Conclusion
The relative risks of cardiovascular events and mortality associated with hypertension differ significantly by the age of onset, with stronger associations observed with a younger age of onset and attenuated gradually with increasing age. Early detection through screening for hypertension among high-risk younger adults, and interventions including lifestyle modification could improve blood pressure control at a younger age, potentially mitigating the excess risk for cardiovascular complications and mortality later in life.
Supplemental Material
sj-doc-1-jpc-10.1177_21501319251350091 – Supplemental material for The Impact of Hypertension Onset Age on the Risk of Cardiovascular Diseases and Mortality: Two 10-Year Retrospective Cohort Studies in the United Kingdom and Hong Kong
Supplemental material, sj-doc-1-jpc-10.1177_21501319251350091 for The Impact of Hypertension Onset Age on the Risk of Cardiovascular Diseases and Mortality: Two 10-Year Retrospective Cohort Studies in the United Kingdom and Hong Kong by Ivy Lynn Mak, Boyuan Wang, Kiki Sze Nga Liu, Edmond Pui Hang Choi, Cindy Lo Kuen Lam and Eric Yuk Fai Wan in Journal of Primary Care & Community Health
Supplemental Material
sj-docx-2-jpc-10.1177_21501319251350091 – Supplemental material for The Impact of Hypertension Onset Age on the Risk of Cardiovascular Diseases and Mortality: Two 10-Year Retrospective Cohort Studies in the United Kingdom and Hong Kong
Supplemental material, sj-docx-2-jpc-10.1177_21501319251350091 for The Impact of Hypertension Onset Age on the Risk of Cardiovascular Diseases and Mortality: Two 10-Year Retrospective Cohort Studies in the United Kingdom and Hong Kong by Ivy Lynn Mak, Boyuan Wang, Kiki Sze Nga Liu, Edmond Pui Hang Choi, Cindy Lo Kuen Lam and Eric Yuk Fai Wan in Journal of Primary Care & Community Health
Supplemental Material
sj-docx-3-jpc-10.1177_21501319251350091 – Supplemental material for The Impact of Hypertension Onset Age on the Risk of Cardiovascular Diseases and Mortality: Two 10-Year Retrospective Cohort Studies in the United Kingdom and Hong Kong
Supplemental material, sj-docx-3-jpc-10.1177_21501319251350091 for The Impact of Hypertension Onset Age on the Risk of Cardiovascular Diseases and Mortality: Two 10-Year Retrospective Cohort Studies in the United Kingdom and Hong Kong by Ivy Lynn Mak, Boyuan Wang, Kiki Sze Nga Liu, Edmond Pui Hang Choi, Cindy Lo Kuen Lam and Eric Yuk Fai Wan in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors wish to acknowledge Hong Kong Hospital Authority for the contributions of data extraction. The computations were performed using research computing facilities offered by Information Technology Services, the University of Hong Kong.
Ethical Considerations
This study was approved by the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster and the THIN Scientific Review Committee. All extracted data were anonymous, and no direct patient contact was required, thereby posing minimal ethical concerns. Consent to participate was not required because the data used in this study were anonymized. IQVIA Medical Research Data (IMRD) incorporated data from THIN, a Cegedim Database. References to THIN were intended to describe the data asset licensed by IQVIA. This study has been conducted and reported in accordance with the STROBE guidelines to enhance the clarity and reproducibility of the findings.
Author Contributions
EYFW and ILM contributed to the study design, interpretation of the results and prepared the manuscript. EYFW and BW contributed to the acquisition of data, statistical analysis, and interpretation of the results. All authors contributed to the interpretation of the analysis, critically reviewed and revised the manuscript, and approved the final manuscript as submitted. EYFW is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Excellent Young Scientists Fund, National Natural Science Foundation of China (Principal Investigator: Eric Yuk Fai Wan; Ref No. 82222902). Start-up Fund of the University of Hong Kong (Principal Investigator: Eric Yuk Fai Wan). The funders have no role in the study design, data collection, data analysis, interpretation, and report drafting. The corresponding authors had full access to all the data in the study and took final responsibility for the decision to submit for publication.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EYFW has received research grants from the Health Bureau, the Hong Kong Research Grants Council, Narcotics Division, Security Bureau, Social Welfare Department, Labour and Welfare Bureau of the Government of the Hong Kong SAR and National Natural Science Foundation of China; serves on member of Core Team for Expert Group on Drug Registration of Pharmacy and Poisons Board, and is the director of Advance Data Analytics for Medical Science (ADAMS) Limited (HK), outside of the submitted work. CLKL has received research grants from the Food and Health Bureau of the Government of the Hong Kong SAR, the Hong Kong Research Grant Council, the Hong Kong College of Family Physicians, and Kerry Group Kuok Foundation, outside of the submitted work. The remaining authors have nothing to disclose.
Data Availability Statement
The electronic medical records used in the current are provided by the Hospital Authority of Hong Kong and IQVIA. Data used in this study is not publicly available. Restrictions apply to the availability of these data, which were used under license for this study. The data can be accessed upon request to the Hospital Authority of Hong Kong and IQVIA. The codes used for this study are available online on Github (![]() ).
).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.