
Abstract
Background:
Shortages of pediatric mental health (MH) specialty providers have left pediatric primary care providers (PPCP) to care for the influx of youth with MH needs. This study examined trends in prescription of antidepressants and antianxiety medication in pediatric primary care clinics from 2015 to 2023.
Methods:
Annual rates of prescription of antidepressant and/or antianxiety medication orders were calculated by race/ethnicity, sex, and practice type. Adjusted mean differences (AMD) were calculated and compared for the beginning and end of the study period.
Results:
Prescription orders for antianxiety and/or antidepressant medications increased between 2015 and 2023 across all patients but was greatest among Hispanic youth (AMD = 50.9, 95% CI = 15.3-86.4) and among females irrespective of race (AMD = 29.3, 95% CI = 16.8-41.7). Despite these increases, non-Hispanic White youth were more likely to receive prescriptions than Hispanic and non-Hispanic Asian or Black youth across time periods. Family practices (treating adults and children) had the highest rates of prescription across time periods.
Conclusions:
While prescription rates for antidepressant and antianxiety medications have increased overall, treatment gaps between White and ethnoracially minoritized pediatric patients have persisted. Differences in prescribing patterns between practice environments suggest PPCPs may be more comfortable prescribing MH medications in family practices relative to pediatric practices.
Background
In recent decades, general pediatrics providers in the United States (U.S.) have seen persistent increases in psychological disorders such as anxiety, depression, and suicidal thoughts and behaviors in adolescent and teen patients.1 -5 This coincides with a period of severe shortage of specialty pediatric mental health (MH) providers, especially providers who take private insurance and/or public insurance programs such as Medicaid. 6 As a result, some studies estimate that up to half of children with MH problems do not receive needed treatment, and there have been troubling increases in rates of suicidal behaviors among young people, especially among youth from racially and ethnically minoritized backgrounds.5,7,8 Pediatric primary care providers (PPCP) across the U.S. have been called upon to meet this influx of MH needs; 1 recent study estimated that one-third of all children receiving some form of mental health treatment saw only their PPCP. 9
Despite reliance on PPCPs to meet the MH needs of children and adolescents, a study of pediatricians found that most felt they had not been adequately trained to treat mental/behavioral health problems, with only 10% considering themselves “well prepared” to treat patients with these needs. 10 Some health systems have answered the need for MH treatment through additional training of pediatricians and/or developing specialty provider-to-provider hotlines and other resources for pediatricians to communicate directly with specialists.11,12 A cluster-randomized trial found that integrating behavioral health treatment directly into pediatric primary care practices was both feasible and broadly effective, but this can be a costly approach that may not be possible in lower-resourced settings.11,12 Given the increased demand for MH treatment in primary care and the diverse range of approaches being used by pediatricians, it would be helpful for health systems to understand whether and how, exactly, young patients with MH needs are being treated in primary care. 13
In this work, we seek to leverage electronic health record (EHR) data from a large ambulatory health system, including 8 pediatrics-only and 20 practices that see both children and adults to better understand the landscape of MH treatment in 1 health system. We focus on prescription of medication for anxiety and depression, as these disorders are correlated with suicide risk and are 2 of the more common MH disorders identified in primary care. 14 We will examine trends in prescribing patterns for antianxiety and antidepressant medications among young people over a 9 year period (2015-2023), and explore whether these patterns differ by practice type and/or by demographic and clinical characteristics of patients.
Methods
Patient Population
In this retrospective cohort study, we used outpatient encounter EHR data from a mid-Atlantic health system that includes 40 total locations providing ambulatory, general, and specialty care. Fully de-identified patient data was extracted from Epic, the EHR system used by this system of outpatient clinics since 2013. The study cohort included patient encounters from the 28 largest ambulatory practices in this system, including patients ages 12 to 20 years old, who had a primary care encounter between January 1, 2015 and December 31, 2023.
Analyses included patients who were between 12 and 20 years of age at the time of encounter. These ages were chosen because: (1) 12 years is the age when pediatric patients begin to be regularly screened for depression using the Patient Health Questionnaire (PHQ) and related versions (eg, PHQ-A, PHQ-2, or PHQ-9) in this health system, and (2) young adults often continue to see pediatric providers through the transition to adulthood. 15 A patient was counted as part of the denominator for the annual cross-sectional rates of the outcomes of interest if they had any type of primary care encounter in a given year. A patient was counted as part of the numerator for an annual rate if they had a prescription ordered for an antianxiety or antidepression medication at a primary care encounter in a given year. The institutional review board of the health system approved this study as exempt, due to full de-identification of the data by the institution’s clinical data acquisition team. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines were followed in this work. 16
Measures
Patients were classified as Hispanic if ethnicity was identified as “Hispanic or Latino” in the EHR. Race was defined using the first chosen race category for the child by parent or caregiver upon registration with the health system and patients were classified as Asian if race was identified as any of 13 separate East and South Asian and Pacific Islander choices in the EHR race field. We use the term “Asian” for brevity in this work, while noting that <0.05% of this group were patients who identified as Native Hawaiian or Pacific Islander. Patients with a race or ethnicity that did not fall into any of these categories (American Indian/Alaska Native, “Choose not to disclose,” and “Other”) were classified as “Other race.” Gender was defined using the “sex” variable in the Epic demographic module, which represents the legal gender or sex of the patient as reported by the parent or caregiver upon registration with the health system. More specific information about gender identity was not collected within the Epic EHR system until 2019, and accordingly there is very limited recording of gender subgroups other than “Male” or “Female” (<0.05%). For the purposes of this analysis, the small number patients identifying as “Nonbinary,” “Other,” or “Unknown” in the clinical record were excluded.
Insurance was classified using insurance type at the first encounter with the health system, and was classified as public, private, or other. Other included military/government funded insurances, such as TriCare. National area deprivation index (ADI) was calculated based on the census block group of each patient address and represents an additional dimension of socioeconomic status (SES). 17 Medical complexity was represented in 2 ways; first, we used the Elixhauser score to broadly represent number of comorbidities, which summarizes a patient’s disease burden using 30 conditions identified using ICD codes. 18 Second, we also calculated the number of Complex Chronic Conditions (CCC) recorded for each patient, in order to account for patients with medical complexity. 19 Finally, we used ICD-10 codes to classify specific recorded MH diagnoses, including anxiety, depression, behavioral disorders, substance use, history of suicide-related behavior and schizophrenia (see Supplemental Table 1 for specific coding conventions). Type of clinic was classified as either “Family Practices,” meaning both adults and children are treated at the clinic, and “Pediatric Practices” meaning clinic providers only treat children, teens, or young adults.
The outcome of a medication order for an antianxiety or antidepressant medication was drawn from the medication orders table in the EHR. Antidepressant and/or antianxiety medications were classified using the medication therapeutic class classifications of “antianxiety” or “antidepressant.” As there is a great deal of overlap between types of medications used to treat depression and anxiety (ie, a medication classified as antianxiety may also be used to treat depression symptoms) the 2 therapeutic classes were grouped together for analysis. For purposes of the analysis, the first date of antidepressant and/or antianxiety medication order was used as the beginning of prescription treatment, noting that we do not have information at this time in the EHR about medication adherence.
Analysis
Annual rates (per 1000) of antidepressant and/or antianxiety medication prescription were calculated for each demographic and clinical subgroup of interest, as well as by practice type. These were presented as line graphs to get a better sense of overall unadjusted annual trends. In order to take into account confounding factors, such as age, insurance type, number of encounters during the study period, years from first encounter to last encounter, socioeconomic status and medical complexity (using the Elixhauser score and a count of complex chronic conditions),18,19 we conducted an analysis of the adjusted mean difference (AMD) in prescribing rates. In order to compare rates of prescribing from the beginning of the study period to the end of the study period, 3-year rates were pooled for 2015 to 2017 and 2021 to 2023, and then AMD between these time periods was calculated accordingly with 95% confidence intervals. All analyses were conducted using Stata software, version 18.0. 20
Results
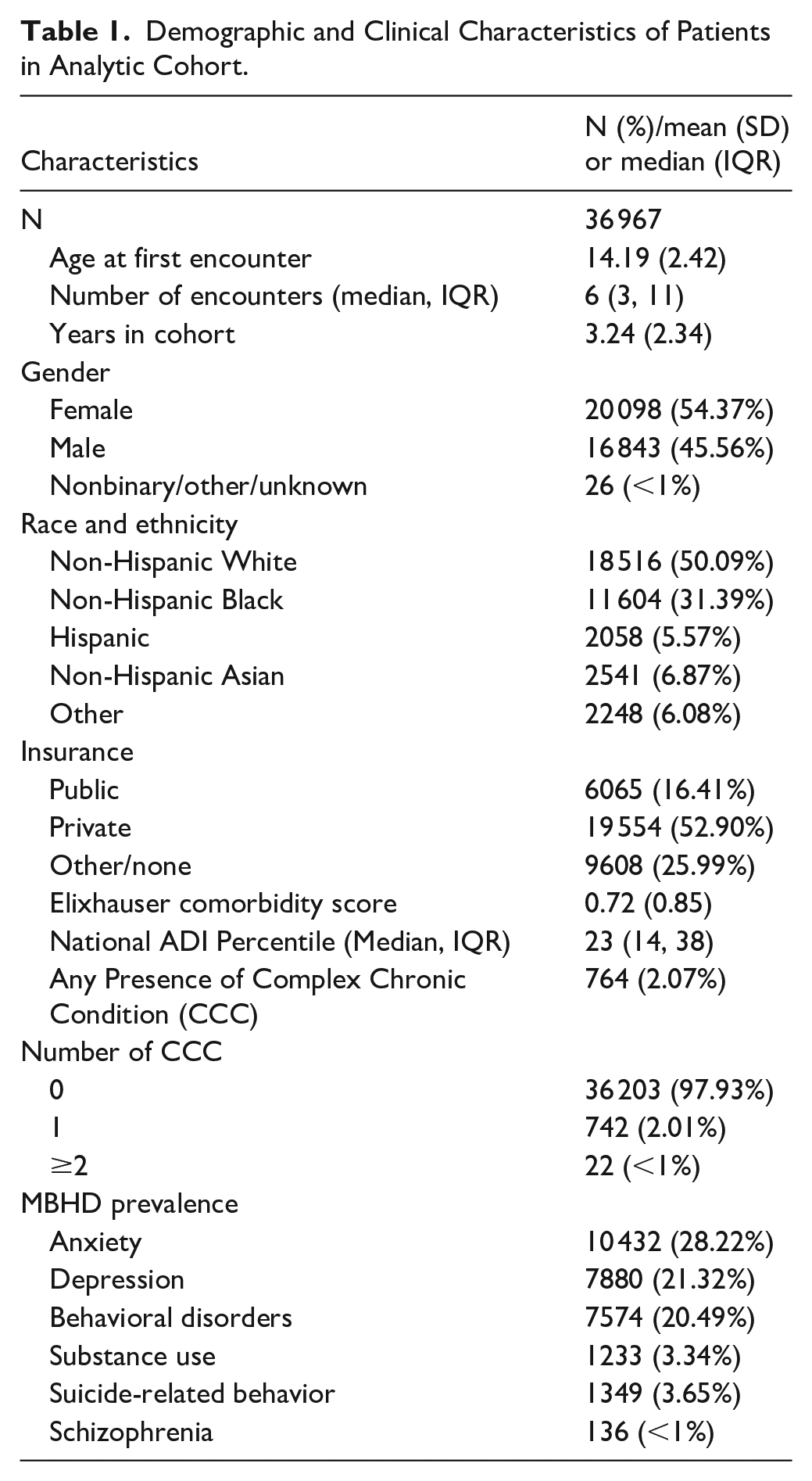
Demographic and clinical characteristics of the study cohort are shown in Table 1. The study sample included 36 967 patients, 54.4% of whom were female, and the median age at first encounter was 14.2 (SD = 2.4). About half of patients identified as non-Hispanic White (50.1%), 31.4% as non-Hispanic Black, 6.9% as non-Hispanic Asian, and 5.6% of patients identified as Hispanic. Most patients had private insurance (52.9%), 16.4% had public insurance, and 26% of patients classified as “Other,” a category largely comprised of government and military insurance. The median number of encounters during the study period was 6 (IQR = 3-11) and the mean time from first to last encounter in the data was 3.2 years (SD = 2.3). Just over 2% of patients had a CCC, with a 28.2% prevalence of lifetime anxiety diagnosis, 21.3% lifetime depression diagnosis, and a 20.5% behavioral disorder diagnosis. Other psychological disorders were less prevalent in this sample; substance use disorder was recorded for only 3.3% of patients and suicide-related behavior was noted for only 3.7% of the study sample.
Demographic and Clinical Characteristics of Patients in Analytic Cohort.
Unadjusted trends in prescribing patterns for antidepressant and/or antianxiety medications can be seen in Figures 1 to 4(c). Figure 1 displays a uniform increase in prescriptions during the study period, and Figure 2 demonstrates that females received prescriptions at higher rates than male patients. Annual trends appear relatively consistent for males and females until 2021, when rates among females spiked considerably, from just over 30 per 1000 to 50 per 1000. This trend was not observed among males, although both groups appear to have a consistent overall peak in 2022. In Figure 3, trends are grouped by type of practice. Family practices started and ended with rates much higher than pediatrics practices, from just over 30 per 1000 to around 50 per 1000. Pediatrics practices also saw increases but went from around 15 per 1000 to just over 30 per 1000. As with the preceding figures, both practice types showed an overall peak in 2022. In Figures 4(a) to (c), trends are grouped by race and sex subgroups. In Figure 4(a), White patients are compared with Black patients, and we see that White females have by far the highest rates of prescription, with a spike seen in 2022, per Figure 2. Black females also had a sustained spike in rates beginning in 2020 while both Black and White males had more modest increases in rates. In Figure 4(b), rates among Hispanic patients are contrasted with White patients, and Hispanic females appear to track somewhat similarly with White females until 2021 whereupon their trajectories diverge as shown, while males in both groups had more modest increases. Finally, in Figure 4(c), we see that Asian females had a spike similar to White, Black, and Hispanic females, though it appears to have begun in 2018.

Overall trend in antianxiety/antidepressant prescriptions, from 2015 to 2023, patients ages 12 to 20 years, n = 36 967.

Trend in antianxiety/antidepressant prescriptions by sex, from 2015 to 2023, patients ages 12 to 20 years, n = 36 967.

Trend in antianxiety/antidepressant prescriptions by practice type, from 2015 to 2023, patients ages 12 to 20 years, n = 36 967.
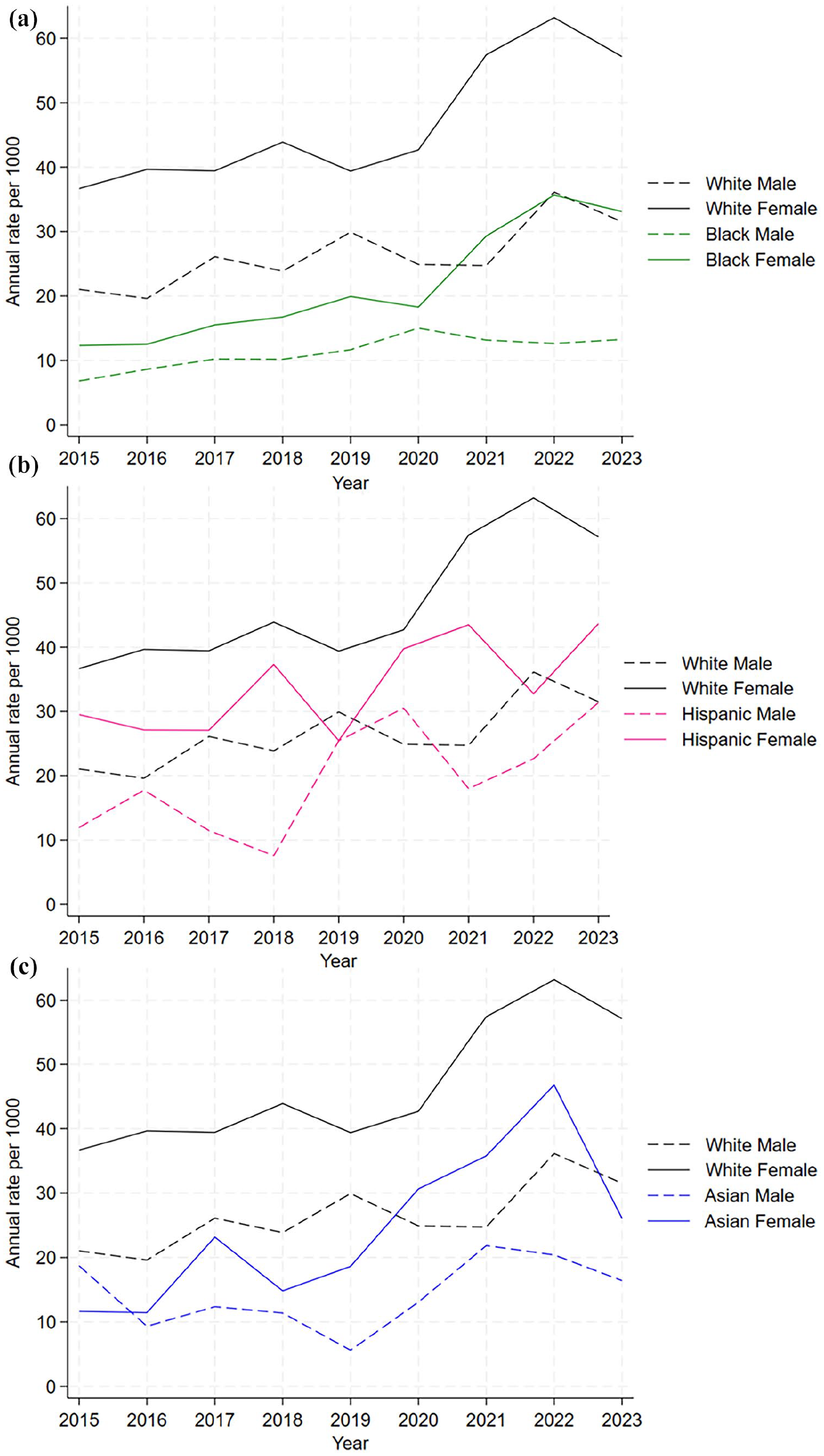
Trend in antianxiety/antidepressant prescriptions by race/sex subgroup from 2015 to 2023, patients ages 12 to 20 years: (a) White and Black males and females, (b) White and Hispanic males and females, and (c) White and Asian males and females.
The results of the pooled AMD analysis comparing prescription rates in the 2015 to 2017 time period with the 2021 to 2023 time period can be found in Table 2. Prescription orders for antianxiety and/or antidepressant medications increased between the 2 time periods across all patients (AMD = 19.9, 95% CI = 11.7-28.2, P < .001), but the increase was greatest among Hispanic youth (AMD = 50.9, 95% CI = 15.3-86.4, P = .005) and females (AMD = 29.3; 95% CI = 16.8-41.7, P < .001). Consistent with the graphical analysis, family practices had the highest rates of prescription in all time periods, going from a rate of 54.4 per 1000 (SE = 3.3) to 78.2 per 1000 (SE = 7.4), representing a significant AMD of 23.9 (95% CI = 7.0-40.8, P = .008). Pediatrics practices went from a rate of 18.1 per 1000 (SE 2.1) to 35.7 per 1000 (SE 3.7), representing a significant AMD of 17.6 (95% CI = 9.2-26.0, P < .001). In the analysis of race and sex subcategories, the only significant increases were among White females (AMD = 36.1; 95% CI = 14.8-57.4, P = .001) and Black females (AMD = 19.2; 95% CI = 3.7-34.7, P = .015).
Adjusted Mean Rates and Differences a per 1000 of First Prescription for Antidepressant, and/or Anti-anxiety, n = 36 967, years 2015 to 2023.
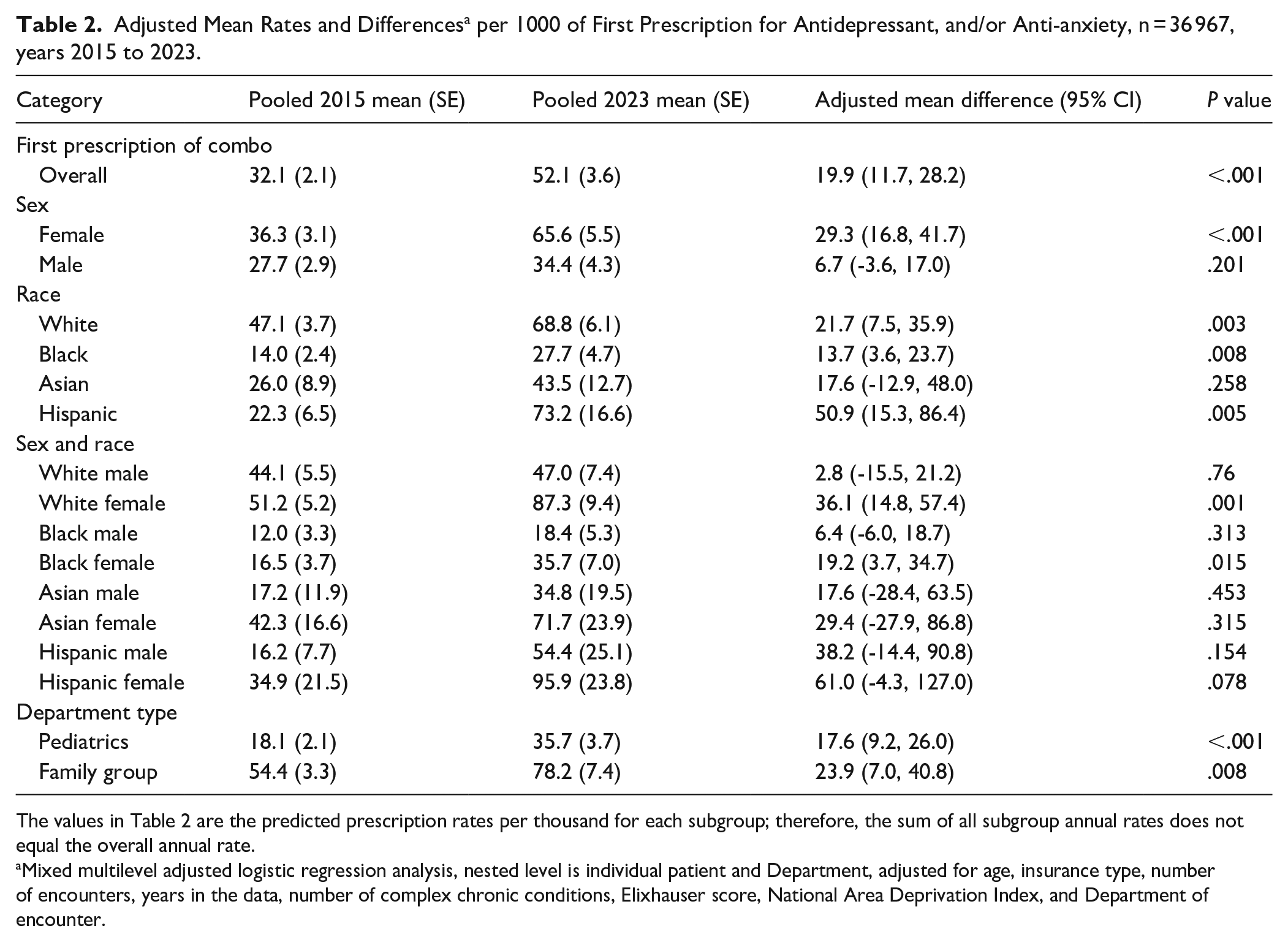
The values in Table 2 are the predicted prescription rates per thousand for each subgroup; therefore, the sum of all subgroup annual rates does not equal the overall annual rate.
Mixed multilevel adjusted logistic regression analysis, nested level is individual patient and Department, adjusted for age, insurance type, number of encounters, years in the data, number of complex chronic conditions, Elixhauser score, National Area Deprivation Index, and Department of encounter.
Discussion
A 2024 study found that nearly 60% of pediatric patients who died by suicide never received any kind of MH treatment, and this rate was even higher among ethnically and racially minoritized youth. 21 Given that 93% of pediatric patients see a PPCP at least once per year, 22 these encounters represent an important opportunity to improve equity in patient care and to save lives. While this study found that rates of prescription of antidepressant and/or antianxiety medications have increased overall, this finding has not reduced the extensive treatment gaps between White youth and those who identify as Asian, Black, or Hispanic. Additionally, we found wide variation in prescribing patterns between different types of practice environments, suggesting varying levels of comfort prescribing MH medications in family practices relative to pediatric practices.
Given the prevalence of MH diagnoses in children, the improved screening occurring in PPC settings, and the limitations in timely MH specialty care, there is an increasing need for pediatric primary care clinicians not only to screen, diagnose, and refer adolescent patients with anxiety and depression, but also to initiate treatment. 23 Guidelines for depression and anxiety treatment in primary care settings state that selective serotonin reuptake inhibitors (SSRIs) should be used when indicated by clinical presentation and patient/family preference.24,25 However when previously surveyed, primary care pediatricians are uncomfortable prescribing medications for depression and anxiety. 26 In our study, we found that rates of prescription of antidepressant and/or antianxiety medications have increased overall from 2015 to 2023. While mood disorders continue to be undertreated in adolescents, our findings on prescribing patterns suggest that comfort and frequency in prescribing is increasing. While we cannot comment on quality of prescribing practices based on our study, there have been recent survey-based and chart review studies that have demonstrated that pediatricians take symptom severity, impairment, and mental health specialty availability into account when initiating treatment.27,28 Notably, our study shows that patients receiving care in family practices were more likely to receive a prescription than in solely pediatric practices. It may be that PPCPs that treat adults are more comfortable with prescribing medications in general and therefore are more likely to prescribe medicines for MH diagnoses in adolescents; however, it is also possible that pediatricians are referring to mental health providers more frequently rather than prescribing medications directly. Further investigation into patterns of prescribing, referrals made by providers, and the related patient outcomes are needed. In addition, efforts in training PPCPs to gain comfort in prescribing would be beneficial, and flexible incremental strategies have been suggested for busy practicing pediatricians including participation in collaborative learning rounds and health system network initiatives to help achieve mental health competencies. 29
Our study adds to growing literature on prescribing practices in primary care settings for adolescent patients experiencing depression and anxiety. Limitations of our study include the use of medication order data, as opposed to filled prescriptions or adherent use of medications, which would have been preferable but were not available in the EHR. We would advocate for continued improvements to EHR integration with health information exchanges, which could integrate pharmacy data into the EHR, allowing future research to account for medication adherence. Secondly, providers may have chosen a nonpharmacologic intervention or a different medication not included in this analysis due to potential concerns about the side effects of specific antidepressants, which may have led to an underestimation of medication prescription. Additionally, we chose to explore adjusted trends in the AMD analysis broadly by pooling 3-year rates for 2015 to 2017 and 2021 to 2023, meaning we did not statistically examine linear trends that may have been occurring on a more granular level, but this is a direction for future research. Additionally, the EHR has very limited data on gender identity for pediatric patients, and we were thus limited to use of binary gender variables, excluding those patients that identified as nonbinary or “other.” It is important that EHR systems continue to improve demographic inclusivity to the extent possible to allow future research to study the unique MH needs and treatment in groups of youth that do not identify as either male or female. Lastly, our study is limited to 1 health system. However, the health system is large with a geographic spread inclusive of diverse patient populations over urban, suburban, and rural practice sites, making the results broadly generalizable to the U.S.
The overall increase that this study found in prescription rates for antidepressant and/or antianxiety medications is consistent with prior literature, and is most likely reflective of fast-paced changes happening in treatment of pediatric MH needs across the U.S.6,9 This study represents a first step in understanding the post-COVID MH treatment patterns impacting U.S. pediatric primary care, yet leaves many questions unanswered. One key question is whether treatment being provided in pediatric primary care is actually helping patients. Previous work has found that the combination of pharmacologic treatment and cognitive behavioral therapy (CBT) is more effective than treatment with antidepressant medication alone,30,31 but the majority of this research has been conducted on adults. It is an important future direction to understand exactly what kind of treatment in addition to medications primary care patients may be receiving and whether and how well different types of treatment are working.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251347906 – Supplemental material for Patterns of Antidepressant and Antianxiety Medication Prescriptions in Pediatric Primary Care in the U.S
Supplemental material, sj-docx-1-jpc-10.1177_21501319251347906 for Patterns of Antidepressant and Antianxiety Medication Prescriptions in Pediatric Primary Care in the U.S by Laura M. Prichett, Andrea S. Young, Ellie Wu, Robert H. Yolken, Emily G. Severance, Juleisa Badio, Meilin Zheng and Tina Kumra in Journal of Primary Care & Community Health
Footnotes
Author Contributions
Laura Prichett and Tina Kumra conceptualized the study, supervised data analysis, drafted the initial manuscript, and critically reviewed and revised the manuscript. Meilin Zheng carried out analyses, drafted all tables and figures, and critically reviewed and revised the manuscript. Robert Yolken, Andrea Young, Emily Severance, Ellie Wu, and Juleisa Badio assisted in the study design and critically reviewed and revised the manuscript for important intellectual content.
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Health /BIRCWH Grant mechanism (Dr. Prichett, K12AR084229), the Stanley Medical Research Institute (grant #7R-1690), and the National Institute of Drug Abuse (Dr. Young, K23 DA044288). This work was also supported by Johns Hopkins Biostatistics, Epidemiology and Data Management (BEAD) Core (internal funding); Dr. Young has received research support from NIH, the Brain and Behavior Research Foundation, Supernus Pharmaceuticals and Psychnostics, LLC. She has served as a consultant to NIH, PCORI, and the Montana State University’s American Indian/Alaska Native Clinical & Translational Research Program, on the Board of Directors for Helping Give Away Psychological Science and on the editorial boards for the Journal of Clinical Child and Adolescent Psychology and Evidence-Based Practice in Child and Adolescent Mental Health. All other authors certify that they have no affiliations with or involvement in any organization or entity with a financial or non-financial interest in the subject matter or materials discussed in this manuscript. The findings and conclusions in this article are those of the authors and do not necessarily reflect the opinions of the National Institute of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this analysis, while fully de-identified, may contain sensitive information and small cell sizes creating the possibility to re-identification of specific patients. The authors do not have the authority or permission to share the data used in this work.
IRB Statement
The Institutional Review Board of Johns Hopkins School of Medicine approved this study as exempt, due to the use of fully de-identified data.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.