
Abstract
Background:
Chronic Kidney disease (CKD) accounts for approximately 82 billion dollars of Medicare spend. Implementing culturally competent, community-based programs may be a strategy for changing utilization behaviors and lowering cost while maintaining quality in this population.
Methods:
A longitudinal claims based study was carried out from April 2023 to August 2024 in the state of CA to assess the impact of the program on cost, utilization, and quality metrics. A propensity matched approach was leveraged yielding of 203 pairs of CKD Medicare Advantage (MA) enrollees. A comparison of the difference of differences was performed between utilization, and available claims-based quality metrics.
Results:
Enrollees in the peer support program, Connect For Life (CFL) generated significantly lower costs of $461 pmpm (95% CI = −1037 to −10 037; P = .016) significantly lower inpatient utilization of 172 per 1000 (95% CI = −10 to −330; P = .037) and significantly higher outpatient utilization of 1212 per 1000 (95% CI = 90 to 2340; P = .035). No differences were found in available quality metrics.
Conclusions:
For CKD MA enrollees in the intervention population, more efficient utilization patterns and lower costs while maintaining quality were observed. The tight propensity match left the study underpowered to detect significant changes for other care settings or individual stages of CKD.
Keywords
Introduction
Healthcare in the United States accounted for 17.3% of gross domestic product in 2020. 1
Patients who are insured by Medicare Advantage (MA; Medicare-approved health plans offered by private companies that cover the same benefits as traditional Medicare and often include prescription drug coverage and additional benefits) represent approximately 33 million US residents and $462 billion (USD) of healthcare spend. The percentage of Medicare eligible participants in a MA plan is slowly increasing, representing roughly 54% of the market, versus the 46% remaining in traditional, fee-for-service (FFS) Medicare. 2
Chronic kidney disease (CKD) is a condition in which the kidneys gradually lose their ability to filter waste products and excess fluid from the blood. 3 End stage Kidney Disease (ESKD) is the progression of CKD to the point where the kidneys have essentially lost all function. 4 Important outcomes for individuals with CKD and ESKD are around slowing progression of disease, reducing cardiovascular events and hospitalization, and managing other side effects such as fatigue and quality of life. 5
CKD and ESKD account for approximately 124 billion dollars of health care spend, 6 or more than a quarter of total Medicare expenditure. Given these global trends, the higher and faster growing spend per MA enrollee when compared to FFS Medicare enrollees, 7 and the financial burden of CKD care, there is a need to continue to pilot and evaluate programs that may drive lower cost more efficient care in the MA market for members with CKD and ESKD whilst maintaining or improving outcomes. This includes in settings not limited to the private insurers that sell MA plans but also the fully capitated provider groups with which these plans typically contract as part of their overall risk-mitigation strategies 8 and to which cost-containment pressures ultimately flow.
Social and Behavioral Drivers of Health (SBDoH) have been shown to effect approximately 80% of outcome and cost variation. 9 Improving these factors was historically not a covered service of payors and providers, and the impact was challenging to quantify. 10 A 68.4% of MA enrollees have 2 or more chronic conditions and 14% of them have CKD 11 Halting progression of chronic conditions like CKD through primary and secondary prevention through use of outpatient settings is a well-established strategy for reducing costs and improving outcomes.12,13
It follows that, for an MA population, an upstream, community-based intervention that tackles SBDoH issues and pushes utilization into outpatient settings where primary and secondary prevention can efficiently occur through building peer support, may be an effective way of favorably bending the cost curve for CKD members and improving outcomes.
Community Engagement Specialists (CESs) within the Connect for Life (CFL) program organize and oversee groups in local communities to foster trusted social connections among peers. These efforts emphasize the value of preventive care, address SBDoH challenges and care barriers, and enhance care navigation and health-related behaviors. The approach encourages members to seek care at more appropriate and efficient locations by leveraging group-based interactions and positive peer pressure. 14 Once trust is built amongst attendees, facilitated by CES staff, positive peer pressure pushes members to act and follow through on health behaviors that are recommended.
CESs are trained in “Wider Circle University,” which follows the 3C national curriculum for community health workers (CHWs) and have the same scope of work. 15 Additionally, Wider Circle CESs are hired from the communities they serve, bringing shared lived experience and deep cultural understanding of local issues and resources, in addition to fluency in the language of the members they serve. This facilitates the establishment of a foundation of trust, which is critical for effectively influencing behavior change.
A significant challenge to this work at present is direct reimbursement for CHWs is only possible in a handful of states. Importantly, even where direct reimbursement is possible, appropriate billing pathways are often limited, making it difficult to meet the needs of members where they are. For example, while California allows for reimbursement for CHWs in Medicaid populations, only 2 codes exist for reimbursement for work done in group-based settings, CPT codes 98961 and 98962 with a cap of 4 members and 8 members respectively, eliminating some of the possible efficiencies upon which Wider Circle’s model is based. 16
For MA populations, similar services can only be billed under a G code, with an initiating event required beforehand, typically in the form of an outpatient primary care or annual wellness event. Reimbursement rates are low which makes the economics challenging for community-based organizations looking to establish sustainable revenue streams. 17 The requirement for an initiating event at a care setting the intervention should be trying to drive members toward, before it has occurred, particularly for a disease like CKD where early intervention to stop disease progression yields better outcomes,12,13 adds additional logistical difficulties. While legislation is continuously evolving, there is no clear pathway for sustainable reimbursement for these services without the need for referrals in MA.
This study reports on a holistic, scalable, group-based community approach that leverages a culturally competent team of CESs to address SBDoH, and drive members into more efficient care environments in a MA population with CKD across a fully capitated provider network.
Methods
A retrospective longitudinal cohort study leveraging claims was used to compare the 2 groups. Study methods are detailed and have been validated in previously published work.18,19 Cleaned claims data was sourced directly from the provider group and stored in a HiTrust certified secure data room. All data was anonymized and only study researchers allowed access.
The intervention group was followed for 12 months from April 1st 2023 with 2 qualifying onboarding interactions within 120 days and at least 1 interaction in the last 90 days to maintain status. A rolling study design was used to ensure complete claims covering the period from April 2023 to August 2024. This maximized the number of participants with 6 cohorts, each starting 1 month after the next, beginning April 1st 2023. The threshold of 2+ interactions was set as a significant threshold for engagement as it was the requirement from the partner provider group for a member to be categorized as engaged. In addition, it was the number of interactions deemed necessary by the team from their previous operational experience to begin to form trust and peer-based influence with the members, which was a key part of the intervention. Qualified interactions included attending an event (virtual or in person), having a discussion around a care gap, a home visit, a care follow up call, or addressing a SBDoH need.
The control group (with at least 12 months of prior health plan membership but not enrolled in CFL) was followed over the same rolling 12-month period for each cohort. Member matching was performed in R using the MatchIT package with a 0.25 caliper. A 1:1 tight caliper matching was used as it introduced less bias. 19 Propensity matching was done across age, sex, comorbidities, baseline utilization patterns, and baseline spend. A difference of differences comparing pre- and post-exposure values between the 2 groups for outcomes of interest was calculated. This methodology has been independently validated as being consistent with typical actuarial practices by Milliman. 19
Study participants were MA members from the state of California enrolled in the same capitated provider group for both exposure and control groups identified as having CKD using ICD-10 codes N18-19.20,21 A total of 203 members were matched to the same number of controls over the period of April 2023 to August 2024. Enrollees in the exposure groups were CFL-eligible members who were previously exposed to CFL. Controls were CFL-eligible members who had never been contacted about nor attended a CFL event. All members in the exposure group were directly invited to participate by the CFL team using multimodal methods.
The CFL program intervention is described in detail in other published work 18 The program involved multiple small groups of approximately twelve enrollees participating in hour-long meetings led by a culturally competent CES, who was sourced, trained, and managed by the CFL team. Each week had different content themes as illustrated in Figure 1 with the overarching theme being to build trust between members through their shared challenges and lived experiences. Once that trust was established members were able to encourage (with guidance from the CES) other members to take positive health actions. Members became part of a larger community after completing their weekly meetings in the smaller group setting. As a part of that larger community, they were invited to participate in health promotion meetings, group physical activities, and peer-to-peer local information exchanges about disease-specific wellness resources. Content across both settings included understanding benefits, understanding the importance of appropriate site of care, changing diet, improving physical activity, practicing gratitude, self-care, and comprehending the importance of screening (see Figure 1).
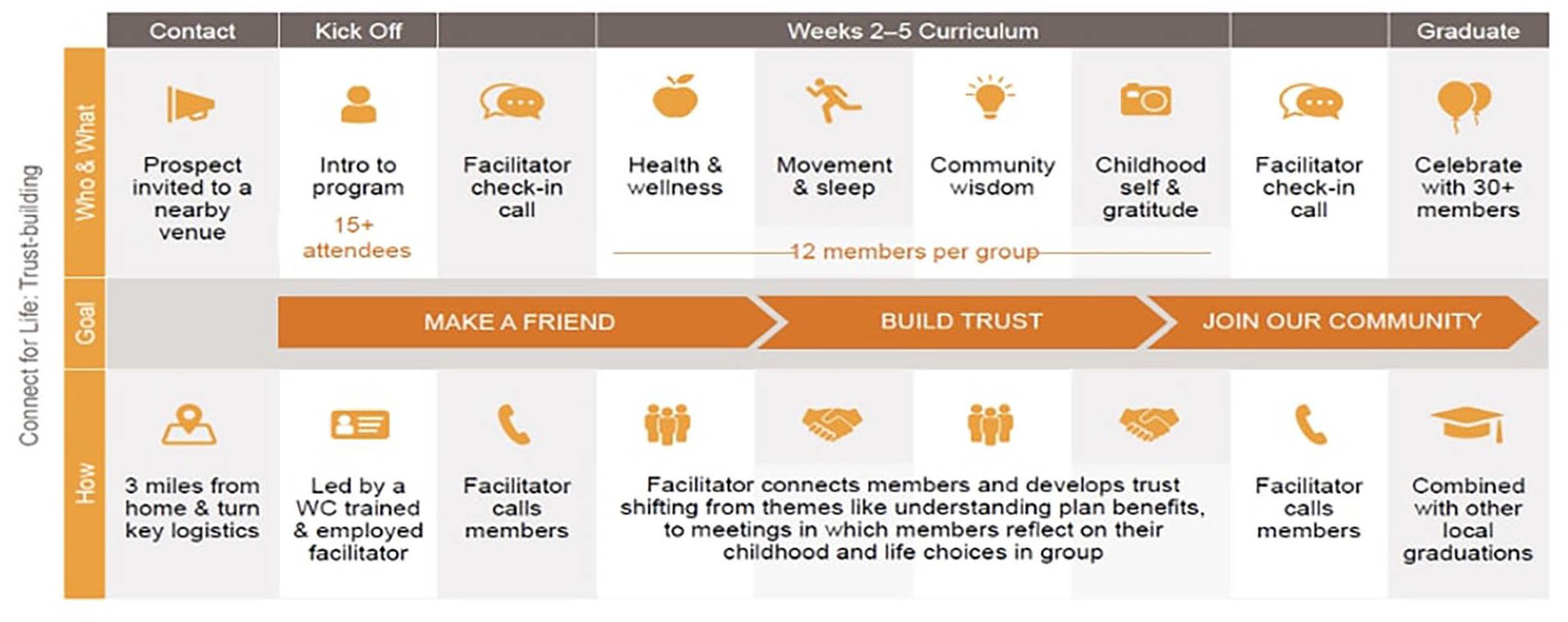
An overview of the Connect for Life community model.
Primary outcomes of interest were related to healthcare utilization (inpatient, outpatient, and non-emergent emergency department) and cost (per member per month). Per member, per month cost (PMPM) was defined as the average monthly cost of a member in USD, summing together all costs in the claims over the study period. Inpatient stays were defined as the number of unique inpatient claims (wherein 1 claim ID related to 1 admission) that occurred in the study timeframe per 1000 members. ED Encounters were defined as the number of unique non-emergent emergency department-related claims (wherein 1 claim ID related to 1 ED event) that appeared in the given timeframe per 1000 members. The NYU algorithm was used to define non-emergent episodes of care. 22 Outpatient Office Visits were defined as the total number of unique claims (with a place-of-service code indicating the visit took place in an outpatient physician’s office wherein 1 claim ID related to 1 office event) per 1000 members. Secondary outcomes of interest were percentage counts of annual wellness visits for eligible members identified through standardized billing codes for these visits in Medicare, with key quality metrics such as flu vaccination and cancer screenings defined by the NCQA. 23 Confounders included age, sex, baseline utilization, paid amounts, and comorbidity score (Charlson Comorbidity Index).
Results
Figure 2 illustrates the waterfall for participants that made up the analysis. Four thousand ninety-nine participants were eligible for the study based on available claims and location of the delivered intervention. One thousand seven hundred forty-eight were removed from this cohort due to having unavailable claims for the complete year prior to the study leaving 2351. A further 401 individuals were removed because their enrollment in the capitation provider group did not meet criteria for sufficient claims within pre-study or study periods to be able to clearly assess the effect of CFL participation on their outcomes. This left 1950 individuals. A further 67 were removed as part of quality control (wherein they were missing key fields required for a 1:1 match), leaving an input data set for matching of 1883 individuals. One thousand six hundred eighty individuals were removed from this intervention pool as they did not meet the 0.25 caliper match leaving 203 individuals matched to 203 controls.

Waterfall of criteria that resulted in 203 matched pairs for the propensity analysis.
Table 1 provides a comparison of baseline characteristics between the exposure group and control. The mean age in each group was 76.8 and 77 years. A 58% were female across both groups. There were no significant differences in Charlson comorbidity scores and there were no significant differences in utilization and paid amounts between the exposure and the control group indicating a successful match.
Comparison of Baseline Characteristics Between Exposure Group and Control.

Continuous variables: P-value for difference calculated from unpaired Welch’s T-test.
Table 2 details the comparison between exposure and control groups for outcomes of interest. After 1 year, the CFL exposure was correlated with significantly higher outpatient utilization in the exposure group vs control of 1212 per 1000 (95% CI = 90 to 2340; P = .035) and significantly lower inpatient utilization of 172 per 1000 (95% CI = −10 to −330; P = .037). Overall pmpm cost was also significantly lower by $461 (95% CI = −1037 to −10 037; P = .016) in the intervention group when compared to controls. No significant differences were found across any quality metrics or non-emergent ED utilization.
Comparison of Exposure Group and Control for Outcomes of Interest.
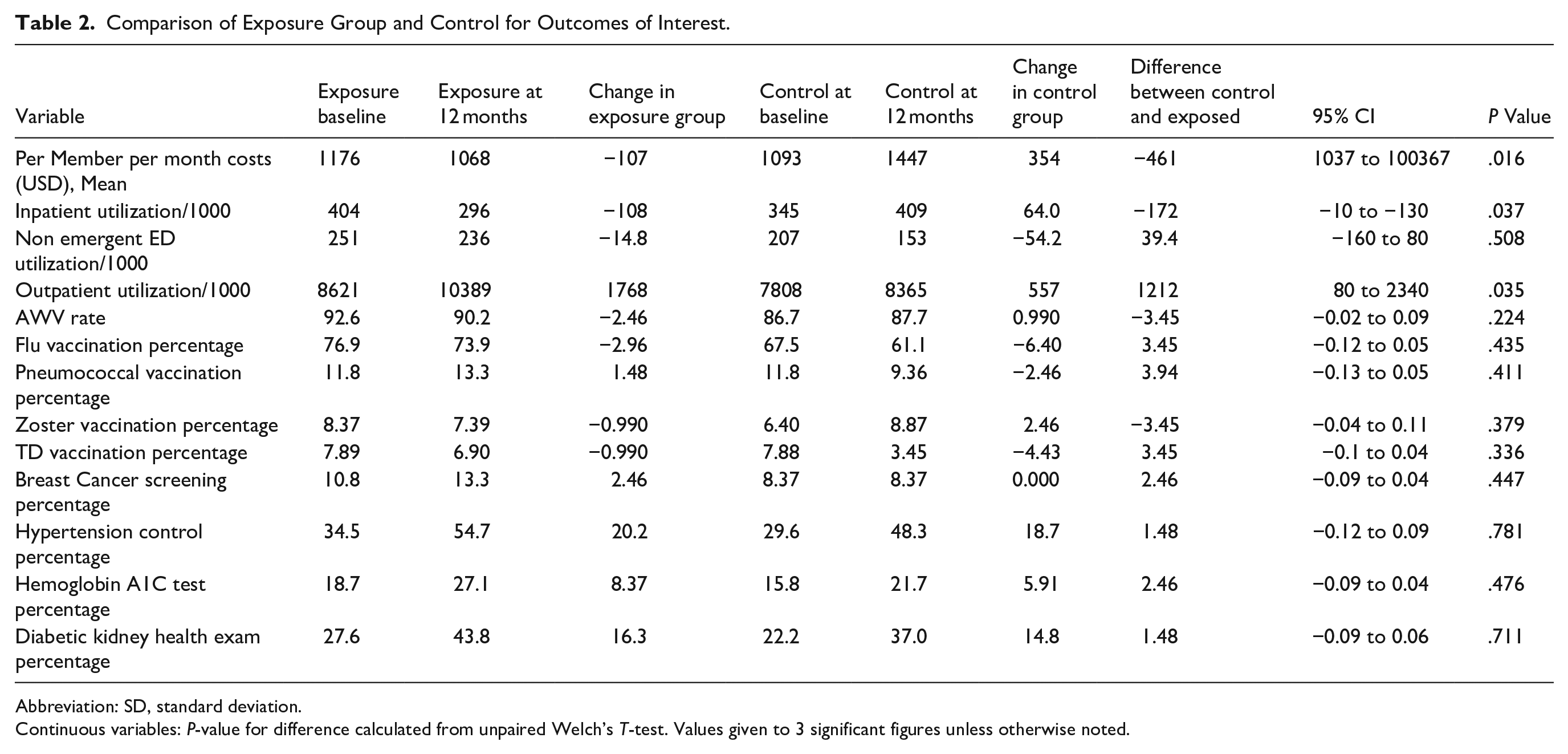
Abbreviation: SD, standard deviation.
Continuous variables: P-value for difference calculated from unpaired Welch’s T-test. Values given to 3 significant figures unless otherwise noted.
In summary the results show shifts of utilization to outpatient settings from inpatient settings, reductions in overall spend, whilst maintaining quality metrics.
Discussion
Recipients of CFL generated significantly lower costs of $461 pmpm (95% CI = −1037 to −10 037; P = .016) significantly lower inpatient utilization of 172 per 1000 (95% CI = −10 to −330; P = .037) and significantly higher outpatient utilization of 1212 per 1000 (95% CI = 90 to 2340; P = .035) with maintained quality metrics when compared to controls.
The study suggests that a community-based exposure may be effective for this CKD MA population in pushing healthcare utilization toward favorable locations and lowering overall costs. This is consistent with existing research. 24 Prior research has shown that CHW-led programs can significantly reduce hospital admissions and increase engagement with primary care in patients with multiple chronic conditions, including CKD. 25 Additionally, targeted community-based interventions addressing social determinants of health have been associated with reductions in total healthcare spending among Medicare and Medicaid populations. 26 The culturally competent and hyperlocal model utilized in the Connect for Life (CFL) program builds on these findings by embedding trusted community engagement specialists with shared lived experience into the peer groups. This may enhance cohesion and activate health-promoting behaviors, consistent with peer influence and positive deviance frameworks. Collectively, these may support the effectiveness of peer-based, community-embedded approaches in promoting more efficient, preventive care utilization patterns, particularly for high-risk populations such as those with CKD.
The underlying mechanism of this positive deviance theory in action may be driven by 2 factors. First, the intentional grouping of members by shared lived experience such that they would be likely to form social connections had they met organically in real life. This created an environment where trust was more likely to form, and positive deviance and social pressure could be effective for difficult to modify health behaviors amongst those members with CKD. Second, the unique facilitation of the groups by the Wider Circle CESs who are experts in group-based support who’s profile was hyper local. This enabled appropriate health care navigation, cultural competence, and local understanding of resources in the community that could be leveraged to promote access and literacy in the CKD population.
There were several limitations with the study. Selection bias may have been present as those attending groups could have been further along the transtheoretical model of change through the commitment to coming to an event and therefore more likely to take benefiting actions. This could explain the improvement observed. 27 Through using a narrow caliper for the propensity match, efforts were made to minimize this potential selection bias. 19 The small study number that occurred as a result of the tight matching will have likely led to the study being underpowered and unable to detect significant differences that may have been present that trended positively (or negatively). The limitations on availability of baseline characteristics in the claims for this population could have led to an imperfect match, resulting in systematic differences between the groups which may have biased the results in either direction. Finally, not enough longitudinal data was present to conduct a dose response analysis where differences in the number of events and outcomes could be understood and whether the relationship was linear or multiplicative.
Conclusion
Our study found that leveraging a community-based program that addresses health behaviors may be an effective strategy for changing utilization patterns and lowering costs in the CKD MA population. Future studies including a dose response analysis would be helpful to understand the effects of each additional attendance and whether the intervention behaves in a linear or multiplicative manner. In addition, larger studies looking at different stages of CKD could tease out differences in impact depending on disease severity and access and linkage to hospital records to compare mortality rate, length of stay and other important outcomes would be meaningful versus those limited to the claims. The role of a CHW-like health navigator staff in facilitating such changes in these settings may have been crucial and a comparison study between groups run by our CESs and groups without them would be useful to understand their influence. Contracting with existing community-based services to better manage care efficiency and push members to outpatient and lower cost settings for patients with CKD could be a viable strategy to bend the cost curve favorably. Policy makers could look at the efficacy of group based CHW interventions and create more flexible reimbursement arrangements for MA populations. At present, the need for an initiating event in the outpatient environment ahead of the intervention leaves the cart before the horse in terms of driving better utilization and getting folks into upstream interventions in the community before they enter traditional care environments. This is particularly relevant with a disease like CKD where earlier intervention is critical in managing disease progression.
Footnotes
Acknowledgements
None.
Ethical Considerations
Our study complied with all guidelines and ethics for responsible use for a study using retrospective anonymized insurance claims with no patient identifiable information. It did not require IRB approval as all claims were anonymized and no human or animal subjects were used in the course of the research.
Author Contributions
All authors contributed per ICMJE guidance. CP and KW wrote the manuscript. FG, JZ, and TC conducted the analysis.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CP, FG, JZ, TC, and KW are employees of Wider Circle, the company that provides “Connect for Life.”
Data Availability Statement
Study used retrospective anonymized insurance claims with no patient identifiable information.