
Abstract
Objective:
This study aimed to examine the intrinsic capacity in Chinese older adults and its determinants (sociodemographic, lifestyle-related, environmental, and health-related factors) based on the WHO Integrated Care for Older People (ICOPE) framework.
Methods:
A cross-sectional community-based study was conducted among 485 community-dwelling older adults recruited from 4 community health service centers in Xinxiang City, Henan Province between August 2024 and February 2025. Intrinsic capacity was assessed across 5 domains: locomotion, cognition, vitality, psychology, and sensory capacity (hearing and vision). Structural equation model (SEM) was used to examine relationships among intrinsic capacity, sociodemographic factors, lifestyle, family support, social participation, healthcare access, and health conditions.
Results:
More than a half of subjects were female (61.2%), married (84.7%), having less than high school education (52%), with a mean age of 73.7 years (SD = 5.5). About 55.9% showed intrinsic capacity impairment, with most impairment of cognition (49.9%), followed by vision (44.9%), hearing (23.7%), locomotion (22.5%), vitality (18.1%), and psychological capacity (13%). The SEM demonstrated good fit and explained 83% of the variance in intrinsic capacity. Significant determinants, ranked by effect size, included dietary habits (β = .544), age (β = −.303), pain (β = −.240), handgrip strength (β = .205), social participation (β = .181), access to healthcare services (β = .138), hospitalization (β = −.10), and physical exercise (β = .089). All paths in the model were statistically significant ( p ′ 0.05).
Conclusions:
The SEM analysis demonstrated that dietary habits, handgrip strength, social participation, access to healthcare services, and physical exercise were positively associated with intrinsic capacity, while age, pain, and hospitalization showed negative associations. These findings suggest that primary care approaches focusing on multi-domain interventions, particularly health promotion, self-care, and early screening, may be promising areas for future public health initiatives. Community-based programs integrating these modifiable factors should be prioritized to promote intrinsic capacity and functional independence among Chinese community-dwelling older adults.
Keywords
Introduction
Population aging presents unprecedented challenges to global health and social care systems, with the proportion of adults aged 60 years and older projected to increase from 12% to 22% between 2015 and 2050. 1 The rising socioeconomic burden on healthcare systems was closely linked to increased prevalence of multimorbidity and disability in populations with high life expectancy. However, traditional disease-centered approaches to aging research have proven insufficient, as the absence of disease does not necessarily indicate healthy aging. 2 In response to this evolving healthcare landscape, the WHO introduced a groundbreaking model in 2015 that shifts emphasis from disease-centered to function-centered paradigms. 3 This model defines healthy aging as “the process of developing and maintaining functional ability that enables well-being in older age.” Central to this model is intrinsic capacity—the composite of all physical and mental capacities that individuals draw upon throughout their life course—encompassing 5 key domains: locomotion, vitality, cognition, psychological well-being, and sensory function. 4
The WHO has published the Integrated Care for Older People (ICOPE) framework to guide assessing and promoting intrinsic capacity of older adults. 5 Within ICOPE, the assessment of intrinsic capacity involves in-depth evaluation across 5 domains using standardized measurements. This approach serves as a valuable tool for promoting healthy aging by identifying and addressing declines in intrinsic capacity, thereby facilitating more person-centered and effective interventions. A decline in 1 or more of the 5 domains is considered to constitute intrinsic capacity impairment. A recent meta-analyze has revealed concerning prevalence rates, with 67.8% of community-dwelling older adults globally and 66.0% in China experiencing intrinsic capacity impairment. 6 This impairment triggers a broad spectrum of adverse outcomes, including functional decline, frailty, mortality, poor quality of life, and so on. 7 Identifying key determinants that influence intrinsic capacity is therefore essential for developing targeted screening protocols and interventions that mitigate functional decline, preserve independence, and optimize quality of life among older adults.
Recent studies have explored various factors associated with intrinsic capacity among community-dwelling older adults, primarily focusing on sociodemographic characteristics (eg, advanced age and education), lifestyle behaviors (eg, tobacco use and alcohol consumption), and health indicators (eg, comorbidity and handgrip strength).8,9 However, a critical limitation persisted: most studies have inadequately addressed environmental influences on intrinsic capacity. 10 The International Classification of Functioning, Disability and Health (ICF) framework highlights environmental contexts as significant contributors to intrinsic capacity, emphasizing the dynamic interaction between these external factors and individual health conditions. 11 This consideration is particularly relevant in China, where the “90-7-3 model” indicates approximately 90% of older adults rely on family-based care and 7% on community-based services, highlighting the critical role of family and community support. 12 Additionally, research has demonstrated that health service access—including geographic accessibility, service availability, and financial affordability—significantly impacted health outcomes in older populations. 13 Despite their importance, these environmental determinants remain understudied in current research. Compared to general regression analysis, structural equation modeling (SEM) offers distinct advantages 14 by enabling the examination of interdependent relationships among multiple influencing factors and their simultaneous impacts on intrinsic capacity. Furthermore, SEM allows intrinsic capacity to be conceptualized as a latent variable measured through 5 domains, which aligns with the theoretical framework of intrinsic capacity as a holistic construct. Moreover, existing studies have disproportionately focused on either economically advantaged urban centers like Beijing or economically disadvantaged rural areas,15,16 with limited evidence from medium-sized Chinese cities. As a third-tier city in central Henan, Xinxiang represents an intermediate level of economic development. Furthermore, its demographic structure closely mirrors Henan Province’s aging pattern, with 17.68% of its 6.17 million permanent residents aged 60 years and above, and 13.04% aged 65 years and above, perfectly aligned with provincial average. 17 Therefore, this study selected Xinxiang City in Henan Province as the research location, filling a critical research gap between China’s economically advantaged urban centers and disadvantaged rural areas.
This study, adopting the WHO ICOPE framework, assessed intrinsic capacity impairment and investigated the relationships among intrinsic capacity, sociodemographic factors, lifestyle behaviors, family support, social participation, healthcare access, and health conditions using SEM. The research was conducted among community-dwelling older adults in Xinxiang City, Henan Province.
Methods
Design and Sample
This cross-sectional study involved older adults from Xinxiang City who were selected through a multi-stage cluster sampling approach. First, all 4 administrative districts of Xinxiang City were included to ensure comprehensive geographic representation. Second, 1 community health service center was randomly selected from each district, resulting in 4 centers for data collection. Finally, we extracted a complete list of elderly residents from each center’s electronic health records and used computer-generated random number tables to select participants according to predetermined sample sizes. Selected individuals were contacted by telephone, informed about the study, and provided informed consent prior to participation.
Data collection occurred from September 2024 to February 2025, with face-to-face surveys conducted by trained researchers at either community health centers or participants’ homes according to participant preference. Physical assessments were carefully monitored to ensure participant safety, and researchers provided emotional support particularly during sensitive assessments such as the Geriatric Depression Scale. For quality control, data was independently entered by 2 research assistants to ensure consistency in data entry.
Study Participants
Study participants included older adults (≥65 years) registered with 4 community health service centers in Xinxiang City from August 2024 to February 2025. Those who met the inclusion criteria were invited to participate in the study. Eligibility required Chinese language proficiency and voluntary consent. Individuals with severe mental disorders, significant language/hearing impairments, or totally dependent living status (Katz ADL ≤2) were excluded. Face-to-face questionnaire surveys were conducted, yielding 485 valid responses from 500 distributed questionnaires.
Measures
Intrinsic capacity was evaluated across 5 domains as recommended by the ICOPE: vitality, cognition, locomotion, psychological, and sensory capacities. The vitality domain was assessed using the Short-Form Mini Nutritional Assessment (MNA-SF). 18 Cognitive capacity was measured through the Montreal Cognitive Assessment—Basic (MoCA-B), with scoring criteria adjusted for participants’ educational levels. 19 Locomotion was evaluated using the Short Physical Performance Battery (SPPB). 20 The psychological domain was assessed with the Geriatric Depression Scale-15 (GDS-15). 21 Finally, the sensory domain, encompassing both visual and hearing capacities, was evaluated using the E visual acuity chart and Finger rub test with supplementary self-reported questions.22,23 Each domain was scored on a scale of 0 to 2 points, where 0 represented severe impairment, 1 indicated mild or moderate impairment, and 2 reflected normal function. The total intrinsic capacity score ranged from 0 to 10 points, with higher scores indicating better functional capacity. Participants scoring between 0 and 8 were classified as having intrinsic capacity impairment.
Sociodemographic factors included age, sex, educational level, marriage, monthly income, income sufficiency, and living arrangements.
Lifestyle-related factors included physical exercise, sedentary time, dietary habits, sleep habits, alcohol drink, and smoking habits. Physical exercise was assessed through 3 items measuring frequency of vigorous, moderate, and light exercises (scores = 3-12, higher indicating greater exercise). Sedentary time quantified daily minutes spent in activities such as watching TV, reading, using computers, or doing handcrafts. Dietary habits were evaluated using a 10-item questionnaire assessing adherence to recommended intake across food groups (grains, vegetables, fruits, soy products, eggs, meat, fish, dairy, oil, and salt), with total scores ranging from 10 to 40 (higher scores indicating better adherence to dietary guidelines).
Environmental factors included family support, social participation, and access to health services. Family support was assessed using family APGAR questionnaire measuring satisfaction with family functioning, with scores ranging from 0 to 10 (higher scores indicating greater satisfaction). 24 Social participation was measured using a scale assessing engagement in diverse activities, with scores ranging from 8 to 40 (higher scores indicating greater participation). 25 Healthcare service access was evaluated through 3 items measuring geographic accessibility, service availability, and financial affordability, with scores ranging from 3 to 8 (higher scores indicating better access). 13
Health-related factors included illness (number of physician-diagnosed conditions), pain presence, pain scale (Visual Analog Scale), sleep quality satisfaction, handgrip strength (kg, measured twice from dominant hand), hospitalization, and falls (number in past 1 year).
Statistical Analysis
Statistical analyses were performed using SPSS 26.0 and Amos 26.0 software. Independent samples t-tests were used to compare mean differences in intrinsic capacity between 2 groups. One-way analysis of variance (ANOVA) was employed to assess mean differences in intrinsic capacity among 3 or more groups. Spearman correlation analysis evaluated relationships between continuous independent variables and intrinsic capacity. Effects with P < .05 were considered statistically significant.
SEM was employed for path analysis to explore the direct effects of sociodemographic, lifestyle-related, environmental, and health-related factors on older adults’ intrinsic capacity. Model fit was evaluated using multiple indices: a χ2/df ratio <5, Root Mean Square Error of Approximation (RMSEA) values ≤0.08, and values ≥0.90 for Comparative Fit Index (CFI), Goodness of Fit Index (GFI), Adjusted Goodness of Fit Index (AGFI), and Tucker–Lewis Index (TLI) were considered indicative of good fit. This article is in accordance with the STROBE guidelines.
Ethical Approval
Ethical approval was obtained from the Xinxiang Medical University Ethics Committee (XYLL-20240279) and the Ethical Review Committee for Human Research, Mahidol University (MUPH2024-081).
Results
The sample comprised 485 older adults aged 65 to 91 years (73.7 ± 5.5), with a majority being female (61.2%) and married (84.7%). Sociodemographic characteristics were shown in Table 1.
Sociodemographic Characteristics (N = 485).

Intrinsic capacity scores in the study population ranged from 0 to 10 (mean = 7.97 ± 1.81), with 55.9% of participants (n = 271) displaying impairment (scores ≤ 8). The prevalence rates of impairment were 57.1% for sensory capacity (n = 277), 49.9% for cognition capacity (n = 242), 22.5% for locomotion capacity (n = 109), 18.1% for vitality capacity (n = 88), and 13% for psychological capacity (n = 63). Regarding sensory capacity specifically, vision impairment was observed in 44.9% of participants (n = 218), while hearing impairment was present in 23.7% of participants (n = 115).
Univariate analysis revealed that intrinsic capacity scores were significantly associated with several participant characteristics (Table 2). Educational level, marriage, sleep habits, pain presence, sleep quality satisfaction, and history of hospitalization all demonstrated significant relationships with intrinsic capacity scores (all P < .05).
Association Between Categorical Independent Factors and Intrinsic Capacity (n = 485).
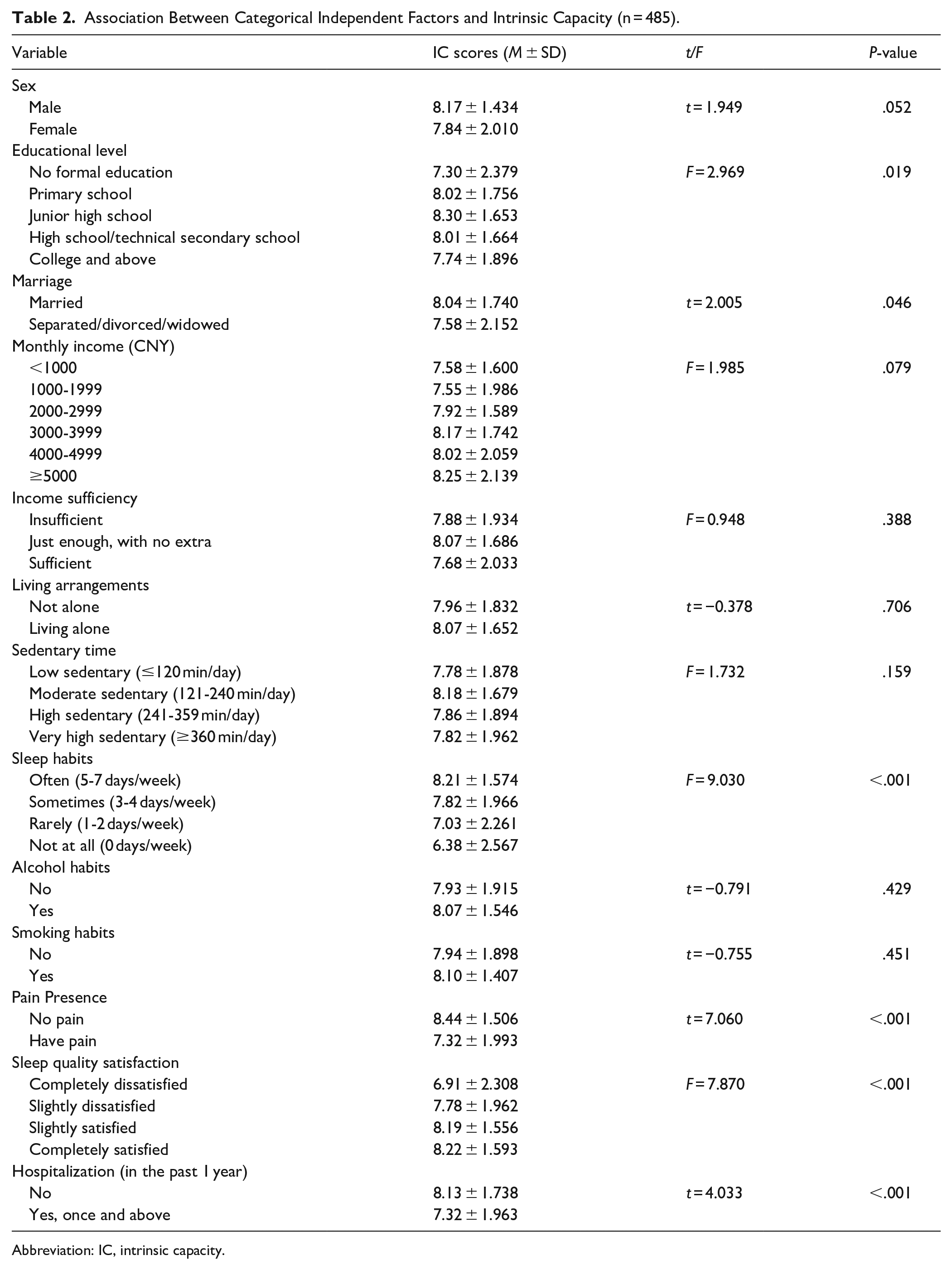
Abbreviation: IC, intrinsic capacity.
As shown in Table 3, Spearman correlation analysis revealed several significant associations with intrinsic capacity. Dietary habits demonstrated the strongest positive correlation (r = .525), followed by weaker positive associations with handgrip (r = 0.259), access to health services (r = .200), social participation (r = .154), and physical exercise (r = 0.141; all P ≤ .01). Among negative correlations, pain scale (r = −.308) exhibited moderate inverse relationships, while age (r = −.296) and illness (r = −.159) showed comparatively weak negative associations (all P < .001).
Correlation Between Continues Independent Variables and Intrinsic Capacity (N = 485).

Family support (r = .078) and falls (r = −.085) showed no significant correlation (all P > .05).
In the SEM, intrinsic capacity was operationalized as a latent variable measured by 5 domains. The model was refined using Modification Indices to establish covariance relationships between variables and non-significant paths (P ≥ .05) were removed to derive the final model (Figure 1). Path coefficient significance was assessed using bootstrap analysis, with results presented in Table 4.
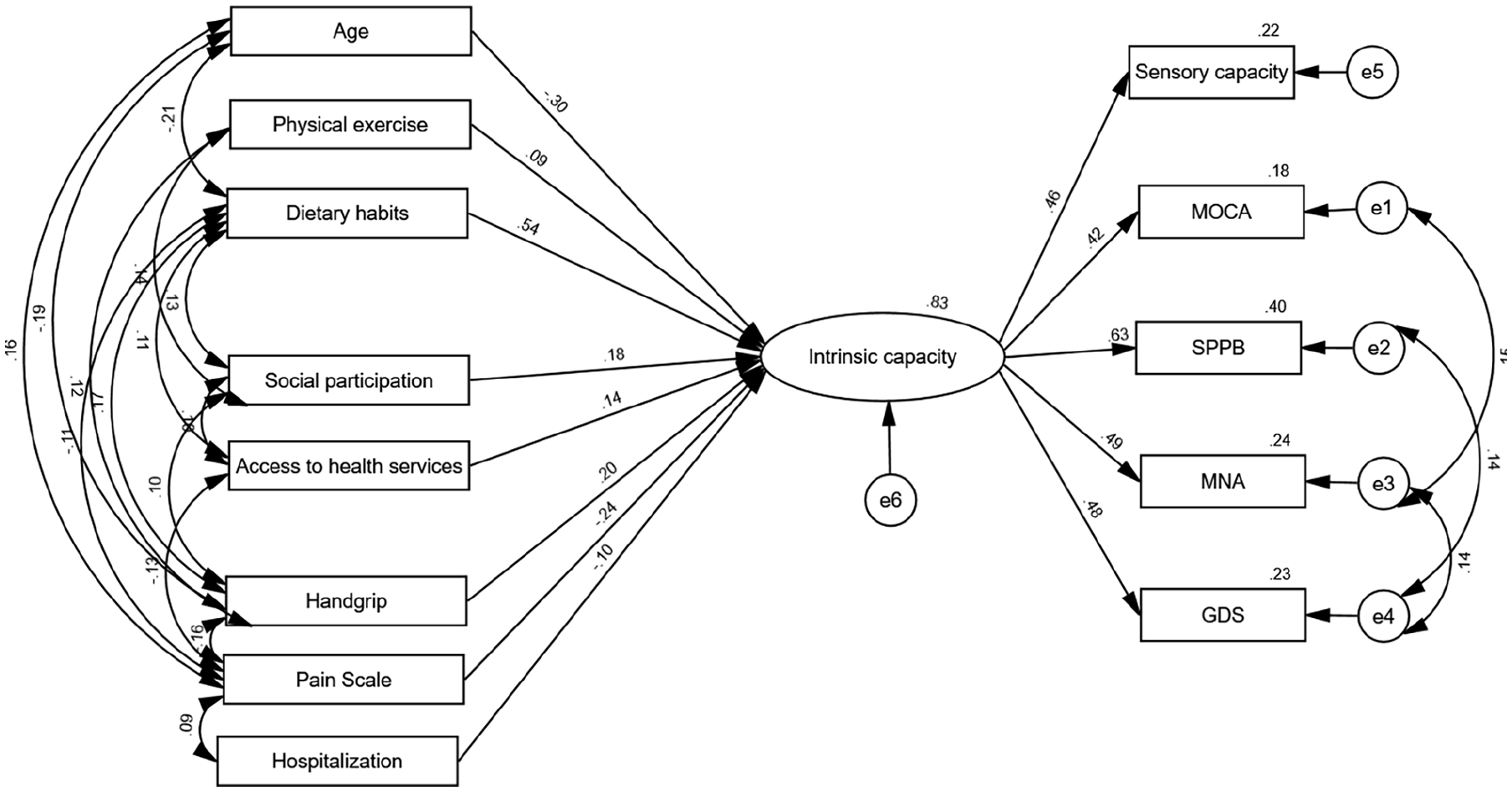
Modified model with standardized parameter estimates.
Direct Effects of Variables in the Model (N = 485).

Abbreviation: IC, intrinsic capacity.
The final SEM demonstrated good fit: χ²/df = 2.752, GFI = 0.960, AGFI = 0.924, CFI = 0.904, TLI = 0.844, and RMSEA = 0.060 (90% CI = 0.048, 0.073).
The 8 factors in the final model explained 83% of intrinsic capacity variance, highlighting their critical roles in determining intrinsic capacities among older adults. Dietary habits exerted the strongest positive effect (β = .544, P = .009), followed by handgrip strength (β = .205, P = .010), social participation (β = .181, P = .013), access to health services (β = .138, P = .009), and physical exercise (β = 0.089, P = .020), indicating that better dietary habits, stronger grip strength, higher levels of social engagement, greater healthcare accessibility, and more frequent physical exercise were associated with enhanced intrinsic capacity among older adults.
Conversely, age (β = −.303, P = .020), pain intensity (β = −.240, P = .007), and recent hospitalization (β = −.100, P = .026) demonstrated negative effects on intrinsic capacity, indicating that advancing age, increased pain levels, and recent hospitalization experiences were associated with diminished intrinsic capacity in older adults.
Discussion
Our study found an intrinsic capacity impairment prevalence of 55.9% among community-dwelling older adults, comparable to the 55.0% reported in a global meta-analysis, 26 but lower than the 67.8% found across 5 countries including China 6 and the 87.8% reported in Mexico. 27 Conversely, our finding exceeds the 39.9% prevalence in the China Comprehensive Geriatric Assessment Study. 28 Regarding specific intrinsic capacity domains, the order of impairment prevalence from highest to lowest—sensory, cognitive, locomotion, vitality, and psychological—matches the sequence reported in a previous study. 26 These variations likely reflect our medium-sized city context, addressing a gap between previous studied focused primarily on metropolitan centers or rural areas in China.
The SEM demonstrated good fit and explained 83% of the variance in intrinsic capacity. It validates the comprehensive impact of sociodemographic factors, lifestyle-related factors, environmental factors, and health-related factors on intrinsic capacity, as conceptualized in the ICF framework. Furthermore, our findings support ICOPE’s emphasis on comprehensive assessment across multiple domains, as evidenced by the significant pathways from intrinsic capacity to its measurement constructs: sensory capacity, cognitive function (MOCA), physical performance (SPPB), nutrition (MNA), and psychological status (GDS). 5
Among sociodemographic factors, age emerged as the sole significant variable in the SEM, negatively influencing intrinsic capacity. This finding aligned with previous researches showing that aging both negatively impacted composite intrinsic capacity scores and increased the risk of its domain impairments.6,9,27 This trend was confirmed in China, where intrinsic capacity impairment prevalence increased from 28.6% in adults aged 60 to 64 years to 66.6% in those over 80 years. 28 Age impacted intrinsic capacity through physiological decline, chronic disease accumulation, and deterioration in cognitive, sensory, and psychosocial functions. 29 Marriage and education showed significant associations with intrinsic capacity in univariate analysis but not in the final model. Married participants demonstrated better intrinsic capacity, likely due to mutual care and emotional support between spouses. 30 Unexpectedly, the univariate analysis revealed a significant but non-linear relationship between educational level and intrinsic capacity: those with no informal education scored lowest, junior high school graduates scored highest, while those with college education and above showed a decline. This pattern may be attributed to moderate education enhancing intrinsic capacity in older adults, while higher education’s additional benefits may be moderated by other factors such as occupational stress and lifestyle changes. Further research is needed to better understand these relationships. Sex, income, and living arrangements showed no significant associations.
Regarding lifestyle factors, dietary habits, and physical exercise demonstrated significant positive effects on intrinsic capacity in SEM. Our findings aligned with a previous research demonstrating that “fruits and vegetables” and “protein-rich” dietary patterns improve intrinsic capacity. 31 Notably, our dietary assessment were based on Chinese Dietary Guidelines focusing on overall dietary balance, offering greater ecological validity than research on specific nutrients. A balanced diet provides comprehensive nutrition, including high-quality protein, essential micronutrients, and dietary fiber—crucial elements for maintaining physiological functions and promoting overall health. Physical exercise benefits likely stem from enhanced cardiorespiratory function, increased muscle strength, elevated brain-derived neurotrophic factors, and improved mental health. 32 Sleep quality correlated with superior intrinsic capacity in univariate analysis, while sedentary time, alcohol consumption, and smoking showed no significant associations. A longitudinal study supports the relationship between sleep and intrinsic capacity, finding that maintaining 7 to 8 h of sleep duration helps maintain optimal intrinsic capacity or delays its decline, while excessive (>10 h) and insufficient (<6 h) sleep negatively impact intrinsic capacity. 33 This relationship likely exists because healthy sleep habits enhance cognitive function, while poor sleep quality correlates with depression in older adults. 34
Environmental factors analysis revealed that social participation and access to healthcare services positively influenced intrinsic capacity in SEM. Enhanced social participation serves as a protective factor against declining intrinsic capacity. This aligns with evidence that social engagement reduces cognitive impairment risk, fulfills belonging needs, and mitigates depression, while social isolation negatively impacts capacity. 35 Healthcare accessibility significantly impacts intrinsic capacity, with evidence showing that proximity to healthcare facilities correlates with maintained physical capacity and lower out-of-pocket expenses reduce depression risk.36,37 Interestingly, family support showed no significant correlation with intrinsic capacity, reflecting the complex nature of Chinese family relationships where support effects may vary by baseline capacity—potentially beneficial for higher-capacity adults while possibly accelerating decline in lower-capacity individuals through excessive caregiving demands. 38
Among health-related factors, pain negatively impacted intrinsic capacity both in SEM and correlation analysis. This finding is consistent with literature demonstrating that pain manifestations correlated with diminished capacity in aging populations, as pain impairs physical functioning, disrupts sleep, and compromises cognitive domains.39,40 Handgrip strength demonstrated a significant positive effect, confirming its value as an accessible biomarker reflecting both musculoskeletal integrity and physiological reserve. Hospitalization history negatively affected intrinsic capacity through mechanisms including bed rest, physical inactivity, medication changes, and psychological stress, with research showing cognitive decline post-hospitalization even after controlling for illness severity. 41 Univariate analysis revealed that participants without multimorbidity demonstrated significantly better intrinsic capacity, suggesting disease management should be central to maintaining capacity in older adults. Unexpectedly, falls showed no significant correlation with intrinsic capacity, contradicting previous research linking falls to decreased physical performance and cognitive decline. 42 This inconsistency may stem from our assessment methodology, which captured only recent falls without considering their severity or long-term consequences.
Our study has several limitations. First, participants with college education or above constituted 24.9% of our sample, which exceeds the national average of 15.5% for higher education attainment. 43 This educational disparity may limit the generalizability of our findings to populations with lower educational levels. Second, our cross-sectional study prevents establishing causal relationships between identified factors and intrinsic capacity; longitudinal studies are needed to validate these associations and track how intrinsic capacity changes over time in response to these determinants. Third, while our SEM examined direct effects of sociodemographic, lifestyle, environmental, and health-related factors on intrinsic capacity, it did not fully address potential interactions among these factors, such as how lifestyle influences might vary depending on health status—an area warranting further investigation.
Conclusion
Our study employed a SEM based on the ICOPE framework to identify key determinants of intrinsic capacity among community-dwelling older adults in China. The SEM analysis revealed that dietary habits, handgrip strength, social participation, healthcare access, and physical exercise positively impact intrinsic capacity, while advanced age, pain intensity, and recent hospitalization negatively affect intrinsic capacity. Primary care providers should implement targeted screening and interventions especially for older adults of advanced age or with recent hospitalizations. This study supports integrated, multi-domain approaches within community settings, such as combining exercise programs with nutritional interventions. These evidence-based insights can inform policy development and resource allocation for community-based healthy aging initiatives that promote functional independence and reduce healthcare burden. Future public health programming should prioritize these modifiable factors to effectively support intrinsic capacity maintenance among aging populations.
Footnotes
Ethical Considerations
Ethical approval was obtained from the Xinxiang Medical University Ethics Committee (XYLL-20240279) and the Ethical Review Committee for Human Research, Mahidol University (MUPH2024-081).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This thesis was partially supported by the Faculty of Graduate Studies and Graduate Studies of Mahidol University Alumni Association.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.