
Abstract
Introduction:
Under the mandate of supporting European immunisation cooperation and strategies, the specific aim of this work was about focusing on vaccine communication in order to raise awareness, increase confidence and strengthen the practice for vaccination in Italy.
Methods:
The four-step Plan-Do-Check-Act cycle applied through a bundle of actions: (Plan) studying national vaccination scenarios and factors underlying vaccine hesitancy by developing a reference grid; (Do) creating a web platform-based toolbox with vaccine communication tools; (Check) engaging within national stakeholders within dedicated roundtables also associated to media trainings; (Act) co-developing, or co-selecting, tools to pilot amongst identified target communities.
Results:
In 2021, we analysed evidence on vaccine hesitancy determinants in scientific (86%) and grey (14%) literature by applying contextual, individual, and vaccine-specific categories. A total of 42 out of 204 vaccine communication tools collected and evaluated in early 2022 referred to Italy. In mid-2022, participatory dialogue and engagement with national stakeholders, media included, addressed vaccine communication improvements in different target populations. In late 2022, co-creation/selection of vaccine communication tools and their piloting focused on specific vaccinations and communities, such as the school setting for Italy.
Conclusions:
To address better vaccine communication outcomes, efforts on multistakeholder collaboration, training and advocacy are needed.
Keywords
Introduction
Immunisation is defined as a successful global health, development and investment story, saving millions of lives every year. Nowadays, despite vaccines are available to prevent more than 20 life-threatening diseases, far too many people around the world – including nearly 20 million infants each year – have insufficient access opportunity to vaccinate. Additionally, in some countries, progress has stalled or even reversed, although the Coronavirus disease (COVID-19) pandemic served as further occasion to highlight the power of vaccines to fight disease, save lives, and create a healthier, safer, and more prosperous future. The World Health Assembly endorsed a new global vision and strategy, the Immunization Agenda 2030 (IA2030), to address all the vaccine-related challenges over the next decade by envisioning a world where everyone, everywhere, at every age – no one left behind, in any situation or at any stage of life – fully benefits from vaccines for better health and well-being.1-3
When we come to the national levels, strengthening and improving vaccination programme implementation necessarily require some actions such as firstly developing data collection and analysis on vaccination components, then sustaining decision-making by consolidating and constantly updating available information on agreed indicators, benchmarked targets, methods and procedures, and delivering rapid and prompt reporting with relevant data. Monitoring and Evaluation (M&E) frameworks are quite complex because they usually aggregated into pre-, peri-, and post-vaccination phases, and include elements of vaccine procurement, transport, storage, staff training, communication, coverage, adverse effects, and identification of successes and failures. 4
Within the European Union (EU) Health Programme, under the mandate of increasing immunisation cooperation and vaccine outcomes in the EU, a specific focus was on studying existing vaccine communication tools in view of further supporting new strategies to raise awareness as well as empower and improve vaccination compliance in target population communities (eg, citizens, health professionals or other stakeholders), even with the aim to amplify visibility and role of the Coalition for Vaccination. 5
In order to achieve this vaccine communication objective aimed at extensive vaccination confidence and equitable uptake, a bundle of actions was developed: from understanding dynamics preventing access to vaccines up to strengthening stakeholder collaboration, through training and dissemination activities. A key action point is in fact the professional training to upskill healthcare practitioners to effectively tackle increasing complexities and uncertainties experienced in primary care in matter of promoting vaccination. We developed a two-fold approach: on the one hand, enhancing vaccine strategies which are recommended both at community level and within each country and, on the other hand, contributing to increase knowledge on vaccines and vaccinations especially among health professionals by better addressing information circulation in different target groups through a multistakeholder collaboration. In alignment to this participatory approach, indeed communication and training actions were mostly emphasised to raise vaccine awareness in specific population groups, by studying mechanisms most hindering vaccine access and, conversely, potential measures and solutions to overcome the identified barriers.
In showing how processes and workflows for effective vaccine-related strategies and interventions would be supposed to be delivered, we specifically describe the Italian case that highlights to what extent vaccination policies need to be based on integrated and coordinated communication initiatives. As noted, the process as a whole has necessarily to include the real engagement of all relevant stakeholders in the field, firstly acknowledging scientific evidence on effective actions to develop and tools to use in order to improve vaccinations in the different population groups. Focusing on the Italian case, the paper shows how the interdisciplinary “journey” for improved forms of communication on vaccinations is crucial for advancing practice in achieving increased vaccine coverage that represents both a major and challenging issue within primary care settings and public community health.
Materials and Methods
As largely used in public health, we adopted the four-step W. Edwards Deming’s model, Plan-Do-Check-Act (PDCA) cycle, because such framework draws the deliberate and defined process for quality improvement in public health as it is focused on activities that are responsive to community needs. It refers to a continuous and ongoing effort to achieve measurable advancements in the efficiency, effectiveness, performance, accountability, outcomes, and other indicators of quality services or processes that achieve increased and more equitable population health. 6
PDCA cycles provide, in fact, a clear structure for iterative testing of changes to improve quality of systems:
Plan – design the change or progress to be tested or implemented,
Do – carry out the test or change,
Check – engage in a lively understanding of the extent of change and its (chances of) success,
Act – plan the next change cycle or full implementation on a broader scale, continue to monitor the change and iterate as necessary by repeating the cycle.
Building on the four core principles underpinning the IA2030 strategy—finalised to maximise the extension of benefits from vaccines to everyone, everywhere— which consist of putting people in the centre, countries in charge of leadership, implementation through broad partnerships, and data-based enabling process, we applied the PDCA model along the study period, 2021 to 2023 (Figure 1).

Plan-Do-Check-Act cycle stages.
Plan (Stage 1) – Study Phase
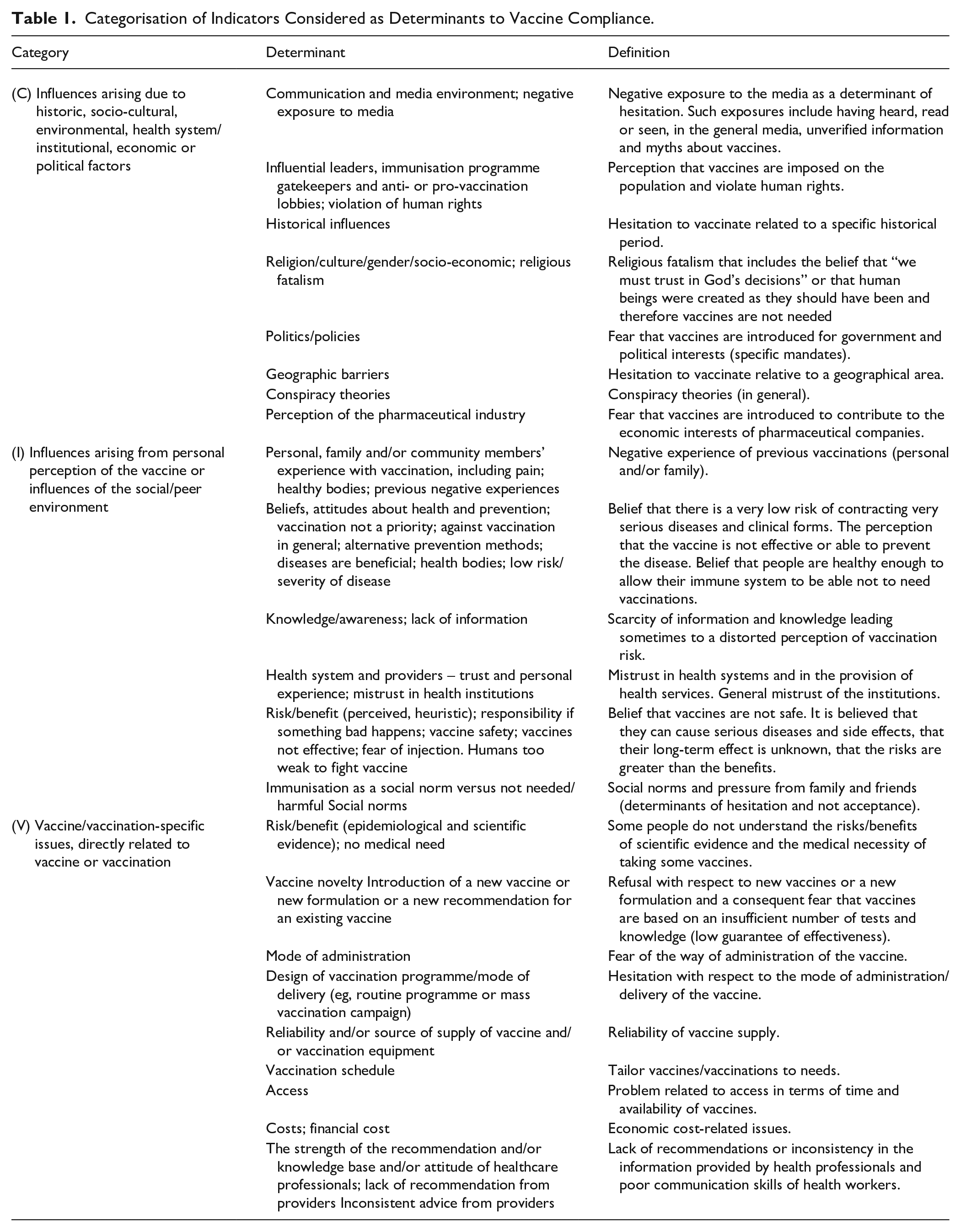
The very base was about developing an understanding of the national vaccination scenarios in four European countries (Italy, Greece, Latvia, and Romania), analysing vaccine attitudes and behaviours, and factors underlying low coverage, especially in underserved communities, in general as well as during health emergencies (eg, the COVID-19 pandemic). To this aim, we designed a prototype reference grid to fill in with literature data on the three macro categories associated to vaccine hesitancy, or confidence, which are contextual elements, individual aspects, and vaccine-specific issues merging what has been retrieved by a much-cited peer-reviewed article listing key vaccine hesitancy determinants 7 and prominent technical reports authored by the European Center for Disease Control and Prevention (ECDC).8,9 Table 1 shows how the indicators were subcategorised, respectively, as related to the context (C) – influences arising due to historic, socio-cultural, environmental, health system/institutional, economic or political factors; individual (I) – influences arising from personal perception of the vaccine or influences of the social/peer environment; vaccine/vaccination (V).
Categorisation of Indicators Considered as Determinants to Vaccine Compliance.
We extracted data from 43 sources using the following headings: lead author, publication year, source type (ie, article, abstract, book, report), language, country/ies included, aim, study information (ie, design, participants, data collection, analysis), and findings (ie, M&E tool/framework used, indicators included, lessons described).
Do (Stage 2) – Implenting Phase
Building on the reference grid, we gathered existing vaccine communication and community engagement tools, in English and country languages, to help increase vaccine uptake and informing a web platform-based toolbox that, in turn, can be gradually updated and enriched as other communication tools are newly developed. Beside descriptive items of the tools (eg, year, source, determinants covered or subject disease), other evaluation criteria were included. Firstly, scored levels for text readability were assessed by a specific literature search on readability scores and evaluation methods. An expert librarian developed and validated the search by querying the collection “Health Research Premium Collection” (ProQuest), which enables research simultaneously in a database of bibliographic records, including the following databases: Consumer Health Database, Health & Medical Collection, Healthcare Administration Database, Medline, Nursing & Allied Health Database, Psychology Database, Public Health Database. Out of 170 pertinent records extracted, about 60% mentioned the Flesch-Kincaid Reading Ease and the Flesch–Kincaid Grade Level. We found a free website (https://goodcalculators.com/flesch-kincaid-calculator/) that offers both formulae. Whether the tool could be transformed in a Word document, it was also possible to use a Microsoft Word’s processing program with a function to calculate readability statistics on textual inputs based on the two Flesch-Kincaid formulae indicated above. The three readability levels identified the following thresholds: 1 – low (<40%); 2 – average (41-70%); 3 – high (>71%). The second evaluation element concerned the graphic layout assessed as positive (≥12) or negative (≤11) from the total count of the single score ranging from 1-poor to 5-high assigned to: Readability (eg, size of characters); Appropriateness (efficacy of graphic choice); Quality (use of colours and image definition); Impact (arrangement of text and figures). Lastly, the complexity was assessed as 1 – simple, 2 – average, 3 – very complex (ie, demanding advanced prior knowledge).
Check (Stage 3) – Verification Phase
The third step encompassed engaging in an interaction with a multistakeholder panel by a dedicated national vaccination roundtable including a media training. The discussion revolved around the ways to improve vaccine uptake in different target groups, by involving the relevant stakeholders in the field such as national and regional health authorities, health professionals, researchers, civil society representatives and citizens’ associations.
Act (Stage 4) – Co-creating Phase
The fourth step, that actually according to a circular approach gives input to a new cycle, concerned co-developing (or even co-selecting) a tool and piloting it amongst the identified target communities to support efforts for vaccine uptake and equity improvement, under a longer sustainability perspective, and above all tailored to specific population groups, vaccines and national scenarios.
Results
Plan (Stage 1)
Figure 2 provides the PRISMA flow diagram of the results from reviewing both scientific and grey literature on national vaccination scenarios in four European countries (Italy, Greece, Latvia, and Romania). Overall, among the screened sources, the final amount of records included was 57: 49 out of 95 peer-reviewed items and eight non-peer reviewed reports out of 47.

PRISMA flow diagram.
The present paper considers the 34 out of 49 scientific studies which took place exclusively in Italy (29) or included Italian population samples within European-based initiatives (5) in the decade 2011 to 2021 (Table 2).10-43 The most studied vaccinations were against influenza (n = 13; 38%), HPV (n = 6; 18%), and COVID-19 (n = 4; 12%). Six studies addressed early childhood vaccines and only one examined vaccinations to health professionals. Four articles analysed all vaccines, on the contrary one focused on varicella and another on measles. With regard to the factors described, on the one hand a total of 15 studies (44%) addressed the determinants combined: three on triple category (contextual, individual, vaccine), whereas different distribution occurred for the double issue (n = 9/26% considered individual and vaccine-specific aspects, two scientific papers explored contextual and individual determinants, and one context- and vaccine-related patterns). On the other hand, among manuscripts concentrating only on one category, 14 (41%) reported findings on individual factors, three on elements related to the vaccine(s) under investigation and two to the context. The most covered topics concerned knowledge foundation, awareness and risk perception, attitudes and behaviours around vaccinations, with focus on barriers or enablers to uptake, according to the specific perspective of target population (eg, health professionals or parents on childhood vaccines).
Synthesised Literature Findings by Italian Studies.

Abbreviations: C, contextual vaccine determinants; EU, European studies; GPs, general practitioners; HPs, health professionals; I, individual vaccine determinants; ICT, Infection Control Team advocating for influenza vaccination among HPs; NR, not reported; V, vaccine-specific determinants; VPDs, vaccine preventable diseases.
Do (Stage 2)
From the 204 heterogeneous vaccine communication tools collected overall across the four countries or at international level, 42 related to Italy. Table 3 shows characteristics for the Italian tools which relate to the decade 2013 to 2022. The most part was issued by institutional actors such as the Ministry of Health (n = 28; 67%) and other two by a governmental body; six tools (14%) were released by the Italian Society of Hygiene, Preventive Medicine and Public Health, five (12%) by Paediatrics Association or Hospital, and one by several groups altogether. Differently from the scientific studies, vaccine communication tools addressed mostly single determinants: 18 tools (43%) vaccine-specific patterns, ten (24%) contextual factors, and nine (21%) individual-related elements. Combination of factors were addressed as follows: three tools individual and vaccine issues, one on context and vaccine, and another on context and individual perspective. These tools mainly targeted general population (67%) and in a certain measure specific groups such as parents, as vaccine preventable diseases (VPDs) were generically indicated or specific vaccinations recalled were measles, COVID-19, HPV, rubella. In more than half of cases (55%), the communication format was poster, other similar versions such as leaflet or booklet covered 21% of the tools, and multimedia material consisted of seven videos. The readability score was possible to apply to the half of tools retrieved: 13 got more than 75, 5 were assessed with medium points (>50), two by low values and one resulted with negative number.
Italian Vaccine Communication Tools.
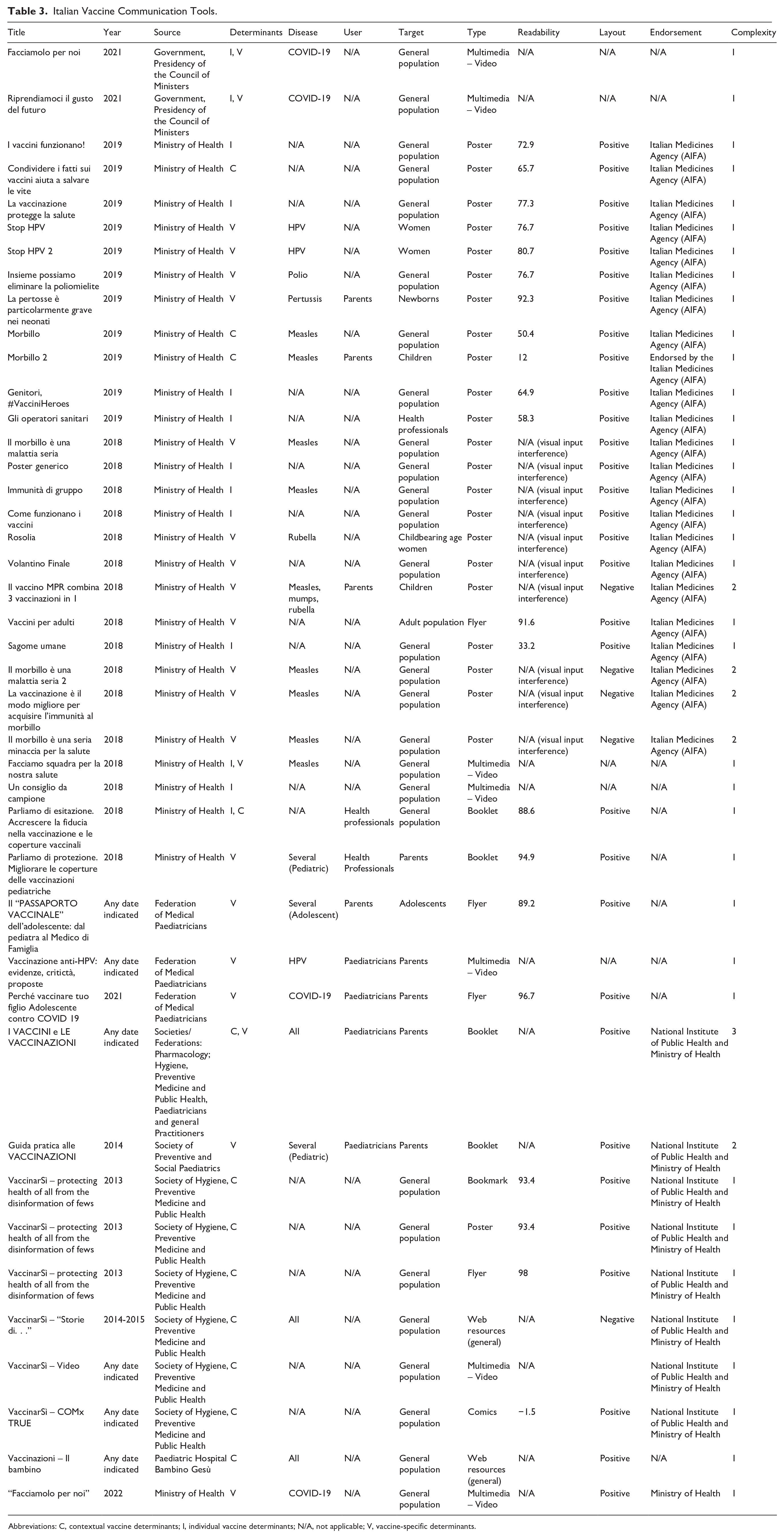
Abbreviations: C, contextual vaccine determinants; I, individual vaccine determinants; N/A, not applicable; V, vaccine-specific determinants.
Check (Stage 3)
A participatory dialogue and direct engagement with national stakeholders, media included, was developed to discuss communication tools for improving vaccine uptake in different populations, in particular vulnerable and underserved groups.
The Italian roundtable took place at the premises of the National Institute of Health, namely Istituto Superiore di Sanità (ISS), in Rome on June 13, 2022 and saw the participation of 11 reference persons representing eight stakeholder categories: institutional as Ministry of Health, Ministry of Education, and ISS Press Office; health professionals (General Practitioners, Nurses, and Pharmacists); Civil Society Organisations as Active Citizenship and School Principals. The Italian stakeholder roundtable particularly focused, in fact, on the role that schools can have in improving levels of awareness and compliance with vaccinations in the students’ community as well as in their families, broadening to a large part of the whole population. Based on the ISS platform for professional training, the gathered stakeholders agreed that it could be viable to build up a digital library/repository of validated materials on vaccinations that can be useful to teachers and students. Training courses can address these issues, providing teachers with communication competences, which are fundamental in the promotion of vaccinations among school-aged children and their families. ISS envisaged the school setting as appropriate context for action, even taking advantage from the long lasting alliances with both Ministries and health authorities (centrally) and the third sector (locally). Furthermore, the national roundtable was associated to a media training that in the case of Italy concerned the main figures about misconceptions related to journalistic approaches to vaccine communication. The focus of the training was on how to improve cooperation between experts and journalists, and how to effectively communicate through modern media reliable information on vaccination and health policies to protect the public from infectious diseases. Participants also discussed how to effectively create social campaigns and reach out to specific social groups. They also analysed the most common fake news about vaccination and together came up with methods to dispel harmful myths and lies about immunisation.
Act (Stage 4)
After the three previous phases (studying national scenarios, gathering vaccine toolboxes, engaging with relevant stakeholders in the field), co-creation and/or co-selection of tools on vaccine communication to pilot followed, both focusing on particular vaccinations and certain population groups, such as the school setting for the Italian node.
In Italy, in fact, vaccine-related issues are not specifically addressed in schools despite this setting is ideal to effectively reach out several target groups (students but also their families, teachers and other school professionals). In this framework, the scope of action was about raising vaccine awareness among secondary school-aged children (10-19 years old) in the Lazio Region, and related groups as indicated (eg, teachers and students’ families). After the national roundtable and the appropriate evaluation of stakeholders’ considerations, the association of school headmasters was engaged to further discuss and exchange ideas and perspectives. In order to better address contents to discuss in a face-to-face meeting, a rapid survey targeted teachers, students, and parents by administering three different web-based questionnaires. Topics investigated were: preferred information sources about vaccines and vaccinations; knowledge, attitudes and practices on indicated vaccines (diphtheria, tetanus, pertussis, poliomyelitis, hepatitis B, Haemophilus influenzae type b infection, pneumococcal disease, measles, mumps, rubella, varicella, meningococcal disease, influenza, herpes zoster, hepatitis A, COVID-19); school engagement and efforts in matter of VPDs; media voice and myths around vaccinations. The total respondents, n = 89, (respectively, 27 students, 28 teachers, and 34 parents confirmed that school can play an active role and serve as privileged context to provide not only vaccine information but also vaccination practice. Selected representatives of the target groups identified were invited in an innovative setting such as the Scientific Museum of ISS on December 12, 2022, to further elaborate on the survey results and figure out possible educational material to develop. Teachers and students were engaged in a lively discussion on health information literacy in general and in particular on vaccine communication tools, by soliciting reasoning about vaccines and vaccinations as relevant disease prevention and public health issue to further embed in the Italian schools. A recognised example as feasible implementation case was the promotion of HPV vaccination.
Discussion
The experience described in matter of pooling vaccine communication actions to promote vaccination in Italy according to the PDCA cycle allows several considerations, even in the light of the comparison with experiences from other countries, which this process and its variations44-46 resulted to be challenging to apply within real implementation programs, up to cases such as reported by Manyazewal et al 47 who included the use of the PDCA cycle in a continuous quality improvement intervention for a vaccination programme in Ethiopia or Aceituno et al 48 who used a logical framework to determine participant engagement in Bolivia.
The first scope of the specific focus on the PDCA framework applied to the Italian context was to highlight to what extent it is fundamental to run the four-stage cycle consistently in order to deliver effective and impactful vaccine communication. Furthermore, the particular matter of vaccine communication has to be necessarily included in the national vaccination strategies which, in turn, need to be considered as a whole. A study on communication implementation in the H1N1 pandemic influenza outbreak in Italy in 2009 found a lack of planning and a low value attached to the skills required to produce effective communications. As also in other two countries, there was a dearth of good quality audience research to inform the development of communications. Little thought had been given to the tone, targeting or channelling of messages. Instead, communications were characterised by a “one size fits all” and a “top down,” expert-led response. There was also little effort to evaluate the impact of communications, but where this was done, very low levels of public compliance and engagement with key behavioural messages were found. 49 Such low adherence to communication principles specifically applied to vaccine policies and strategies can be retrieved even in a recent assessment of the national coverage for different vaccinations in Italy in the last 25 years. The acting Ministers and Chief Medical Officers from 1999 to date analysed five consecutive National Vaccination Prevention Plans (1999/2000, 2005-2007, 2012-2014, 2017-2019, 2023-2025) and commented on the quite heterogeneous situation in Italy: whereas childhood vaccinations approached target levels, though regional differences, others such as for adolescents, the elderly, and vulnerable individuals consistently fell short of targets. This result is linked to the ambitious and well-planned vaccination policies in Italy over the past 25 years which successfully impacted, onto newborns immunisation, but conversely causes for failure to achieve goals for other groups have to be searched also among inconsistent implementation of the Regional Vaccination Prevention Plans. 50
Linking up to the concept expressed earlier, about the need to look at the vaccination chain as a whole that necessarily considers the vaccine communication lever, in Italy large population-based surveillance systems are in place to monitor continuously behavioural multirisk factors in adults and older individuals, and represent valuable data sources even to detect several vaccine-related aspects. This applied to vaccine flu compliance among health professionals, 51 disparities for rubella vaccination coverage among Italian versus migrant childbearing-age women, 52 associations between vaccination against influenza and health literacy level in regional subsamples 53 or, during the last pandemic, to understand the COVID vaccine confidence in the elderly. 54
In the last years, health literacy has been conceptualised as a social vaccine in the context of the COVID-19 pandemic but, when exploring the vaccine-specific health literacy, so called vaccine literacy, among the general population, some particular drivers characterise this subarea of the general health literacy. Both the theoretical and experimental scientific debate has been deepening and increasingly led to understand that general health literacy and its specific forms such as vaccine literacy only partially but not completely overlap. It means that highly health literate people may not show high vaccine literacy, and the two forms of literacy (general and vaccine-specific) tend to differ as per weight in predicting some health or health-related outcomes. Therefore, health- and vaccine-literacy need to be considered as partially interweaving knowledge, skills and competencies relating to vaccinology that deals with several issues including wide ranged disciplines, from biology and epidemiology up to human and social sciences. In turn, such complexity is associated to the vaccination rationale that is about individual and community health protection. Vaccines do represent, in fact, primary prevention tools on healthy people who are called to assumption of responsibility and decision on themselves or for others (e. g., parents to their children) and, as shown in this study predictors to vaccination uptake or acceptance may significantly differ from levers for other health behaviours. 55
It seems then fundamental that to appreciate the real progress in terms of vaccine communication, beside the implementation of a comprehensive and well-designed strategy such as the PDCA framework here presented, as also Others have suggested indicating ten actions to counteract vaccine hesitancy in Italy, 56 diverse systems or procedures for disease prevention and health promotion need to be considered according to a holistic approach. In the present study, some of the measures proposed by the Italian Society of Hygiene, Preventive Medicine, and Public Health encompassing the role of vaccine communication are retrievable, namely in establishing multidisciplinary working groups, recognising local and national best practices, focusing on professional training and promoting both collaborations between scientific societies and knowledge from behavioural sciences.
Limitations
The exercise about pooling vaccine communication actions to promote vaccination in Italy shows the ideal cycle to put in place according to the PDCA model. However, to commute theory to practice, each step is approximated at the better solution but some limitations apply such as, firstly, the different scale through the PDCA cycle is developed. Where it was adopted the national perspective, part of the evidence retrieved referred to subnational levels, that is, regional or local (eg, single hospital). Additionally, to indicate how effective the health communication is, readability of not all tools can be assessed by using the Flesch-Kincaid formulae.
Conclusions
Through a broad perspective to look at vaccine communication, it emerged how vaccine hesitant or confident behaviours in the different population groups are associated to determinants which apply to contextual, individual, and vaccine-specific issues. Thus, the elaboration process of vaccine communication tools need to be designed and developed building on available and updated evidence, as well as used and assessed in a coordinated, integrated and collaborative multistakeholder and intersectoral scenario. Vaccine literacy improvement passes through sustainable and synergic life course interventions, including continuous training to health professionals. Physicians and other healthcare workers have the huge potential to be a mighty force in fighting infodemics and reversing hesitancy toward vaccination, but to gain health it is necessary that communities continuously collaborate, partner, and support each other, to do what one sector could never do as effectively on its own. Such complex reasoning appears even more relevant when the discussion is about vaccines and vaccination policies.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251342097 – Supplemental material for Pooled Vaccine Communication Actions to Promote Vaccination in the European Union: The Case of Italy
Supplemental material, sj-docx-1-jpc-10.1177_21501319251342097 for Pooled Vaccine Communication Actions to Promote Vaccination in the European Union: The Case of Italy by Valentina Possenti, Roberto Croci, Roberta Terlizzi, Annina Nobile, Luca Fucili, Marco Mirra, Stefano Lucattini, Massimiliano Di Gregorio, Anna Maria Giammarioli, Scilla Pizzarelli, Francesco Corea, Antonio Mistretta, Paola De Castro and Raffaella Bucciardini in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We truly wish to thank EuroHealthNet staff who coordinated the EU-funded project “Improving IMMunisation cooperation in the European UNION” in the persons of Caroline Costongs, Alison Maassen, Alba Godfrey, David Hargitt as well as all participating Partners.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research refers to some actions developed within “Improving IMMunisation cooperation in the European UNION” that has been receiving funds by the European Union’s 3rd Health Programme, 2014-2020, under grant agreement number 101018210.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Please, contact the corresponding author for specific information requests on data presented.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.