
Abstract
Introduction:
Disparities in access to tobacco cessation support and resources remain significant issues among community members with low socioeconomic status (SES). Community health workers (CHWs) can connect with community members and have flexibility in delivering treatments to underserved populations. The Community Health Allies Nicotine Guidance Education (C.H.A.N.G.E.) project, designed for CHWs, aimed to address the disparities by implementing a tailored tobacco cessation training program. The current study examined the C.H.A.N.G.E. program’s preliminary effectiveness on CHW knowledge gain.
Methods:
Data were collected from CHWs in Chicago, IL who participated in the training program between October 2022 and December 2023, and CHWs completed a tobacco cessation knowledge questionnaire pre-training, post-training, and at 1- and 6-month follow-up. A paired samples t-test was conducted to assess changes in CHWs’ pre-post knowledge change. Descriptive analyses were also explored to examine the type of knowledge that was retained and whether that differed by the client population that CHWs served.
Results:
CHWs (N = 72) were mostly women (68%) who worked in their current role for an average of 2.34 years (SD = 1.54). The mean age of participants in the study was 38.06 years (SD = 13.09). Baseline knowledge was low (M = 3.75 [1.18] out of 10) but significantly increased post-training (M = 6.64 [1.13]; P < .001). There was no difference in change of tobacco cessation knowledge scores for groups based on client population served.
Conclusion:
The C.H.A.N.G.E. training effectively improved CHWs’ tobacco cessation knowledge. However, knowledge changes had no differences based on client types of CHWs. This study highlighted the importance of continuous adaptation and evaluation of training programs to fit the needs of CHWs and their clients in underserved, community-based settings.
Introduction
Tobacco use remains among the most imminent threats to worldwide public health. 1 In the United States, those with lower socioeconomic status (SES) have a disproportionately greater prevalence of tobacco use (24%) compared to the national average (15%). 2 Evidence indicates that tobacco cessation interventions outside hospital settings are necessary and feasible for community organizations to adopt to support adults with low SES.3,4 Implementing and disseminating tobacco cessation treatment and tools for interventions that fit the nature of community healthcare could benefit community members who want to quit smoking with more resources accessible to them.5,6
Community health workers (CHWs) are non-physician healthcare providers who work directly with community members outside hospital settings, focusing on healthcare education and health resources navigation services, including doing brief tobacco cessation interventions. 7 However, existing tobacco cessation trainings for CHWs in the U.S. have been found unsuitable due to high cost, long training time, and relevance issues for their low SES clients. 8 CHWs lacked sufficient knowledge of tobacco use and cessation, despite their clients’ significant need for such interventions.9-11 The Community Health Allies Nicotine Guidance Education (C.H.A.N.G.E.) project adapted the World Health Organization Toolkit for Delivering the 5A’s and 5R’s Brief Tobacco Interventions in Primary Care©12-14 to equip CHWs with tailored skills and knowledge for effective tobacco cessation support, addressing a critical gap in training suitability and knowledge retention among these non-physician professionals. The training lectures and discussions provided CHWs with background in the nicotine addiction, information on tobacco cessation treatment and available services, and skill-building for motivational interviewing specifically for tobacco cessation. 15
In community health settings, CHWs often found that clients with complex health conditions were smoking. To effectively provide smoke cessation counseling to clients with cardiovascular problems, chronic pain, and mental health concerns, CHWs need to possess extra and specialized knowledge on the health condition as well as how tobacco use is related to these health issues. The previous study conducted by the C.H.A.N.G.E. team found that CHWs primarily see clients with specific health conditions predominantly related to tobacco use. A needs assessment survey revealed that 72.4% of CHWs served clients with chronic illnesses. In addition, 40.3% of CHWs reported working with patients who had experienced homelessness, 56.9% saw clients with mental health disorders, and 40.3% assisted people with substance use disorders. 8 One benefit of tobacco cessation training is it builds providers’ knowledge and confidence in treating high-risk individuals and reminds researchers and practitioners to pay attention to clients with special needs. 16 Therefore, CHW-focused tobacco cessation training needs to include information and knowledge of tobacco use and tobacco cessation for individuals with special conditions. Thus, the knowledge learning trajectory may be different for CHWs that serve different types of clients because general training may not cover all tobacco-related knowledge for all kinds of co-occuring health conditions. However, only a little research explores the knowledge trajectories of CHWs, what specific knowledge CHWs retain, and what they still need to learn.
To understand how an adapted training for CHWs affected knowledge change, we examined the pilot data from the C.H.A.N.G.E. project. We hypothesized that CHWs’ knowledge would increase post-training. Additionally, we examined which knowledge participants gained most effectively based on the types of clients they served. Comparing knowledge change scores for different client types and analyzing the correct rates for each knowledge test question across the pre-training and post-training surveys will be important for us to have more insights into the effectiveness of the training and the specific knowledge areas where CHWs showed the greatest retention.
Methods
Participants
We recruited a convenience sample of CHWs from community-based organizations (CBOs) and a CHW degree program at a community college in Chicago, IL, a large urban city in the U.S., to participate in the C.H.A.N.G.E. training in person. Each training session had approximately 10 to 20 participants. Survey data were collected from 111 CHWs during trainings held from October 2022 to December 2023. During the training period, 111 participants completed the pre-training survey, and 103 participants completed the post-training survey, with some CHWs leaving the training early. We conducted a complete case analysis of 72 participants who fully completed all knowledge test questions in both pre-training and post-training surveys. Follow-up surveys were collected online after 1 month and 6 months from 15 participants; because only 6 participants had complete data for pre-training, post-training, 1- and 6-month follow-up, these results will not be discussed.
Procedure
A quasi-experiment, pre-post design was employed to examine the C.H.A.N.G.E. training’s effect on CHW knowledge. Each training session, lasting about 150 min, started with participants filling out the pre-training survey asking for basic information about themselves and their clients, tobacco cessation counseling practices, as well as the tobacco cessation knowledge questionnaire. Each participant received a handbook with lecture materials and other training materials created by the C.H.A.N.G.E team. At the end of the session, participants were asked to complete the post-training survey asking about training receptivity and the same tobacco knowledge questionnaire again. A $50 gift card was given to each participant when they finished the training session and both questionnaires. The follow-up surveys assessed tobacco knowledge, as well as training implementation.
The training was led by 2 instructors, who were doctoral and master’s level health psychologists. The training session contained 3 parts: a lecture on tobacco cessation and the nicotine addiction, training on motivational interviewing, and a role-play activity. The lecture included topics such as facts about tobacco use among underserved communities, the difficulty of quitting smoking for community members, and treatment options available. Motivational interviewing (M.I.) training provided information on brief counseling techniques and “good” versus “bad” examples of doing M.I. with clients. 13 Lastly, the role-play allowed participants to take turns playing CHWs and clients, practicing skills they learned in the training sessions. In addition, hypothetical low SES client cases were discussed throughout the training session and included in each aspect of training.
Measures and Analysis
Knowledge among CHWs was evaluated using an investigator-initiated 10-item tobacco knowledge questionnaire, which covered subjects like smoking prevalence, tobacco use disparities, weight gain following cessation, symptoms of nicotine withdrawal, and evidence-based tobacco cessation treatments. The questions were adapted from a previous questionnaire developed by the study team 9 and covered information that was presented in the training, which was adapted from the WHO Toolkit. The 10 knowledge test questions were within 3 categories: Tobacco Use (Qs 1, 2, and 3), Tobacco Cessation (Qs 5, 6, 9, and 10), and Tobacco Myths (Qs 4, 7, and 8). See Supplemental Appendix for the complete knowledge test questionnaire.
The knowledge test score of each participant was calculated as the respondent’s total number of correct answers (ranging from 0 to 10). If the answer option to a multiple-choice question was correctly selected, the participant received a score of 1 on that knowledge test question. If all answers were correctly selected in the checkbox (choose all that apply) questions, they received a score of 1, no partial correct score was given if some, but not all correct answer were chosen. We added each question’s score together to get a final score for the knowledge test. The analyses incorporated knowledge ratings as a continuous variable.
In the pre-training questionnaire, we asked participants what type of client/patient population they see in their current position. Participants were asked to indicate whether or not they see each type of client, and which group they primarily serve among “Individuals with mental health disorders,” “Individuals with substance use disorders,” “Individuals with chronic illnesses,” “Individuals experiencing homelessness,” “Individuals in the criminal justice system,” “Individuals experiencing domestic violence,” and “other.” We coded “Yes” and “Yes, this is the group I primarily serve” together as participants served this group of clients. For analysis, we conducted a paired t test on pre-training and post-training knowledge test scores on 72 participants who had a complete knowledge test data (no missing questions).
Results
CHWs were mostly women (68%) who worked in their current role for an average of 2.34 years (SD = 1.54). The mean age of participants in the study was 38.06 years (SD = 13.09). Most of CHWs (75%) spent less than 15 min or 15 to 30 min time with their client during 1 visit in their job. Pre-training knowledge score (the baseline condition) was low, but significantly increased post-training (t = −19.11, P < .001).
We calculated the percentage of participants correctly answering each question for pre-training and post-training conditions (see Figures 1 and 2). There were 8 (out of 10) questions that the post-training correct rate was higher than the pre-training correct rate. Correct rate of question 9 (“Which of the following are principles of motivational interviewing?”), a multiple answer question, was the same (25.0%) in pre- and post-training. Question number 4 (“Smoking relieves mental health symptoms (such as anxiety, depression, etc.)”), which was a true or false question, had a higher pre-training correct rate (44.4%) than the post-training correct rate (30.6%).

Correct rate of each question with comparison between pre- and post-training.
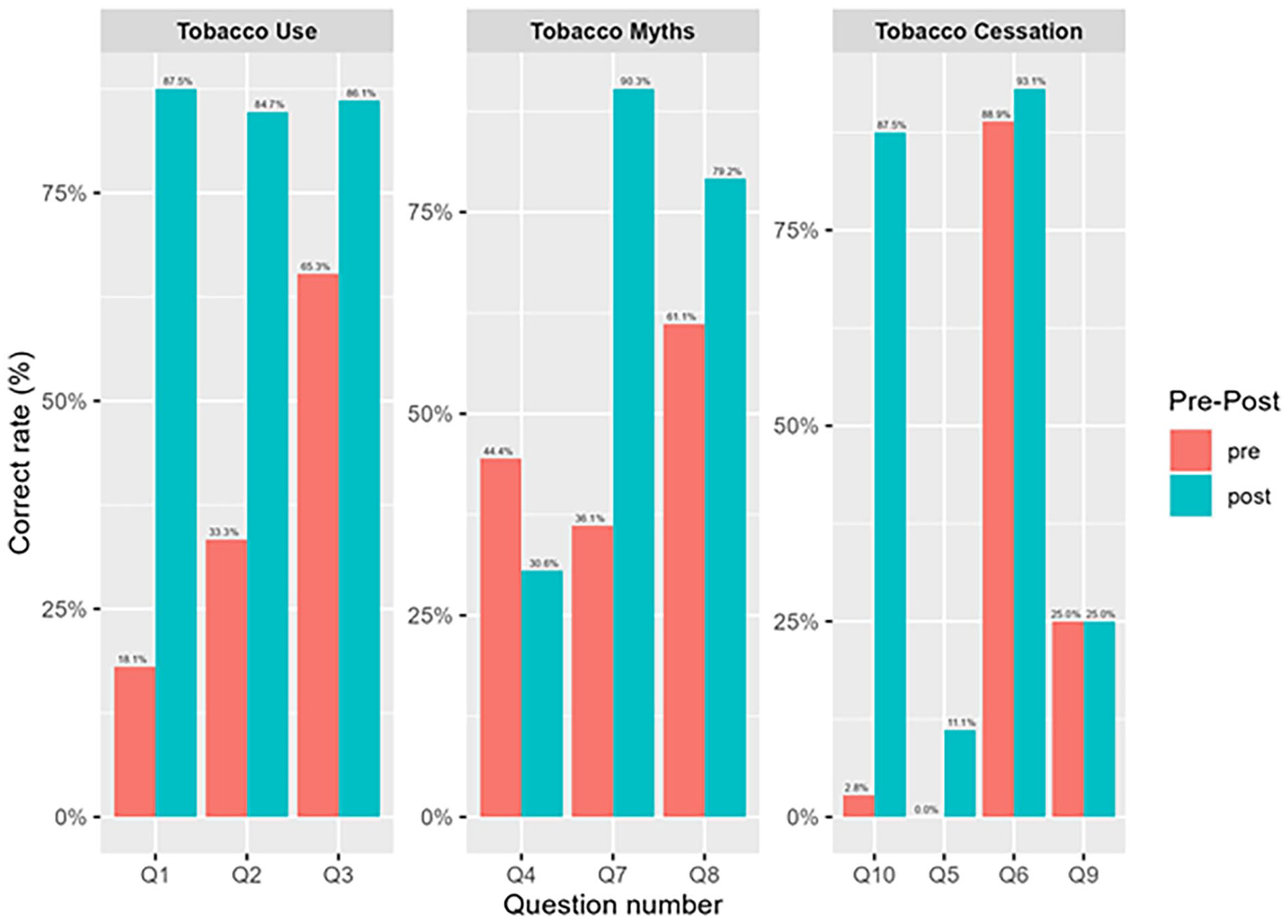
Correct rate of each question indicating knowledge group.
In addition, a change score was calculated as each participant’s post-training knowledge test score minus their pre-training knowledge test score. We grouped the change score by the client types that participants reported in the pre-training survey (e.g., Individuals with mental health disorders, Individuals with substance use disorders, Individuals with chronic illnesses, Individuals experiencing homelessness, Individuals in the criminal justice system, and Individuals experiencing domestic violence). Figure 3 shows the mean change score within each client type. The mean change scores had a mean of 3.09 (SD = 0.11).
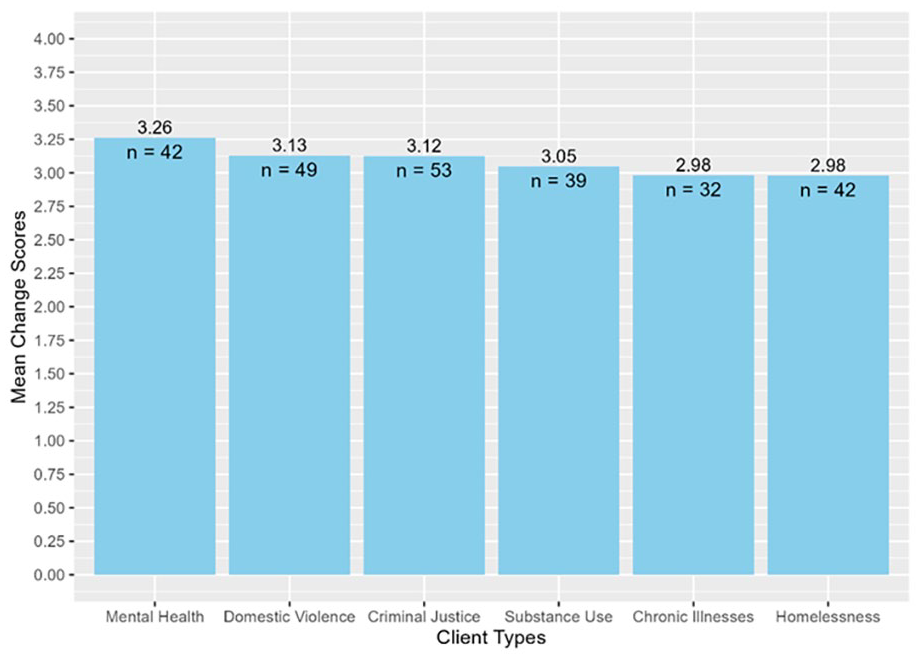
Mean change score for CHWs grouped by types of clients they serve.
Discussion
In our sample of community health workers, baseline knowledge of tobacco use, tobacco cessation, and tobacco myths was low before taking the training session. However, the knowledge score of the CHW participants improved significantly after training, which suggested that our training materials and design helped them acquire knowledge on topics like tobacco use, interventions, and myths about tobacco. Thus, our efforts to adapt traditional tobacco cessation models to fit the CHW model better returned optimistic results. Adapting a brief intervention focusing on skill-building in motivational interviewing was a promising strategy to modify a tobacco cessation training that will be relevant for CHWs and the low SES communities they serve.
Furthermore, we conducted a preliminary repeated measure analysis of variance (ANOVA) on 6 participants who had complete data on pre-training, post-training, 1-month follow-up, and 6-month follow-up. Results showed a significant difference in mean knowledge test scores at different follow up assessments. Although results should be interpreted with caution, they suggested that while the training effectively increased knowledge immediately post-training, this increase was maintained only up to 1 month before returning to baseline levels by the 6-month follow-up. Although this ANOVA had a small sample size, it gives a preview of the trend of knowledge retention among CHWs. As additional data are collected, future research will explore knowledge retention at 6 months using an intent-to-treat analysis and all available data to understand when knowledge is lost over time. A systematic review of CHW training program literature found that researchers across the globe needed to address the sustainability of ongoing training for CHWs. 17 Assessing knowledge retention in promoting public health interventions is critical for researchers and practitioners to understand the effectiveness of the training materials. 18
The current study also examined what types of information CHWs learned through the training. In general, tobacco use, interventions, and tobacco myth knowledge increased after training. Checkbox (choose all that apply) questions had a low correct rate (e.g., Question 9) even after the training (e.g., “Which of the following are principles of motivational interviewing? Please check all that apply.”) because it is natural that participants need to remember all the information about the topic to answer correctly. Although this method of assessing knowledge (i.e., checkbox questions) may be useful to thoroughly assess learning, more time may need to be spent discussing this crucial tobacco-related information during training to help CHWs’ understanding. Notably, Question 4, “Smoking relieves mental health symptoms (such as anxiety, depression, etc.),” had a meager correct rate (29.1%) in post-training, even lower than the correct rate in the pre-training test. This was expected, as this was a “trick” question designed by C.H.A.N.G.E. team. The trainer discussed how nicotine can bring a relaxing sensation by immediately relieving acute nicotine withdrawal symptoms, which makes people believe that stress and anxiety are reduced. However, research showed smoking cannot relieve any stress in the long term. 19 Tobacco use and stress were important for CHWs to bring up with clients when doing interventions, so the C.H.A.N.G.E. team designed a question to test if participants clearly understood the nuanced relationship between stress and smoking. The participants’ confusion may be due to the structure of the question. Nonetheless, this suggests that this is an important topic that trainers should spend more time clarifying with CHWs.
Additionally, descriptive analysis showed that the types of clients CHWs see had no impact on their knowledge retention within the current sample. Because we cannot create mutually exclusive groups of CHWs with client types, we needed more information on whether seeing clients with special needs has an impact on knowledge retention. Future studies should assess this information in ways to better group CHWs by the types of clients they see during work. However, we could still see that participants who see clients with mental health conditions had the greatest change score on the knowledge test compared to other client-type groups. Surprisingly, participants who serve people with chronic illnesses had a relatively low change score. CHWs may already have specific knowledge about smoking before training, so the change score does not reflect their knowledge retention. Community members may have limited knowledge of using medication or nicotine replacement therapy (i.e., nicotine patch and nicotine gum) to help the cessation process. People with specific health conditions (i.e., substance use disorder or chronic illness) may have concerns about using these cessation options. Thus, CHWs must guide them in learning and understanding what interventions can help them most effectively. Thus, tobacco cessation training must contain relevant knowledge and intervention skills that could help them respond to the different needs of community members.
The findings of the current study align with previous research on tobacco cessation training for CHWs. One other study specifically adapted a tobacco education program designed for CHWs. 20 The study found that a CHW-specific curriculum in tobacco cessation was highly acceptable among CHWs as it was informative, relevant, and interactive. Both studies emphasized the importance of teaching CHWs relevant knowledge and skills to deliver tobacco cessation interventions for communities. While the Lautner et al. (2019) 20 study focused more on the curriculum development process and implementation feasibility without extended follow-up assessments, the C.H.A.N.G.E. study employed a quasi-experimental pre-post test design to evaluate knowledge retention quantitatively. These findings suggest that while tobacco cessation training for CHWs is effective in improving knowledge, future programs should incorporate sustained engagement strategies such as follow-ups and reviews and ongoing mentorship to maintain long-term retention. Additionally, a combination of culturally tailored materials and evidence-based intervention models may enhance the impact and scalability of CHW training programs across diverse communities
The current study has some general limitations. Because the study participants primarily lived in specific neighborhoods or communities in the Chicago area, our conclusions should not be construed as applying to all CHWs. Instead, they should be understood as representing the needs and practices of those providing services in Chicago. Moreover, these data do not include CHWs that serve non-English speaking clients. However, Chicago communities have very diverse low SES populations and high rates of smoking, so these findings are still relevant to tobacco cessation and community health worker practice, especially among those living in and serving large, urban cities. 21 Another limitation is that the sample size of follow-up sessions was small and needed a matched group of participants, so we could not conduct analyses to examine knowledge trajectories over time. Missing data or unusable survey answers were also limitation of the current study. This was due to some managers of CHW programs opting not to complete the entire training, as well as participants skipping questions on the survey or making mistakes in answering. We decided to use complete case analysis to better examine knowledge change.
Conclusion
In conclusion, the current study demonstrated the necessity of tailored tobacco cessation training for CHWs that fits both their strengths and needs while supporting their role in providing smoking treatment to populations with low socioeconomic status. Our findings from the C.H.A.N.G.E. project revealed a significant increase in tobacco use and cessation knowledge among trained CHWs. Knowledge outcomes did not change significantly across CHWs who served different client types. Future research should prioritize practical, CHW-relevant knowledge dissemination and feedback from CHWs to refine trainings further. Our program also explored which type of knowledge was gained. These results can help guide community organizations in developing their own training programs for their CHWs that is tailored to the specific needs of CHWs. Future research should also focus on how CHW-specific tobacco cessation training is associated with actual tobacco use outcomes among community members.
Supplemental Material
sj-pdf-1-jpc-10.1177_21501319251341977 – Supplemental material for Examining the Preliminary Effectiveness on Knowledge of a Tobacco Cessation Facilitator Training for Community Health Workers
Supplemental material, sj-pdf-1-jpc-10.1177_21501319251341977 for Examining the Preliminary Effectiveness on Knowledge of a Tobacco Cessation Facilitator Training for Community Health Workers by Tianqu Lu, Anna Veluz-Wilkins, Andres Mauricio Garcia Sierra, Dedeepya Konuthula and Marcia Tan in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We would like to thank all of the community health workers who participated in this research. We would also like to thank Shariwa Oke, MA, Clarissa Huard, MPH, and Lian Nicholson, MA for their support in developing the visual materials for the curriculum.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the American Cancer Society (ACS_IRG [IRG-16-222-56]), the University of Chicago Comprehensive Cancer Center Support Grant (P30 CA14599), and the V Foundation for Cancer Research (V2021-006).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.