
Abstract
Objectives:
The COVID-19 pandemic presented significant challenges, particularly the psychological impact of prolonged preventive measures. This study aimed to explore the longitudinal relationships among adherence, anti-pandemic fatigue, and depression, focusing on how these dynamics evolved.
Methods:
A prospective longitudinal survey was conducted among 627 adults in Hong Kong during the pandemic across 3 waves. Repeated measures ANOVA, cross-lagged path modeling, and mediation model were employed to assess temporal relationships among adherence, anti-pandemic fatigue, and depression.
Results:
Adherence at T3 significantly predicted T4’s anti-pandemic fatigue (B = 0.196, SE = 0.055) and depression (B = 1.690, SE = 0.247), and anti-pandemic fatigue significantly predicted T4’s depression (B = 0.684, SE = 0.260). These effects diminished at later waves, reflecting psychological relief as restrictions eased. Notably, adherence was found to increase anti-pandemic fatigue, which in turn exacerbated depressive symptoms.
Conclusion:
While relationships varied over the 3 time points, the longitudinal design has clarified the causal inference. The study highlights the mental toll of prolonged restrictions and emphasizes the importance of designing integrative strategies that support adherence while addressing fatigue and depression. These findings offer actionable insights for primary care and community health programs in managing future public health emergencies.
Introduction
The COVID-19 pandemic, instigated by the novel coronavirus SARS-CoV-2, emerged in December 2019 and swiftly turned from a regional epidemic to a world-wide health emergency. 1 Since then, policies related to COVID-19 prevention have become one of the most important global issues. In the early phases of pandemic outbreaks, in the absence of potent medications, strategies such as minimizing person-to-person contact were deemed the most effective for halting the rapid rise in the number of infections. 2 Several research suggested the benefits of adherence to preventive measures, highlighting its critical role in addressing the pandmemic.3-5 However, the prolonged duration of the COVID-19 pandemic makes sustained adherence poses risks, particularly to mental health.6,7 Therefore, this study aims at examining the impact of adherence to preventive measures on psychological well-being.
As reported in prior study, adherence to preventive measures is associated with greater daily hassles which may further trigger anti-pandemic fatigue. 8 However, in most cases, the relationship between adherence and fatigue was found to be negative, with low adherence often considered a result of heightened fatigue.9,10 The lack of longitudinal studies makes it challenging to draw causal conclusions about whether adherence causes fatigue. Conceptually, greater adherence reflects a higher level of engagement with the intended practices, which aligns with the underlying cause of fatigue—sustained periods of cognitively demanding activity. 11 As the COVID-19 pandemic transitioned into its middle and later stages, many studies highlighted the detrimental effects of anti-pandemic fatigue on the population.8-10,12,13 Anti-pandemic fatigue is characterized as a form of mental fatigue that specifically arises from prolonged engagement in preventive measures, leading to a gradual decline in motivation to comply with recommended protective behaviors. 8 Fatigue is recognized as a symptom of a wide range of mental and physical illnesses; however, it can also have significant adverse effects on healthy individuals, such as work disabilities or even cognitive impairments.14-16
Notably, individuals experiencing fatigue often show a higher prevalence of depression. 17 During COVID-19, depression has emerged as a prominent psychological hurdle,18,19 with concerns ranging from fear of the virus20,21 to the daily hassles brought about by the pandemic as potential triggers for depressive symptoms. 21 Considering the long-time adherence to strict measure is related to the daily hassles, it may also further contribute to the increased level of depression. 8 Moreover, a few cross-sectional studies identified negative associations between pandemic-related fatigue and mental health outcomes (eg, depression).9,22,23 Building on these arguments, we further propose a mediation model in which adherence at the earliest time point influences depression at the final time point through anti-pandemic fatigue at the intermediate time point.
Previous studies examining psychological impacts during pandemics have largely employed cross-sectional designs to examine the immediate psychological effects of preventive measures.8,9,24 While these studies provided valuable snapshots, the temporal dynamics were failed to be present. While these studies provided valuable snapshots, they could not capture temporal dynamics. Several key questions remain unanswered: whether anti-pandemic fatigue leads to low adherence or whether higher adherence brings greater fatigue,8-10 and whether fatigue serves as a precursor to or a symptom of depression. 25 In other words, the causal directions among adherence, anti-pandemic fatigue, and depression remain ambiguous. Therefore, longitudinal studies are essential for understanding temporal ordering of effects, capturing dynamic processes over time, and providing stronger evidence for causal mechanisms. Clarifying these causal relationships in pandemic settings is crucial for designing evidence-based interventions that effectively reduce psychological harm.
Research Context
Strict preventive measures, such as travel restrictions, contact tracing, and extensive testing, were widely implemented during the early stages of the pandemic. However, concerns about the adverse impacts of prolonged restrictions led many countries, 18 including US and UK, to gradually relax these measures and adopt strategies to coexist with the virus. 26 However, Hong Kong experienced a prolonged phase of domestic containment, placing significant pressure on its citizens. This context provides a valuable setting for examining the potential consequences of sustained adherence with preventive measures.
Data and Methods
Research Design
This panel study targeted Hong Kong residents aged 18 years and older who could communicate in Cantonese or Mandarin. To ensure representative sampling while protecting participant privacy, we employed a random-digit dialing approach. Phone numbers were selected randomly using a multistage process. A local Hong Kong directory provided phone numbers, both landline and mobile. Prefixes were randomly chosen and used as “seeds” to create numbers using the “last digit ±1 or 2” method. After removing duplicates, 6000 numbers were randomized. Initial phone contact was used to screen for eligibility based on our inclusion criteria (age ≥18 years, Hong Kong residency, and Cantonese/Mandarin language ability). Only participants meeting all criteria were invited to proceed with the full interview. For households with multiple eligible members, participants were selected using the last birthday method to ensure random selection.
All interviews were conducted via telephone using structured questionnaires, with strict privacy protocols in place. Personal identifiers were separated from survey responses, and data were anonymized before analysis. Verbal informed consent was obtained and documented from all participants before data collection began.
The data used for the analysis were part of the 5-wave longitudinal data collection endeavor that took place at different time points: T1 baseline (December 19, 2020 to January 6, 2021; n = 1255), T2 follow-up (June 11, 2021 to July 21, 2021; n = 1003), T3 follow-up (December 21, 2021 to January 21, 2022; n = 803), T4 follow-up (March 22, 2022 to April 18, 2022; n = 703), and T5 follow-up (June 29, 2022 to July 27, 2022; n = 627). Data from the T3, T4, and T5 follow-ups were used for the present longitudinal analysis. During T3 data collection, Hong Kong faced the onset of its fifth COVID-19 wave, leading to swift anti-pandemic measures. By T4, Hong Kong was at the peak of this wave, with stringent measures in place for months. By T5, infections had reduced, and restrictions were relaxed.
Measurements
Depression was measured using the Chinese version of the 9-item Patient Health Questionnaire-9 (PHQ-9) with a 4-point Likert-type scale ranging from 0 (“not at all”) to 3 (“nearly every day”). 27 The higher the total scores, the greater the depressive symptoms. The internal consistency of the scale was assessed using Cronbach’s alpha, resulting in a satisfactory level of reliability (α = .914-.962).
Anti-pandemic fatigue was evaluated using 8 items developed by the Fatigue Assessment Scale.8,16 All items were rated on a 5-point Likert-type scale ranging from 1 (“never”) to 5 (“always”). The Cronbach’s alpha for the scale ranged from 0.933 to 0.957 in the current study, indicating high reliability. This scale includes items that assess various emotions, such as worry, concentration, and energy, experienced during the COVID-19 pandemic. A higher mean score for all items indicates a higher level of anti-pandemic fatigue.
Adherence to preventive measures was assessed using a 6-item and 5-point Likert-type scale, ranging from 1 (“limited times”) to 5 (“almost all the time”). An acceptable internal consistency of this scale was reported in this study (α = .529-.732). The questions were developed by the researchers and aligned with the COVID-19 prevention measures advocated by the Center for Health Protection, a governmental body responsible for managing the pandemic in Hong Kong. The scale items covered various preventive actions, including proper mask usage, handwashing practices, and voluntary participation in virus testing. A higher mean score for all items, indicated a higher level of adherence to preventive measures.
Data Analysis
Repeated measures analysis of variance (ANOVA) was conducted to analyze the differences in mean scores of 3 variables at 3 time points, and a post hoc test was subsequently performed to reveal specific differences using a paired t-test. A cross-lagged path model was employed to assess the influence of a variable measured at 1 time point on another measured at a subsequent time point, which provided insights into the temporal dynamics and potential causal effects between the variables of interest. The cross-lagged path model includes 2 components: (1) the autoregressive component, which represents the stability of each variable over time, and (2) the cross-lagged component, which represents causal relationships between the variables. Demographic variables (ie, gender, age group, educational attainment, and economic activity status) were included as the confounding variables. The suggested criteria for indicating adequate model fit are as follows: a Comparative Fit Index greater than 0.90, a Tucker-Lewis Index greater than 0.90, a Root Mean Square Error of Approximation less than 0.10, and a Standardized Root Mean Square Residual less than 0.05.28,29 Mediation analysis was performed using the PROCESS macro, 30 with age, gender, education attainments, and economic activity status as the covariates. Ordinary least squares (OLS) regression was used to estimate the direct, indirect, and total effects. The significance of the indirect effect was assessed using 5000 bootstrapped samples to compute bias-corrected 95% confidence intervals. Data analysis was conducted using SPSS version 26.0 and R 4.1.0 with the “Lavaan” package version 0.6-15.
Results
Demographics of Participants and Key Variables
The demographic characteristics of the participants and the descriptive results of the 3 variables are presented in Table 1.
Demographic Characteristics of Participants and Descriptive Results of Variables (n = 627).

Results of the Repeated Measures ANOVA
The post hoc test results highlighted the variations observed in the repeated measures ANOVA outcomes (see Figures 1–3). Depression and anti-pandemic fatigue levels remained consistent at the first 2 time points (T3 and T4) and decreased at the final point (T5). However, adherence levels were significantly higher at T4 than at T3 and T5.
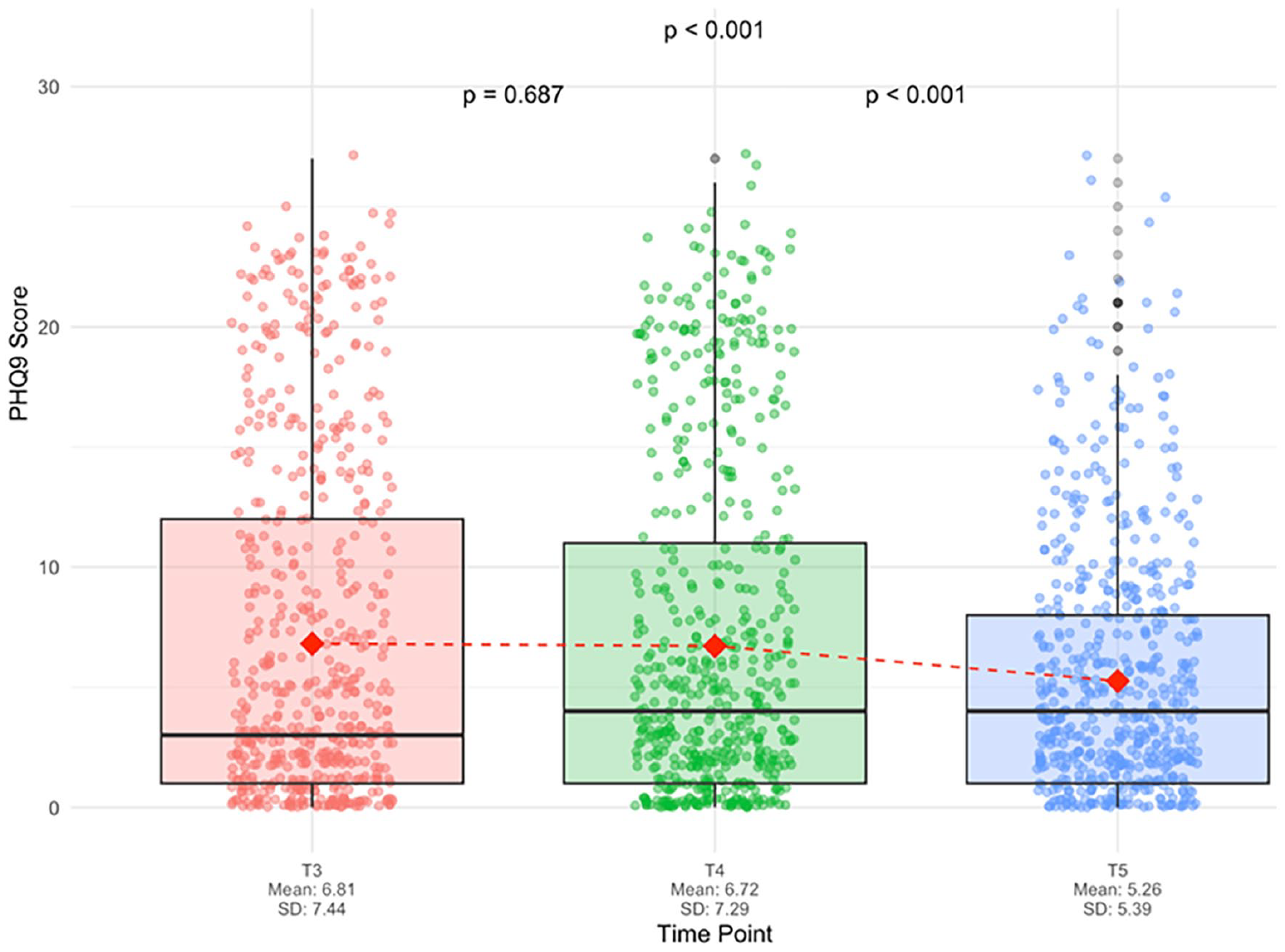
Depression scores progression (n = 627).

Anti-fatigue scores progression (n = 627).

Adherence scores progression (n = 627).
Results of Cross-Lagged Path Model
Based on the indicated criteria, the model presented acceptable fit. Regarding depression, the model accounted for 76.0% at T4 and 50.5% at T5. For anti-pandemic fatigue, the model accounted for 39.9% at T4 and 14.4% at T5. Table 2 presents the autoregressive and cross-lagged effects of the models.
Cross-lagged and Autoregressive Effects.

P < .05.**P < .01.***P < .001.
The autoregressive paths in the model reveal the significant effects of each variable on its subsequent waves. Significant and positive correlations were observed between depression at T3 and T4, and between depression at T4 and T5, indicating a consistent and stable pattern of depression over time. Similar patterns of high stability were observed for anti-pandemic fatigue and adherence to preventive measures.
The significant autoregressive pathways indicated that elevated scores in all 3 variables at T3 were associated with higher scores at T4 and similarly at T4 to T5, suggesting that the position of the participants on these variables remained consistent over the examined time periods.
Adherence at T3 positively predicted anti-pandemic fatigue and depression at T4 (anti-pandemic fatigue, B = 0.196, P < .001; depression, B = 1.690, P < .001), whereas the associations became insignificant in the latter 2 waves. Meanwhile, anti-pandemic fatigue at T3 positively predicted depression at T4 (B = 0.684, P < .01), and anti-pandemic fatigue at T4 was not significantly associated with depression at T5.
Results of Mediation Model
Mediation analysis was conducted to examine whether anti-pandemic fatigue at T4 mediates the relationship between adherence at T3 and depression at T5. The indirect effect of adherence on depression through fatigue was significant, despite a non-significant total effect and direct effect (see Table 3). Specifically, higher adherence to preventive measures (T3) contributed to anti-pandemic fatigue (T4; β = .194, P < .001), and higher anti-pandemic fatigue (T4) further predicted increased depression (T5; β = .408, P < .001).
Results of Mediation Analysis.

P < .05.
Discussion
Previous research has frequently highlighted the increased prevalence of psychological issues, particularly depression, during the COVID-19 outbreak,31,32 due to the unknown and highly contagious disease33-35 or restrictive measures during COVID-19.36-38 These studies highlight the connection between the impact of prevention measures on daily life and the development of negative psychological experiences. However, many studies overlooked the potential adverse effects of adherence to preventive measures, which may exacerbate daily challenges. Furthermore, the lack of longitudinal research limited presentation of a causal relationship between prevention measures and psychological outcomes. To address these gaps, this study employed 3 waves of longitudinal survey data to examine how individual adherence to preventive measures influenced the experience of anti-pandemic fatigue and depressive symptoms over time during a pandemic.
According to findings from the repeated measures ANOVA, which indicates the observed pattern over time in the population, levels of depression and anti-pandemic fatigue remained stable during the first 2 time points (T3: December 21, 2021 to January 21, 2022; T4: March 22, 2022 to April 18, 2022), followed by a significant decrease at T5 (June 29, 2022 to July 27, 2022). Meanwhile, adherence levels were comparable at T3 and T5 but significantly increased at T4. The surge in adherence during the T4 phase, coinciding with the peak of the pandemic around March 2022, was driven primarily by the imposition of stringent preventive measures by the government, including the shutdown of entertainment venues. The increase in adherence during this period was attributed more to compulsory compliance than to personal choices. Regarding the trends of anti-epidemic fatigue and depression, it is interesting to note that there was no significant increase from T3 to T4. Given that T3 marked the beginning of the fifth wave of the pandemic for Hong Kong and that citizen had already endured 2 years of pandemic conditions, it is plausible that the levels of anti-pandemic fatigue and depression were already elevated by phase T3. This might explain why no further deterioration was observed at T4 (March 22, 2022 to April 18, 2022), as individuals might have already reached a relatively high level of mental strain due to long-term exposure to stressful conditions.39,40 At the T5 stage (June 29, 2022 to July 27, 2022), both depression and fatigue levels decreased as the spread of the virus began to be under control in Hong Kong.
Adherence to preventive measures at T3 positively predicted anti-pandemic fatigue levels at T4. The relationships between adherence to preventive measures and anti-pandemic fatigue reported in previous cross-sectional studies are inconsistent.8,9 Conceptually, the adverse effects linked to high adherence may take time to manifest, which could account for similar findings not being supported by cross-sectional research. 8 The present study substantiated a clear cause-and-effect relationship, showing that higher adherence in the earlier phase leads to increased fatigue in the later stages.
We also observed a lagged effect of adherence at T3 on depression at T4. Considering the stringent social restrictions during the period from T3 to T4, adherence to such measures usually led to a higher level of social isolation, as people were discouraged from going out. 41 In addition to social isolation, the hassles caused by adherence to restrictive measures was also a predictor of depressive symptoms. 37 Moreover, high adherence during the early stages of the outbreak was associated with greater concern about the virus, which was a major cause of depression during COVID-19.20,42 As the severity of the pandemic escalated in Hong Kong between the T3 and T4 periods, concerns about the virus were anticipated to persist and continue to influence depressive symptoms. Previous research has suggested a potential link between adherence to preventive measures and mental health issues. 43 However, these studies were unable to effectively demonstrate the negative impact of adherence, primarily due to the lack of sufficient longitudinal data—a limitation addressed by the current study.
However, no evidence was found to support a relationship between adherence at T4 and anti-pandemic fatigue or depression at T5. These results may be attributed to the specific pandemic context prevalent during data collection. As discussed above, the period from T3 to T4 was a phase of escalating severity during the pandemic, with a sharp increase in daily confirmed cases and an extended duration of restrictive measures. However, from T4 to T5, the preventive measures were loosened. The changes in the pandemic situation likely made the lagged effects of adherence at T4 on fatigue and depression at T5 insignificant.
The observation that anti-pandemic fatigue at stages T3 to T4 predicted subsequent levels of depression aligns with the findings of previous studies. 9 Some researchers contend that fatigue contributes to psychological dysfunction under stressful conditions, whereas stress is often identified as the primary contributor to depression.44,45 Thus, fatigue can be considered a predictive factor for depression. However, some scholars have argued that fatigue and depression share conceptual similarities, 46 often resulting in autocorrelation when examined through cross-sectional research. The findings of this study offer nuanced evidence that anti-pandemic fatigue could serve as a predictor of depression during a pandemic. Due to the lack of significant differences between anti-pandemic fatigue and depression at T5, a similar rationale was considered. As the pandemic came under better control and perceived severity diminished, the mental strain related to COVID-19 eased, likely resulting in the absence of a predictive relationship between fatigue and depression.
Notably, a significant mediation pathway spanning 3 time points was identified, indicating that adherence to preventive measures contributes to anti-pandemic fatigue, which, in turn, predicts depressive symptoms. This finding suggests that adherence may not have a direct long-term effect on depressive symptoms but could contribute to their development indirectly by increasing anti-pandemic fatigue. The significant indirect effect through anti-pandemic fatigue, coupled with non-significant total and direct effects, suggests competitive mediation in the relationship between adherence and depressive symptoms. This pattern indicates that while adherence influences depression through increased fatigue, there may be opposing unmeasured mechanisms or pathways that suppress the overall relationship, warranting further investigation to identify these additional mediating factors.
The present study has offered evidence for examining the predictive relationships among adherence, fatigue, and depression as the COVID-19 wave transitions from its initial emergence through its peak and decline. While predictive relationships varied across time points due to changing pandemic contexts, our findings highlight how prolonged restrictive measures can impact mental health, with improvements noted when restrictions were eased. As the emergence of future infectious diseases is anticipated to occur periodically, 47 these findings offer crucial insights for public health strategies. The study demonstrates that while adherence to preventive measures is essential during health emergencies, prolonged implementation may contribute to psychological burden through increased anti-pandemic fatigue and subsequent depression. This suggests the need for more balanced public health approaches that protect both physical and mental well-being.
First, authorities should consider implementing flexible intervention strategies that maintain necessary preventive measures while monitoring and addressing psychological impacts. This could involve integrating mental health surveillance into public health systems and strengthening community-based psychological support programs. Second, communication strategies should focus on framing preventive measures positively, emphasizing personal agency and community benefit, while providing clear timelines to reduce uncertainty. These insights are particularly relevant for high-density urban environments like Hong Kong, where strict measures may be necessary during public health emergencies. Future emergency preparedness plans are suggested to incorporate these findings to develop integrated approaches that effectively balance public health measures with their potential psychological impact. This research transcends a basic analysis of COVID-19, casting light on expansive strategies for managing recurrent public health challenges, including chronic disease management and other health crises affecting specific populations.
Limitations and Future Research Directions
While this study provides valuable insights into the mental health implications of COVID-19 prevention efforts, several limitations should be noted. First, while demographic variables were controlled, certain potential confounders such as pre-existing mental health conditions and socioeconomic status were not included in our analysis. Second, our reliance on self-reported measures, while common in pandemic research, may be subject to social desirability and recall bias. Third, although our 3-wave design with 6-month intervals captured meaningful changes over a 12-month period, longer-term psychological effects might extend beyond this timeframe.
These limitations suggest several directions for future research. First, future studies should consider incorporating additional variables such as pre-existing mental health conditions, income levels, and social support networks to better account for potential influences on the depression trajectory. Second, when feasible, researchers should consider complementing self-report measures with objective data (eg, digital tracking of specific behaviors) to enhance validity of research. Third, studies with extended follow-up periods and more frequent measurement points could better capture the long-term psychological impacts of prolonged preventive measures.