
Abstract
Objective:
The Wrightington, Wigan, and Leigh NHS Teaching Hospitals Foundation Trust (WWL) developed a novel virtual ward (VW) service that integrated with community and primary care, supported healthcare throughout a patient’s journey, and had a clinical workflow that could step-up or step-down care as needed. We described their VW and evaluated clinical outcomes, adherence, safety, and patient satisfaction.
Methods:
Retrospective, single-center study of patients admitted to the WWL VW service from January 14, 2022 to January 31, 2024. Clinical data collected by WWL in their database for patients admitted to the VW, were matched to data captured automatically by the Current Health (CH) platform linked to the CH remote monitoring kits assigned to patients on the VW. The CH kits enabled the VW care at WWL and included a wearable device for continuous vital signs monitoring, a blood pressure cuff, and tablet. Evaluation metrics included clinical scope, clinical outcomes, adherence, safety, and patient satisfaction.
Results:
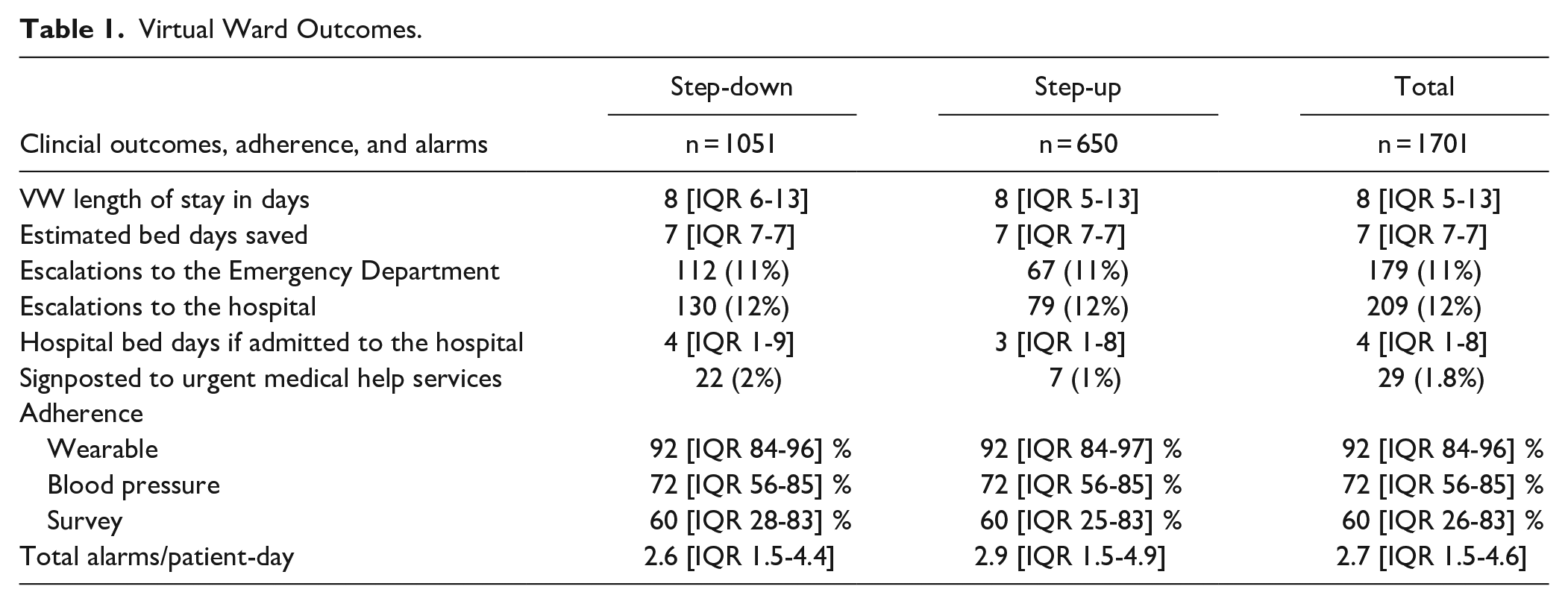
There were 1835 admissions and a 93% match rate between the clinical and CH databases. About 38% of referrals were step-up (31% ambulatory care and 7% primary care) and 62% of referrals were step-down (100% inpatients). Most specialty referrals were from thoracic and acute medicine (77%). The median length of stay on the VW was 8 days [IQR 5-13], 209 (12%) admissions were escalated to the hospital, 179 (11%) escalated to the emergency department out of hours, and 29 (2%) signposted to urgent medical services. Adherence to the wearable device was 92%. There were 38 minor safety incidents (typically hypersensitivity reactions or administrative errors) and 17 expected deaths. About 94% of admissions rated the VW experience as “excellent” or “good.” Results were similar between step-up and step-down referrals.
Conclusion:
We have shown the VW service yielded acceptable clinical outcomes, was safe with no serious adverse events or negative impact on mortality rate. Patient adherence to the technology and satisfaction with the VW service were high. The VW service was innovative in its acceptance of a broad range of patients, expanding services beyond respiratory medicine, and in developing a step-up pathway, preventing some patients from ever taking up an acute bed in the hospital.
Keywords
Introduction
Globally we are experiencing demographic shifts toward older populations, 1 along with a rise in chronic diseases2,3 and multimorbidity.4 -6 Hospitals in the UK, like the US, have seen a rise in older, multimorbid patients often experiencing prolonged hospital stays.7 -9 These delays have a downstream effect on hospital bed occupancy and overcrowding in acute emergency care areas. National Health Service (NHS) virtual wards (VW), similar to US Hospital at Home (HaH), help expand capacity by allowing inpatients to be cared for outside the brick-and-mortar hospital.
The promise of VWs and HaH lies in their ability to deliver safe and effective healthcare for patients at home, reducing burden on brick-and-mortar institutions, supporting care provision closer to home, and maintaining or increasing patient satisfaction. VWs allow patients to receive hospital-grade care in the comfort of their own homes, 10 linking acute hospital care with community-based healthcare. VWs can integrate with primary care by supporting chronic disease management, enhancing care continuity, and reducing unnecessary hospitalizations.
The National Health Service (NHS) in the UK has extended funding for VWs for 2025 and 2026, following a successful evaluation of 22 000 VW admissions in South-East England.11,12 In the US, the Acute Hospital at Home Care Waiver, created by the Centers for Medicare & Medicaid Services to cope with the COVID-19 pandemic, 13 has allowed VWs to expand, along with improved technology. 14 Continued funding, however, depends on further expansion, and evaluation of this care model both in the UK and overseas.
VW services described in the literature have typically focused on COVID-19, frailty, and respiratory care as primary use cases driving VWs forward.15 -17 These often used “step-down” pathways, moving patients in a single direction from an acute bed in a hospital to a VW. 18 There are limited publications describing VW care models that include step-up pathways in the literature. These tended to be small, focused on single use cases, but show positive results.19 -21 Step-up pathways could fundamentally change healthcare by diverting patients that would otherwise occupy a hospital bed, to receiving the care they need at home. For the right patient, this could mean a reduced risk of complications, 22 more movement, 23 and increased comfort 24 through monitoring or recovery.
Wrightington, Wigan, and Leigh Teaching Hospitals NHS Foundation Trust (WWL) developed a VW service that integrates with primary and community care to support patients across the care continuum with both “step-up” and “step-down” pathways and associated referral sources with very few exclusion criteria (Supplemental 1). Every admission was assessed on its merits based on clinical need and clinician assessment. Referral sources for “step-up” care included Advanced Care Practitioner, Emergency Department (ED) physician, General Practitioner (GP) and other community clinicians (cardiac or respiratory nurse, matron, React team GP). The Community React Team is a responsive service dealing with urgent issues, usually within 2 h, to reduce hospital attendance and admissions. The team can receive referrals from other services and provide interventions including intravenous antibiotics. 25 The numbers 111 and 119 also provide medical help and advice for urgent but not life-threatening situations. The Community React Team, 111, and 119 will be referred to as “urgent medical help services” in this paper. Referral sources for “step-down” care included discharging consultants, ward staff, and VW Band 7 Coordinator on an acute site.
An example of a patient on a “step-up” pathway would be one referred directly into a VW by their GP, without ever having to leave their home. It would also be a patient admitted to the VW from the ED before they take up a hospital bed. In this paper, we refer to step-up and step-down pathways in specific ways, meaning to, and from the VW. The step-down pathway is when a patient is moved from an acute bed in a hospital to a VW. The step-up pathway is diverting a patient before they require a hospital bed.
Step-up patients came from their homes, communities, care facilities, or GP surgeries, unlike step-down patients that came to the VW from an acute bed in a hospital. Admission to VW included remote monitoring, individualized care plans, education around equipment and clinical team contact, and when to contact emergency medical services (ED) out of hours to promote autonomy and shared care responsibility (Supplemental 1).
Remote Patient Monitoring Platform Enabling the Virtual Ward
The VW was enabled with the Current Health (CH) platform, which included a clinical dashboard and alerting system for healthcare providers (HCPs). The patients received a secure home hub that passively transmitted data from monitoring devices. Devices included a continuous remote vital signs monitor worn on the upper arm, a tablet for collecting survey data (eg, symptom surveys) and undertaking daily video calls and consultations, a blood pressure cuff, scale, pulse oximeter, and/or spirometer. Patients and HCPs communicated via the tablet.
The wearable vital signs device measured pulse and respiratory rates, oxygen saturation, skin temperature, and step count. The home hub transmitted these data to the cloud by broadband or free roaming cellular network (4G); patients did not require home internet. Data appeared on the clinical dashboard in near real-time and aggregated into 15-min intervals. When patients were not near their home hub, data were stored for up to 10 h and backfilled when device was within range. Customized alerting thresholds were set by the WWL clinical team in consultation with the CH staff. CH platform configuration included options to tailor alerts to each program and combine parameters to increase specificity, for example, increased pulse rate AND decreased oxygen saturation, set to specific thresholds. When a patient’s vital signs breached these thresholds, the clinician received an alert through the clinical dashboard and responded according based on an established escalation protocol. Patients were called for clinical review if required by VW clinician, in working hours.
Objective
To demonstrate that the VW with step-up and step-down care is safe, effective, and well-liked by patients using 2 years of real-world data.
We evaluated the clinical scope, clinical outcomes, adherence, safety, and patient satisfaction of a novel NHS VW model that expanded its service through integration with community and primary care and compared the clinical outcomes between “step-up” and “step-down” pathways.
Methods
Retrospective, single-center study of patients admitted to the WWL NHS Foundation Trust VW service from January 14, 2022 to January 31, 2024 and had not requested their data be removed.
Population
Patients within the WWL catchment area were referred to the VW by an HCP (described in the Introduction Section and Supplemental 1). There were minimal inclusion and exclusion criteria. Patients 18 years or older had to consent to VW admission, be able and willing to have daily video calls and use the CH monitoring technology, and could not have an implantable cardioverter-defibrillator or allergy to metals within the wearable that would have prevented the use of the wearable device.
Patients were discharged through individual assessment rather than set criteria. When HCPs responsible for patients believed they no longer needed the ongoing care and monitoring, patients were discharged from the VW service (Supplemental 1).
Wrightington, Wigan, and Leigh Data
Data were collected by WWL staff from multiple sources during patient admission to the VW to evaluate clinical outcomes, safety, and patient satisfaction. Clinical outcomes and descriptive data were collected by the WWL VW team and inputted into their own database. Clinical data included VW length of stay (LOS), estimated hospital bed days saved, number of escalations to the ED, number of escalations to hospital admission, hospital LOS if admitted, and number of times the patient was signposted to urgent medical help during the VW stay. The estimated hospital bed days saved as direct result of virtual care was based on the subjective experience of clinical teams. Descriptive data included patient comorbidities (eg, diabetes, hypertension, coronary heart disease, chronic kidney disease, and any other long-term condition), referring specialty, referral pathway, and patient demographics, such as age on referral and gender.
The NHS used Datix, a web-based system, for safety incident reporting and risk management. This web-service, used across the NHS as a risk management/significant incident reporting tool, was used to identify any significant patient related incidents with regards to VW service during the specialty evaluation window. Safety metrics included accidents, complaints, serious adverse outcomes, and death. Datix entries about staffing issues during periods of sickness or administrative issues were excluded. Deaths were also identified from the hospital database.
Current Health Data
THE CH data generated by the platform included adherence metrics to the wearable device, all peripheral kit components (eg, blood pressure cuff), alarming data (eg, when patients’ vital signs breached preset thresholds), and patient experience survey response data.
Patient experience was captured in 3 surveys delivered via the remote monitoring tablet. Surveys included the Telehealth Usability Questionnaire (TUQ) Ease of Use subdomain of 6 questions, 26 the WWL Patient Experience Survey, and the Friends and Family Test (FFT). 27 The TUQ response used a 7-point Likert scale from “Strongly Agree” to “Strongly Disagree” and was averaged over the 6 questions. The Patient Experience Survey consisted of 19 questions developed by WWL staff with categorical (eg, excellent to poor; very easy to very difficult) and open text responses. We report on 5 of these questions: how patients rated the VW process, the overall VW care received, how easy they found the CH equipment to use, the main benefits of being cared for at home, and on improvements that could be made to the VW experience. The Friends and Family Test was a 1-question survey: “On a scale of zero to ten, how likely are you to recommend the Current Health kit if a family member or friend had a similar health condition.” All patient experience surveys are reported at the admissions level, meaning a patient admitted more than once, may have submitted survey data more than once.
Database Matching
The WWL clinical dataset (containing clinical outcomes and descriptive data) and the CH dataset (containing adherence and patient experience survey data) were matched by patient ID and admission date; repeat admissions were included and unmatched data were excluded, except for safety and expected deaths data. Safety incidents and number of deaths were reported for the entirety of the WWL VW admissions. Some data could not be matched between datasets because of data entry errors in identifiers.
Data Analysis
Variables were summarized using descriptive statistics per admission. For patients admitted more than once, each admission is included in the dataset independently from each other. We report mean and standard deviation for normally distributed variables and median and interquartile range for non-normally distributed variables. We report percentages for binary or categorical variables. There were a small number of missing values in the clinical data set, and we excluded these in our reporting. The surveys were not mandatory and there were many missing surveys for the patient experience results.
Adherence was calculated as tasks or wear time completed versus prescribed. All adherence metrics were percentages with 100% representing complete adherence. Alarms from the CH platform to WWL VW staff were totaled and divided by the number of days the patient was admitted onto the VW (eg, the LOS) for alarms per patient-day. Average daily census was calculated using the sum of inpatient days on the VW each month, divided by the days in the month from 14 January 2022 to 31 January 2023. Safety data were in open text format and summarized in words. Clinical outcomes, remote monitoring adherence, and alarms per day were reported for the whole sample and stratified by referral pathway (step-up vs step-down).
We used the SQUIRE reporting guidelines for the improvement of healthcare. 28 The data collection related to this work was part of a service evaluation and was not submitted for NHS Research Ethics Committee review. 29 NHS service evaluations use aggregate, non-identifiable data to assess the performance of the service and are considered exempt from ethics review as it is not considered research by the Health Research Authority. Specifically, participants are not randomized, there is no protocol demanding a change in treatment or patient care from accepted standards, and the findings are not considered generalizable. 29 Patients are entitled to the removal of their data from analysis.
Results
The WWL clinical dataset included 1835 admissions to the VW during the evaluation window; 50 patients requested their data be excluded. Of the 1835 WWL VW admissions, we had a 93% match rate to CH admissions data. A total of 134 admissions could not be matched to CH data, leaving 1701 admissions successfully matched to the CH database. There were 38% of referrals from step-up pathways (ambulatory care = 31%, primary care = 7%) and 62% from the step-down pathway (100% inpatients). Most specialty referrals were from thoracic and acute medicine (77%), and the remainder from cardiology, general surgery, endocrinology, gastroenterology, stroke, and geriatric medicine.
Admissions over time by referral pathway (step-up or step-down care) are shown in Figure 1 reflecting a growth in VW admissions, and particularly those for the step-up pathway. Average daily census by month is shown in Figure 2 reflecting growth in the average number of patients cared for each day on the VW. Of the 1701 admissions, the large majority were single admissions (n = 1524 or 90%). However, there were some repeat admissions: 155 patients (9%) had a second admission to the VW, 19 patients (1%) had a third admission to the VW, and 3 patients had 4 admissions.

Number of admissions to the virtual ward per month by referral source.

Average Daily Census on the virtual ward.
Admissions were 54% female. Most admissions were 65 years or older (64%) with an overall mean age of 67 (16 SD) years ranging from 16 to 98 years old (Figure 3). Six patients, aged 16 or 17 years, were admitted to the VW based on clinical need, though the overall inclusion criteria for the VW was age 18.

Age at admission to the virtual ward.
Reported comorbidities for admissions were diabetes (20%), hypertension (34%), coronary heart disease (2%), chronic kidney disease (8%), and other long-term conditions (80%). Only 14% of admissions had no comorbid conditions, 43% had at least 1, and the remaining 43% had more than 1.
Clinical outcomes, adherence metrics, and alarms can be found reported in Table 1 by referral pathway (step-down or step-up) and for the total sample.
Virtual Ward Outcomes.
There were 38 incidents during the 2-year evaluation period. These incidents were related to VW patients, systems, and processes. Some of the patient factors included hypersensitivity reactions to the wearable device resulting in minor irritation, laboratory issues with blood test results going to the GP rather than to the VW staff, and a patient using their own blood pressure cuff rather than the provided cuff that transmitted blood pressure readings to the clinician-facing dashboard, resulting in absent blood pressure readings. An example of a process issue was a discharge medication not being documented in a discharge letter. There was one out-of-hospital cardiac arrest and on full review of the case, no omissions of care were found with regards to the VW. Of 1835 admissions in the VW there were 17 expected deaths in the cohort (0.9%).
Like the overall VW sample, 91% to 92% of responses to patient experience surveys were from unique admissions. However, patients admitted more than once had the opportunity to submit survey data more than once; the remaining 8% to 9% were from repeaters to the VW. Response rates for surveys were between 35% and 56% of the total admissions sample (Table 2). Patients reported positive experiences in the VW via the 3 surveys (Table 2). The Ease of Use survey showed high levels of agreement that the kit was easy to use (Supplemental 2). About 77% of responses to the Friends and Family Test were between 8 and 10, indicating high satisfaction with the VW service provided by WWL.
Patient Experience.

Patient Experience score is the percentage of responses rated as “excellent” or “good” (eg, care received from the VW).
Friends and Family Test score is a mean value of responses from 0 to 10 with 10 being most likely to recommend the Current Health kit.
Ease of use score is a mean of the Likert-scale responses per patient from 1 = strongly disagree to 7 = strongly agree. A score of 7 indicates that patients strongly agree with statements about the Current Health kit being easy to use.
In the WWL Patient Experience survey, the VW experience (94%), the care received from the VW (98%), and the CH kit and wearable (95%) were rated as “excellent” or “good.” CH kits were rated as “easy” or “very easy” to use in 93% of survey responses, which aligned with findings from the Ease of Use survey results. The main benefits as reported by patients were “being cared for in their own home” and “how good it was to be in their own homes knowing they were safe” because they were being monitored. Many patients mentioned what comfort it was to be able to get good sleep, have control over their food and downtime, be free from hospital-acquired illness, and to know their care at home left a bed open for someone that needed it more than them.
Being with family, using my own bathroom, my food and getting my own drinks. Getting more rest and knowing there was someone in the background if I needed help, plus it’s freeing up a bed at the hospital.
Female, 72 years old
Home environment definatly [sic] aids recovery, less stressful in regards to in hospital having to continuously ask staff for everything which is not fair on staff as they are all so busy.
Male, 61 years old
Patients were also asked how their VW care could be improved and whether they found anything difficult. Many patients responded that there was nothing that needed to be improved. Some patients felt that it could be lonely, were worried about their safety if something happened when nobody was nearby, and they would have liked more help with the equipment.
Just anxiety over any symptoms and that you may become unwell on your own without help around.
Female, 39 years old
I find it ok, but I do also like being in the care of nurses or doctors in the ward too. When I was at the hospital the other day I found it comfortable and staff were very helpful. I didn’t get long periods of being left alone considering the workload they have.
Female, 67 years old
Discussion
Providing care at home through WWL’s novel VW model is safe and effective, even for complex patients that are high acuity and have comorbidities. WWL developed their VW within integrated care services using multidisciplinary community rapid response teams per the guidance of the British Geriatric Society. 30 Furthermore, they created a VW with enhanced clinical scope by improving accessibility and inclusivity. They expanded and scaled the VW to more than the traditional use cases of respiratory and frailty patients. It meant that 38% of the VW patients that would otherwise have occupied a bed in a hospital were diverted to the VW and of those, 7% never had to leave their home.
Patient satisfaction scores suggest the technology was easy to use and the VW service was well liked by patients and aligned with person-centered care. Survey response rates were between 35% and 56%, and likely those patients that answered the surveys also engaged better with the VW service and technology. However, the very high adherence rates to the wearable device across this sample support a positive relationship between patients and the technology.
In our outcomes, we included metrics on alarming. Alarms are related to patient safety, alarm fatigue, and clinical workflow. If alarms are underutilized, early warning signs of patient deterioration could be missed. If alarms are overutilized, patients, caregivers, or HCPs may become desensitized. Alarming for VWs and HaH is different than alarming in a hospital setting. 31 By providing alarming data on this VW service we provide insight into clinical burden and potential alarm fatigue. 32 This could help clinicians manage expectations and staffing based on expected alarm rates.
In a meta-analysis and systematic review of RCTs providing step-down VW care, Chauhan and McAlister 33 found that VWs were associated with fewer ED visits, lower health care costs, and shorter lengths of stay, compared to standard post-discharge care. The WWL VW had slightly higher median LOS at 8 days compared to 6.3 mean days in a national study of over 5000 patients of US hospital care at home programs. 34 The WWL VW had escalations to the ED at 11%, higher than 6.2% in the US study but similar to a smaller study of a COVID-19 VW that reported 9%. 15 This shows us that the WWL VW appears comparable in its metrics to other VW-type services. Escalation to hospital care should not be considered a “failure” - more as evidence that the VW was accepting patients that were truly acute, rather than fit for discharge home.
The VW at WWL was safe for patients with only 17 expected deaths (1%) in the 2-year timeframe of this study. Of those 17 deaths, some were from families that asked for the reassurance and support of monitoring a family member during end-of-life care at home.
Average hospital death rates in the UK are 8.5%, though there is considerable variation. 35 Other VWs report a mortality rate of 1% to 2%, 36 in line with our findings. While it may be that fewer acutely ill patients are admitted to the VW than remain in the hospital, the matched case control study by Jalilian et al 37 still found that WWL VW patients had 63% lower mortality rates than matched hospital inpatients. Levine et al 34 in a national review of acute hospital at home care, found a mortality of 0.5% during care and a 30-day post-discharge mortality of 3.2%. A rapid evidence synthesis found that VW care had mortality rates as good or better than hospitalized patients 38 while another systematic review found a reduced mortality rate for heart failure VW patients compared to hospitalized patients but no reduction in mortality for other diagnoses. 33 While there have not been direct comparisons to hospitalized patients, Bates et al 39 identified adverse events in 1 in 4 hospital admissions with almost a quarter of those being preventable.
Though the VW admits high acuity patients, it will not be ideal for every patient. Patient acuity level of the VW was not measured; therefore, it is unknown how similar the acuity level of the VW population is to patients cared for solely in hospital. The simplified and inclusive clinical pathways WWL used for their VW meant that admitting clinicians had to have the experience and autonomy to include more challenging patients. This could limit use by clinical staff with less experience. The WWL VW team also found it challenging to get clinician buy-in and promote VW awareness, especially for the step-up pathway. To secure clinician buy-in, the WWL VW team regularly communicated the uptake of the VW service from various specialty teams, creating a leaderboard. These successes were shared widely through a newsletter, executive blogs and hospital trust updates. Small group engagement sessions and one-to-one discussions were also utilized to secure uptake and engagement.
It took time and communication to improve clinical acceptability of the service and technology and promote its uptake among GPs. WWL started small, had a few engaged clinicians (ie, clinical champions), 40 showed early results of safety and acceptability, targeted clinicians happy to adopt these VW models, and shared success metrics. They also improved the service model based on feedback from clinical teams and patients. The increased trend for uptake of the VW in general and of step-up care in particular suggests that these tactics were successful (Figure 1).
VWs, enabled by remote monitoring and incorporating step-up care pathways could help manage complex cases across multidisciplinary teams. In lower resource settings, simplified models of remote consultations with intermittent vital sign monitoring could benefit patients requiring prolonged care when a hospital is far or lacking capacity. They can bridge the gap between primary and secondary care, though success relies (in part) on effective integration into a shared electronic patient record. Further research would be useful to assess outcomes for step-up patients, and to identify opportunities for primary care specific pathways.
Researchers and clinicians could refine patient selection criteria and patient stratification. First, to identify patients most likely to benefit from VW services. Secondly, to ensure patients receive the appropriate level of care and monitoring based on their clinical acuity, possibly moving from continuous remote monitoring to intermittent monitoring as they recover.
We recommend that beyond the measures of clinical outcomes, adherence, safety, and patient satisfaction available for this evaluation, measures of cost, patient acuity, 30-day readmission, and the number of hospital bed days a patient had before being stepped down to VW care should be included in VW evaluations. To be meaningful, analyses should be powered and collected once the VW is established. 12
As the aging population grows, infrastructure is strained, and healthcare costs continue to soar, many health systems could benefit from step-up care pathways that keep patients safe and out of hospital beds. This evaluation contributes to the limited evidence base on VW outcomes that include step-up pathways. We have shown here it is safe, effective, and well-liked by patients.
Conclusion
In this application of an expanding VW service we have shown the service is safe and liked by patients, yielded good clinical outcomes, and had no negative impact on adverse events or mortality in this patient sample. The VW service was innovative in its acceptance of a broad range of patients and in developing the step-up pathway. We have shown how to successfully integrate a VW service with primary care and utilize an efficient step-up and step-down approach. This care model could reduce burden on hospitals by reducing length of stay and bypassing hospital admission altogether.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251326750 – Supplemental material for A 2-Year Retrospective Clinical Evaluation of a Novel Virtual Ward Model
Supplemental material, sj-docx-1-jpc-10.1177_21501319251326750 for A 2-Year Retrospective Clinical Evaluation of a Novel Virtual Ward Model by Juliana Pugmire, Abdul Ashish, Alison Chadwick, Matt Wilkes, Daniel Meekin, Ben Zaniello and Nicole Zahradka in Journal of Primary Care & Community Health
Supplemental Material
sj-docx-2-jpc-10.1177_21501319251326750 – Supplemental material for A 2-Year Retrospective Clinical Evaluation of a Novel Virtual Ward Model
Supplemental material, sj-docx-2-jpc-10.1177_21501319251326750 for A 2-Year Retrospective Clinical Evaluation of a Novel Virtual Ward Model by Juliana Pugmire, Abdul Ashish, Alison Chadwick, Matt Wilkes, Daniel Meekin, Ben Zaniello and Nicole Zahradka in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We are grateful to Louise Hough, the UK commercial team, and the clinical teams for their many contributions to supporting this virtual ward.
Authors’ Note
This paper is about a specific hospital, Wrightington, Wigan, and Leigh, within an NHS Trust and a named remote patient monitoring platform, Current Health, used to support the virtual ward being evaluated.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JP, MW, BZ, and NZ. are employees of Best Buy Health Inc., Boston, MA, USA and hold stock in the company.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statements
The collection of this data was considered a service evaluation and was therefore not submitted for NHS Research Ethics Committee review (Health Research Authority, 2022).
Data Availability Statement
The data underlying this study are not publicly available for commercial reasons.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.