
Abstract
Introduction:
The COVID-19 pandemic accelerated telehealth adoption, but disparities in its utilization persist. This study examines primary care patient sociodemographic characteristics, telehealth utilization patterns, and provider adoptions before and during the pandemic.
Methods:
A retrospective cohort study analyzed data from Mississippi Medicare beneficiaries continuously enrolled in Parts A, B, and D who accessed primary care services from 2019 to 2021.
Results:
Among 201 677 Medicare beneficiaries accessing primary care, 1364 used telehealth before the pandemic, compared to 73 994 during the pandemic. Telehealth utilization shifted during the pandemic to younger, female, White beneficiaries, and those enrolled in Medicare due to disability or End Stage Renal Disease. During the pandemic, telehealth users exhibited higher Charlson Comorbidity Index and Social Vulnerability Index but lower Digital Divide Index scores compared to non-telehealth users. Telehealth was associated with more primary care visits, broader access, and higher continuity of care. Primary care physicians increased their share of telehealth services to 39%, while specialties such as neuropsychiatry and psychiatry showed the highest adoption rates, reaching 55% and 38%, respectively.
Conclusions:
Telehealth demonstrated a growing role in primary care during the pandemic. Future efforts must address digital divides and advance health equity when integrating telehealth into primary care services.
Introduction
Primary care is the cornerstone of a functional and equitable healthcare system, providing the regular source of care for early detection and treatment of diseases, chronic disease management, and preventive care.1 -4 However, the COVID-19 pandemic severely disrupted traditional primary care delivery, forcing healthcare systems to adopt new strategies to ensure continuity of care while minimizing the risk of COVID-19 transmission. In response, the Centers for Medicare & Medicaid Services (CMS) introduced a series of Medicare coverage expansions to enable the delivery of healthcare services via telehealth, which were embraced by policy changes from state Medicaid programs and commercial insurers. 5 These policy changes have shaped the landscape of telehealth adoption and utilization in the U.S. While the pandemic propelled telehealth into mainstream healthcare delivery, debates about its future coverage and role in primary care have continued as the public health emergency (PHE) has subsided. 6
The 4 core functions of primary care (4Cs), first contact access, comprehensiveness, coordination, and continuity, are widely recognized as essential contributors to high-quality primary care, associated with better quality services, lower costs, and less inequality.2,7 Primary care physicians have suggested that telehealth has the potential to enhance the 4Cs of primary care by improving access to care and facilitating ongoing management of chronic conditions.8,9 However, recent research suggests that the expansion of telehealth services may exacerbate the existing disparities in primary care utilization, particularly among Medicaid enrollees. 10 Evidence regarding the impact of telehealth on the 4Cs of primary care remains limited, particularly in underserved regions, underscoring the need for further investigation.
To address this gap, we conducted a retrospective study examining primary care telehealth utilization by patients and providers before and during the COVID-19 pandemic in Mississippi, a medically underserved state with one-third of its population residing in primary care health professional shortage areas (HPSAs). 11 This study specifically analyzes variables related to primary care access (eg, number of primary care visits), comprehensiveness (eg, number and proportion of services provided by different specialists), coordination (eg, involvement of specialists in primary care through telehealth), and continuity (eg, Bice-Boxerman Continuity of Care Index). By linking the analysis to the 4Cs, this study seeks to explore how telehealth coverage changes influenced its adoption in primary care and whether its usage patterns aligned with the principles of equitable, accessible, and effective care.
Methods
This retrospective cohort study included Mississippi Medicare beneficiaries who were continuously enrolled in Medicare Parts A, B, and D without Part C coverage from 2019 to 2021 and accessed primary care services. Primary care services were identified using healthcare common procedure coding system (HCPCS) and CMS specialty codes specified in the 2-step attribution method of the CMS. 12 Telehealth services were identified using place of services (02 and 10) and HCPCS modifiers (93, 95, GT, GQ, G0, and FQ). Beneficiaries with at least 1 primary care claim billed with telehealth services were classified as telehealth users, while those without such claims were classified as non-telehealth users. Beneficiary telehealth grouping, along with sociodemographic characteristics and primary care utilization, were analyzed for 2 time periods: before COVID-19 (January 1, 2019 to February 28, 2020) and during COVID-19 (March 1, 2020 to December 31, 2021).
Demographic variables included age, sex, and race. Race was categorized into 3 groups, White, Black, and Other. The Other race category included beneficiaries identified as Asian, Hispanic, North American Native, and others. Unknown race was treated as missing. Socioeconomic characteristics included the original reason for entitlement (Old Age and Survivor’s Insurance (OASI), Disability Insurance Benefits (DIB), and End Stage Renal Disease (ESRD)), Medicare-Medicaid dual enrollment, residential rurality (defined using Rural-Urban Commuting Area (RUCA) codes 4-10), 13 and primary care HPSA designation. 14 The RUCA codes and HPSA designation were determined using residential zip codes. The Charlson comorbidity index (CCI) was used to summarize patient comorbidities. 15 Social vulnerability index (SVI) and Digital Divide Index (DDI) were measured at the beneficiary residential county level through the Federal Information Processing System (FIPS) codes to quantify social determinants of health and assess the additional support in accessing telehealth.16,17 The SVI consisted of 4 themes, socioeconomic status, household characteristics, racial and ethnic minority status, and housing type and transportation, with scores ranging from 0 to 1, where higher values indicate greater vulnerability. 16 The DDI was measured with 2 components, infrastructure/adoption score (INFA) and socioeconomic scores, with values ranging from 0 to 100, where higher values indicate a greater divide. 17
Primary care utilization was measured by the number of primary care visits per month and by access, defined as whether beneficiaries received care from different provider types, including primary care physicians, nonphysician practitioners, medical specialists, surgeons, and other physicians. 12 Additionally, the proportion of services provided by each provider type was calculated. The Bice-Boxerman Continuity of Care Index (COCI), ranging from 0 to 1 with higher values indicating greater continuity of care among fewer providers, was used to measure the care continuity at the beneficiary level. 18
Descriptive statistics were reported to summarize beneficiary characteristics by primary care telehealth utilization before and during the COVID-19 pandemic. The magnitude of differences between telehealth users and non-users was assessed using odds ratios (ORs) and chi-square tests for categorical variables, as well as mean differences and Wilcoxon rank-sum tests for continuous variables. Visual aids were used to describe the percentage of telehealth services provided by each type of provider and the percentage of primary care delivered via telehealth across specialty provider types, including medical specialists, surgeons, and other physicians.
Results
A total of 201 677 Medicare beneficiaries were included in the analysis, with 1364 beneficiaries accessing primary care through telehealth before the COVID-19 pandemic and 73 994 during the pandemic.
Sociodemographic Characteristics
Table 1 displays the patient sociodemographic characteristics by telehealth utilization. Before the COVID-19 pandemic, primary care telehealth was more likely to be accessed by beneficiaries who were younger, male, Black, enrolled in Medicare due to disability, dually enrolled in Medicare and Medicaid, and residing in rural or HPSA-designated regions. During the COVID-19 pandemic, telehealth use shifted toward beneficiaries who were younger, female, White, and enrolled in Medicare due to disability or ESRD being more likely to access telehealth services, while those dually enrolled in Medicaid or resided in rural or HPSA-designated regions were less likely to use telehealth. Although younger beneficiaries consistently had higher odds of accessing primary care telehealth compared to older groups, the magnitude of this association decreased during the pandemic, with ORs increasing from less than 0.6 to over 0.6 across all age groups.
Patient Sociodemographic Characteristics by Period (N = 201 677).
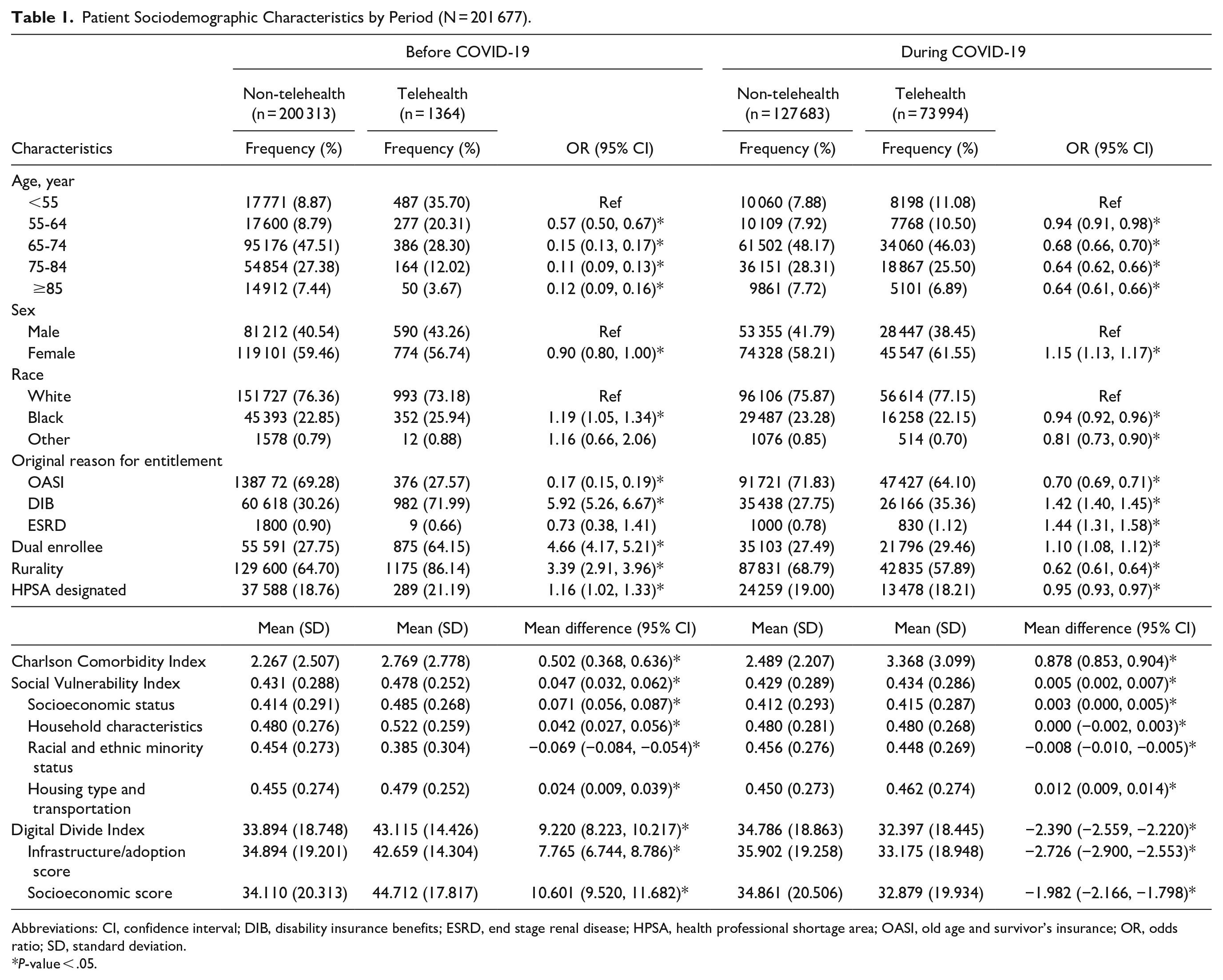
Abbreviations: CI, confidence interval; DIB, disability insurance benefits; ESRD, end stage renal disease; HPSA, health professional shortage area; OASI, old age and survivor’s insurance; OR, odds ratio; SD, standard deviation.
P-value < .05.
When examining indices, telehealth users had higher CCI scores than non-users, with mean differences of 0.502 (95% CI = 0.368, 0.636) before COVID-19 and 0.878 (95% CI = 0.853, 0.904) during the pandemic. Telehealth users also consistently exhibited significantly higher SVI scores compared to non-users across both periods. Significant differences were also observed across all SVI themes, with telehealth users exhibiting higher scores compared to non-users, except for the racial and ethnic minority status theme, where telehealth users had lower scores, as indicated by mean differences of −0.069 (95% CI = −0.084, −0.054) before COVID-19 and −0.008 (95% CI = −0.010, −0.005) during the pandemic. Additionally, telehealth users had higher DDI scores before the pandemic, with higher infrastructure/adoption and socioeconomic component scores. However, during the pandemic, telehealth users exhibited significantly lower DDI scores, with decreases in both components compared to non-users.
Patient Primary Care Utilization
Table 2 presents the primary care utilization among patients. Before the COVID-19 pandemic, telehealth users were more likely to access nonphysician practitioners and medical specialists compared to non-users, with ORs of 4.44 (95% CI = 3.75, 5.25) and 1.66 (95% CI = 1.47, 1.88), respectively. During the COVID-19 period, telehealth users were more likely to access all provider types, including primary care physicians (OR = 2.18), nonphysician practitioners (OR = 2.71), medical specialists (OR = 2.28), surgeons (OR = 1.57), and other physicians (OR = 1.54).
Patient Primary Care Utilization by Period (N = 201 677).
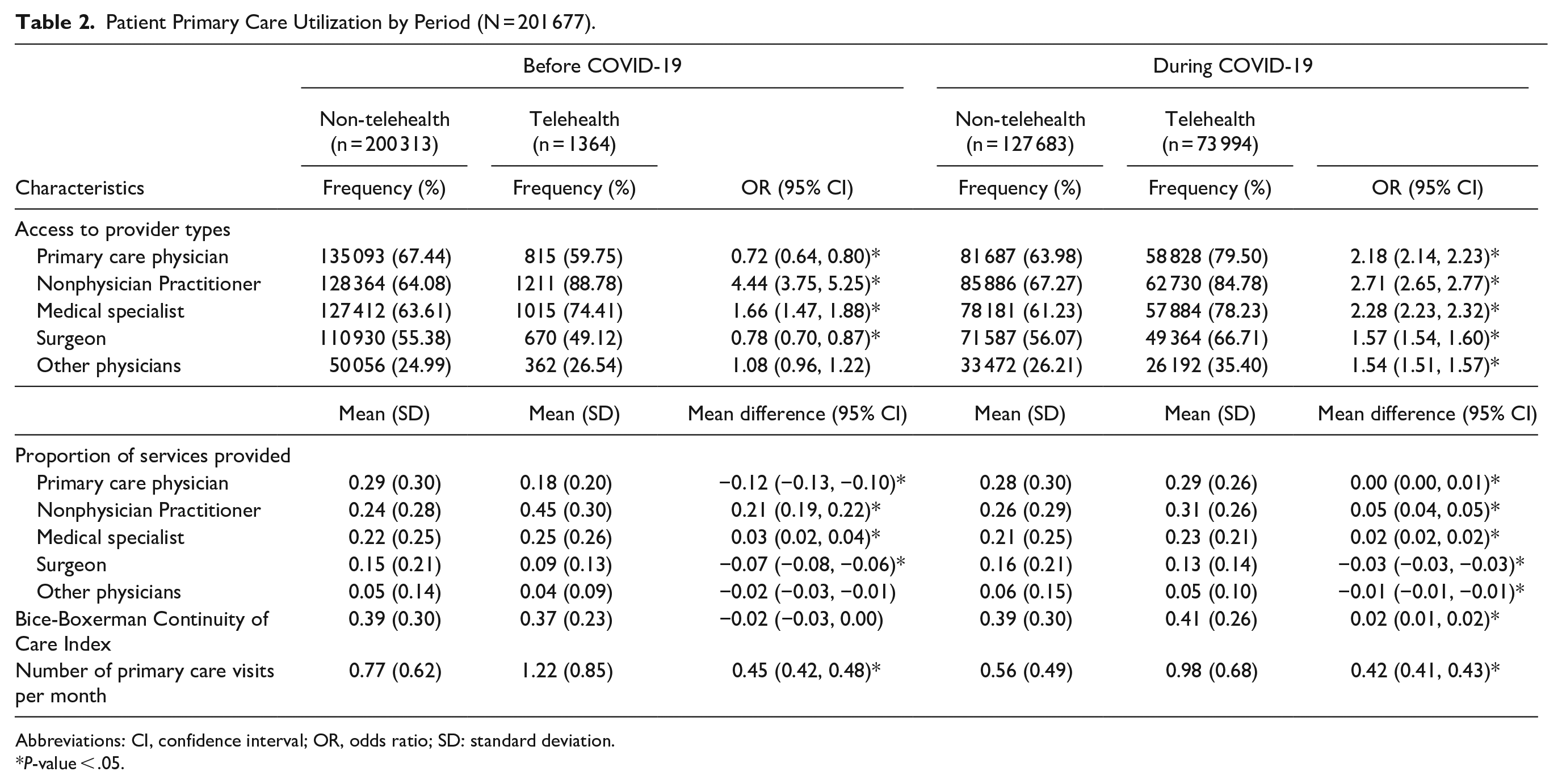
Abbreviations: CI, confidence interval; OR, odds ratio; SD: standard deviation.
P-value < .05.
Additionally, nonphysician practitioners and medical specialists provided a higher proportion of primary care services to telehealth users than non-users before the pandemic. A similar pattern was observed during the pandemic, although the magnitude of these differences decreased. Before COVID-19, the absolute differences in the proportion of services provided to telehealth users versus non-users were 0.12 for primary care physicians, 0.21 for nonphysician practitioners, 0.03 for medical specialists, 0.07 for surgeons, and 0.02 for other physicians. During the pandemic, these absolute differences decreased to 0.00, 0.05, 0.02, 0.03, and 0.01, respectively.
Although the types of providers differed, telehealth utilization was associated with an increase in primary care visits during both time periods. On average, telehealth users accessed 0.45 (95% CI = 0.42, 0.48) more primary care visits per month than non-users before COVID-19 and 0.42 (95% CI = 0.41, 0.43) more visits during the pandemic. Telehealth users had lower Bice-Boxerman COCI scores before the pandemic, with a mean difference of −0.02 (95% CI = −0.03, 0.00), but significantly higher COCI scores during the pandemic, with a mean difference of 0.02 (95% CI = 0.01, 0.02).
Telehealth Utilization by Primary Care Providers
Figure 1 illustrates the quarterly distribution of telehealth services by provider type from Quarter 1 (Q1) 2019 to Q4 2021. Before the COVID-19 pandemic, telehealth services were predominantly provided by nonphysician practitioners and medical specialists. However, during the pandemic, the shares of telehealth services provided by nonphysician practitioners and medical specialists decreased, while primary care physicians increased their share of telehealth services during the pandemic to 39.2% in Q4 2021. Other provider types, including surgeons and other physicians increased telehealth services, but still contributed minimally to telehealth services, with their combined share remaining below 10% throughout the period.

Percentage of telehealth services provided by provider type over time.
Figure 2 displays the proportion of services provided via telehealth by provider specialty across medical specialists, surgeons, and other physicians. Neuropsychiatry, psychiatry, interventional pain management, preventive medicine, and allergy and immunology had the highest rates of telehealth utilization during the pandemic, with neuropsychiatry reaching over 55% adoption and psychiatry reaching 38%.

Percentage of telehealth services provided by specialty (medical specialists, surgeons, and other physicians).
Discussion
While telehealth policies during the pandemic aimed to broaden access, their real-world impacts were uneven. This study examined the patient characteristics and primary care utilization patterns of Mississippi Medicare beneficiaries who accessed telehealth before and during the COVID-19 pandemic, providing evidence to guide telehealth policy in the post-pandemic era.
Before the pandemic, telehealth policies primarily benefited rural residents. 19 Telehealth users were younger, male, Black beneficiaries who were dually enrolled in Medicaid, enrolled in Medicare due to disability, and residing in rural or HPSA-designated regions. Telehealth users exhibited higher CCI, SVI (except for racial and ethnic minority status), and DDI scores, reflecting poorer health status, greater social vulnerability, and limited digital infrastructure in their neighborhoods. Lower SVI scores for racial and ethnic minority status suggest these groups were less likely to use telehealth, consistent with existing literature on telehealth disparities. 20
However, during the pandemic, the coverage expansion fostered a shift in telehealth utilization. Higher adoption was observed among younger, female, White beneficiaries who were not enrolled in Medicaid, enrolled in Medicare due to disability or ESRD, and resided in non-rural or non-HPSA designated regions. ORs closer to 1 during the pandemic indicate that telehealth expansion policies, such as expanded reimbursement and relaxed geographic restrictions, have facilitated broader utilization with reduced access disparities, particularly among individuals with fewer healthcare disadvantages. This shift was echoed in SVI findings, where telehealth users had more similar SVI scores to non-users during the pandemic, compared to the larger differences observed before COVID-19. Lower DDI scores among telehealth users during the pandemic further reflect better socioeconomic status and improved infrastructure readiness, highlighting the effectiveness of policy changes in expanding access while emphasizing the ongoing need to address digital disparities and barriers faced by more vulnerable populations.
Implications for Primary Care Utilization and Practice
By facilitating more accessible care, telehealth has the potential to enhance first contact access. Before the pandemic, primary care telehealth services were predominantly delivered by nonphysician practitioners and medical specialists, who were also the most commonly accessed providers for telehealth users. In primary care practices, nonphysician practitioners often collaborate with physicians to support patient-centered care. 21 The observed predominant role of nonphysician practitioners highlights the capacity of telehealth to support care coordination and team-based care delivery, as well as the need to strengthen coordination between telehealth and traditional primary care to ensure seamless integration of services.
During the pandemic, telehealth adoption expanded to include a broader range of provider types, including primary care physicians, surgeons, and other specialists. This shift reflects the adaptability of telehealth to meet the increased demand for comprehensive care when in-person access was limited. The significant increases in the proportion of telehealth services provided by most specialists, as shown in Figure 2, further support the role of telehealth in enhancing the comprehensiveness of primary care. However, this increasing diversity in provider contributions also highlights the need for mechanisms to improve care coordination.
With policy expansions during the pandemic, telehealth users exhibited higher Bice-Boxerman COCI scores compared to non-users, suggesting improved continuity of care among fewer providers. Consistent with findings from community health centers, 22 this finding underscores the potential of telehealth in strengthening patient-provider relationships and enabling ongoing care management, even during periods of limited in-person access. Collectively, these results emphasize telehealth as a valuable tool for advancing the 4Cs of primary care while highlighting the need for continued efforts to effectively integrate telehealth services into the broader primary care landscape.
Limitations
This study is limited to Medicare beneficiaries in Mississippi, a Deep South state with limited healthcare resources and a population primarily comprising seniors, individuals with disabilities, and ESRD patients. While these findings reflect the typical needs of a medically underserved region, resonating with existing findings of the nationwide Medicare Advantage and commercially insured enrollees, 23 they may have limited generalizability to other states or populations. While the data-driven approach provides a comprehensive view of primary care usage, the claims data lack context of these services, such as whether they were patient-initiated or provider-encouraged. Additionally, telehealth utilization during the pandemic may have been influenced by mandated social distancing measures, which could differ in the post-pandemic era. Future efforts should focus on sustaining provider adoption of telehealth in a post-pandemic context. 24 Finally, while this study considers the 4 core functions of primary care, it does not evaluate clinical outcomes directly. Future research should examine the long-term impact of telehealth on health outcomes and healthcare utilization to provide a more comprehensive understanding of its effectiveness, both overall and by provider types.
Conclusion
This study highlights the evolving role of telehealth in primary care, particularly during the COVID-19 pandemic. Facilitated by policy expansions, we observed significant shifts in telehealth utilization patterns, with broader adoption and reduced access disparities. Our findings also highlight its potential to enhance primary care through the 4 core functions. Despite these advancements, the increased access among individuals with fewer healthcare disadvantages highlights the need for targeted efforts to ensure equitable access for underserved populations. Future efforts should prioritize addressing barriers faced by individuals with greater social vulnerabilities, with a particular focus on mitigating digital divides and improving access to telehealth. Moreover, sustained efforts are needed to support provider adoption and ensure the seamless integration of telehealth into primary care workflows. By addressing these challenges, telehealth can solidify its role in high-quality primary care, promoting improved health outcomes for all populations.
Footnotes
Author Contributions
Conceptualization: All authors; Methodology: All authors; Formal analysis and investigation: All authors; Writing—original draft preparation: YZ; Writing—review and editing: All authors; Funding acquisition: YZ and SC; Resources: YZ and SC; Supervision: SC and JMS.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LSL is an employee of Immunovant, Inc. Other authors have no conflicts of interest to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the Office for the Advancement of Telehealth, Health Resources and Services Administration, U.S. Department of Health and Human Services under the National Telehealth Centers of Excellence Award (U66RH31459). The information, conclusions, and opinions expressed are those of the authors and no endorsement is intended or should be inferred.
Ethical Consideration
This study was approved by the Institutional Review Board (No. 2021-1058) of the University of Mississippi Medical Center with a waiver of informed consent and HIPAA authorization.
Consent to Participate
Informed consent to participate was waived.
Consent for Publication
Not applicable.
Data Availability
Due to restrictions stipulated in the data use agreement with the Centers for Medicare & Medicaid Services (CMS), sharing of identifiable Medicare research data is prohibited.