
Abstract
Introduction:
Cervical Cancer (CC) is a preventable and treatable disease if detected early, yet it remains a global health challenge. In Ecuador, CC is the second most common cancer; however, screening uptake remains suboptimal due to poor knowledge, low willingness, and limited access to healthcare. Traditionally, CC screening requires a healthcare professional, creating social and access barriers. Innovative techniques such as “self-sampling” (SS) for human papillomavirus (HPV) detection offer a promising alternative.
Objective:
This study evaluates the acceptability, attitudes, and user experience of a community-based SS program among a hard-to-reach population following a local educational session.
Methods:
A quasi-experimental study was conducted in a rural community in Cuenca, Ecuador. Educational sessions were organized, after which women were offered the option to perform SS for HPV detection. Three questionnaires were administered to assess population characteristics, risk factors, and experiences toward the process.
Results:
Of the 130 participants, 90% accepted SS, and 10% rejected SS. A significant number of women reported that SS was faster and less painful compared to traditional Papanicolaou tests (P < .05).
Conclusions:
SS shows strong potential for increasing CC screening, especially in hard-to-reach areas, emphasizing the need to adapt screening programs to meet diverse community needs.
Introduction
Cervical cancer (CC) is a preventable and curable disease when detected in its early stages, according to the World Health organization (WHO). However, it remains one of the most common cancers, claiming the lives of thousands of women worldwide annually.1,2 Globally, CC is the fourth leading cause of cancer-related deaths among women, with approximately 350 000 fatalities reported in 2022. 1 In Ecuador, CC ranks as the second most common cancer, accounting for 1792 new cases and 939 deaths in 2022.3,4
The strong association between Human papillomavirus (HPV) and CC is well-documented in both biological and epidemiological contexts. Fourteen high-risk HPV (HR-HPV) types, including 16 and 18, are responsible for approximately 70% of CC cases. 5 Conversely, low-risk HPV (LR-HPV) types, such as types 6 and 11, are associated with genital warts and cutaneous lesions. 6 Despite the prevalence of HPV infections, approximately 90% of cases resolve spontaneously within 2 years. 7
HPV testing assesses the presence of HR-HPV types given their associations with the development of CC,8,9 while Papanicolaou tests, also known as Pap smears, identify cellular changes in the transformation zone. 10 Co-testing (HPV testing and Papanicolaou test) performed every 5 years is one of the recommended screening strategies for women aged 30 to 65 years to enhance the accuracy of CC screening by evaluating both viral infection and cellular changes.11,12
Routine CC screening is typically conducted using a Papanicolaou test, which in Ecuador has a sensitivity and specificity of approximately 75% and 50%, respectively. 13 However, multiple barriers hinder the implementation of comprehensive CC preventive programs, resulting in screening coverage of only 58.4% among Ecuadorian women aged 12 to 49 years who have ever been examined for CC prevention.14,15 National guidelines recommend conducting Papanicolaou test every 3 years for women aged 30 to 65 years. 13
Practical, psychosocial, and emotional barriers significantly contribute to the low participation in CC screening. These barriers include geographical constraints, social inequities, lack of time, inadequate risk perception, limited knowledge, fear, discomfort, embarrassment, cultural beliefs, and distrust of the healthcare system.16-18 Such factors are particularly pronounced among “hard-to-reach” women. 19 Addressing these barriers requires tailored strategies, including improved management of stigma and poverty, increased educational initiatives, and enhanced health promotion efforts across individual, community, organizational, and policy levels. 18
Educational initiatives have proven essential in increasing CC awareness, particularly in rural communities. 20 In Ecuador, studies have shown that many women of reproductive age, especially in rural and indigenous communities, lack adequate knowledge about CC screening, its causes, and its consequences, further hindering screening uptake.21 -23
Traditional CC screening typically involves a healthcare professional collecting samples. However, self-sampling (SS) techniques, which enable women to collect cervicovaginal samples for HPV detection independently, offer a viable alternative. 24 SS methods, such as vaginal and urine sampling for HPV, have demonstrated high sensitivity (94.4% and 88.8%, respectively) and specificity (92.1% and 94.1%, respectively). 13 With comparable validity to samples collected by healthcare professionals, SS is particularly valuable for under-screened or never-screened populations. 25
SS can be conducted in healthcare facilities or offered in community settings, extending its reach to women who may otherwise lack access to these services. SS kits typically include a brush or swab for collecting cells from the cervix and lower genital tract, along with detailed instructions.13,26 Evidence suggests that SS is an acceptable and effective alternative, particularly in rural areas where conventional screening faces logistical challenges. 18
In Ecuador, few studies have evaluated the acceptability of SS methods, especially in community contexts outside healthcare facilities.13,27,28 This study aims to assess the acceptability, attitudes, and user experiences of SS following an educational intervention among a hard-to-reach population, historically hindered by geographical, economic, and/or cultural barriers to healthcare access.
Methodology
Study Design
This study involved an intervention combining an educational session on CC and its screening methods with the option for SS.
Study Population and Participants
The study was conducted in the rural community of Sinincay, located in Cuenca, Ecuador, between December 2022 and August 2023. Sinincay has a population of approximately 26 500 inhabitants, including around 12 000 men and 14 000 women. Women aged 30 to 65 years accounted for 5800 individuals of the population. 29 They can be considered as hard-to-reach women. In 2022, only 161 women underwent a traditional Papanicolaou test at the local healthcare facility, according to the health center records.
All women in the community were invited to participate in the educational session, and from this group, those meeting the inclusion criteria were identified as eligible for the study. Ultimately, 130 eligible women were enrolled form a preselected sample based on the criteria outlined below.
Inclusion Criteria
Eligible women were required to be aged 30 to 65 years, had ever been sexually active, had no prior diagnoses or treatments for CC, had no history of hysterectomy, were not currently pregnant, were Spanish-speaking, and were able to provide informed consent.
Exclusion Criteria
Women were excluded from SS if they were menstruating at the time of sampling, had used any vaginal medication (such as creams or ovules) within the previous 48 h, or had engaged in sexual intercourse within 48 h before the SS session. Women who met any exclusion criteria but wished to undergo SS were advised to return at a later time when eligible. The exclusion of active bleeding (menstruation) followed the manufacturer’s recommendations for the Evalyn® Brush and established Papanicolaou test guidelines, as the presence of blood may compromise sample quality and interfere with test results.30,31 Although HPV testing is not strictly equivalent to pap testing, similar exclusion criteria were applied.
Recruitment
As outlined in Figure 1, the recruitment process was carried out in collaboration with various community leaders, including parish presidents, local priests, church members, healthcare professionals, school principals, and representatives from the local government. Invitations to the educational sessions were distributed through community meetings, church gatherings, health center promotions, and health fairs. Additionally, pamphlets specifically developed for this study were disseminated to high school students, placed at bus stops, and shared on social media platforms. These pamphlets provided detailed information about the educational sessions, including the date, time, and location.

The initial approach process followed in the Sinincay community.
Intervention Implementation
The intervention consisted of 3 stages: an educational session, the option to perform SS, and a follow-up 3 months post-intervention. Three questionnaires were administered to eligible participants. These instruments were developed by the research team and validated through a pilot study involving women from a different community.
Questionnaire 1 (Q1) collected socio-demographic data and screening habits. Questionnaires 2 (Q2) and 3 (Q3), which assessed pre- and post-test knowledge regarding SS, were based on a Likert scale and did not allow participants to provide additional explanations. Participants selected the option that best aligned with their perception from a predefined set of options.
First Stage: Educational Intervention
Before the educational session, participants completed a self-administered questionnaire (Q1) designed to gather information on socio-demographic characteristics, condom use, risk perception, and screening habits.
The 20-minute educational session was facilitated by field researchers and delivered in simple language using clear and engaging visuals. Key topics included CC causes, progression, symptoms, prevention, and available screening methods. Detailed instructions on SS were provided using a sample “Evalyn Brush” (Rovers, The Netherlands), with a live demonstration to ensure participant understanding. To reinforce the information, a video, created specifically for the population was shown following the demonstration. The participants were offered the option to undergo a SS test.
Second Stage: Self-Sampling
After the educational session, participants completed Questionnaire 2 (Q2), which assessed their attitudes toward SS using Likert scale measurements, while reasons for actual acceptance or refusal of SS were captured through a predefined set of options, allowing participants to select the response that best aligned with their perspective. Participants who accepted SS were then invited to perform SS in a private room within the community municipal hall. Women who could not undergo SS on the same day due to exclusion criteria were given the opportunity to visit a designated facility at a later date.
Following the SS procedure, participants completed Questionnaire 3 (Q3), which gathered feedback on their experience with SS, reassessing the same attitudes evaluated in Q2 using Likert scale measurements. It also allowed participants to reflect on and share their actual experiences with SS. The educational sessions and SS collection period lasted 3 months, concluding in March 2023.
A medical professional personally delivered the SS test results to each participant at the same venue where the SS procedure was conducted (Figure 2).

Flowchart of the process followed in the Sinincay community.
Sample Collection
Self-sampling test
Women who consented to participate in SS test received a kit containing an Evalyn Brush and a step-by-step instruction brochure (provided by the manufacturer) in Spanish. The SS procedure was conducted on-site in a private setting, such as a bathroom at the designated venue.
Upon delivery to the Laboratory of Molecular Biology, the Evalyn brushes were washed with Hank’s Balanced Salt Solution from Mole Bioscience. DNA Extraction was performed using the Nucleic Acid Extraction Kit (Boiling Method) according to the manufacturer’s protocol (Mole Bioscience). Samples were either processed immediately or stored at 4°C for future testing. HPV genotyping was carried out using the 24 HPV Typing Kit (Jiangsu Mole Bioscience), with real-time PCR conducted on an Exicycler™ 96 thermocycler (Bionner).
Data analysis
Descriptive statistics were calculated to determine frequencies, means, and percentages for key variables. Pre-test and post-test evaluations were analyzed using descriptive statistics. The analyses were conducted using the ggplot2 package (version 3.4.2) and RStudio (version 2023.03.0; Posit Software, Boston, MA, USA).
Results
A total of 11 educational sessions were conducted across the community, with an average attendance of 12 eligible women per session, achieving the preselected sample size of 130 participants.
Characteristics and SS Uptake
The socio-demographic characteristics, condom use, risk perception, and screening uptake are summarized in Table 1.
Characteristics and SS Uptake of Women From the Community of Sinincay.
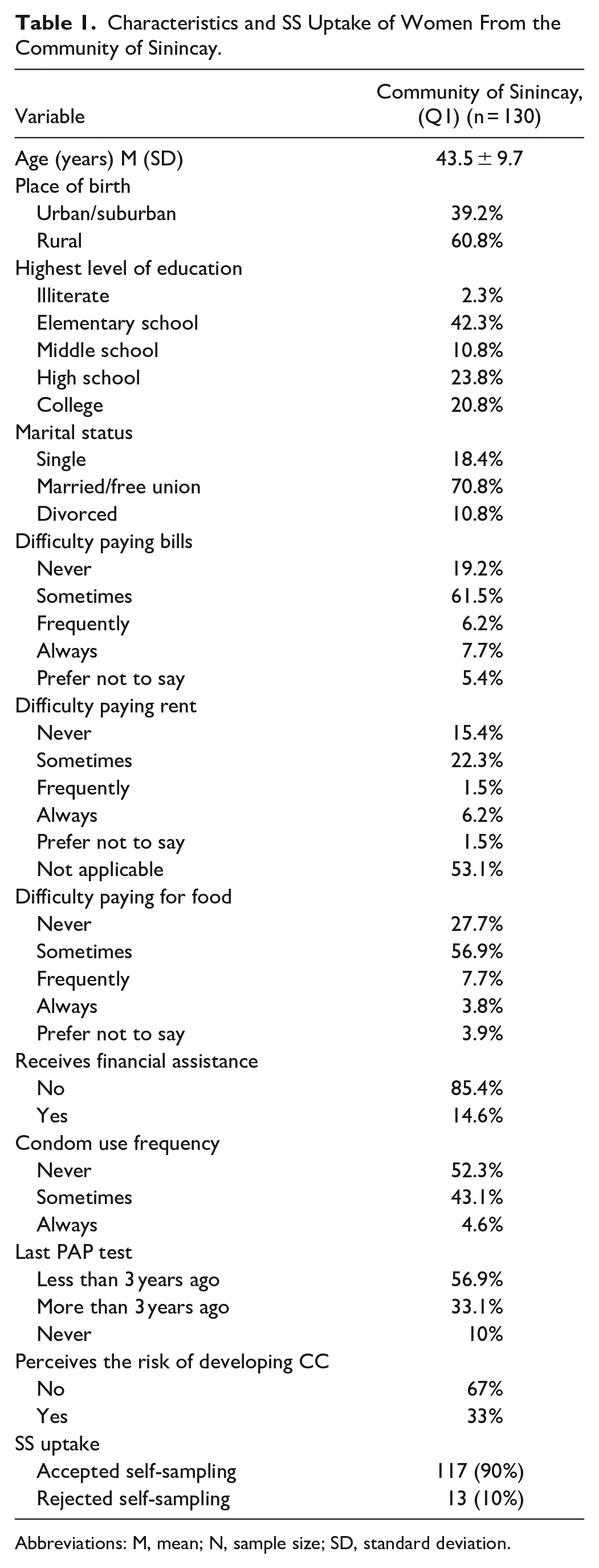
Abbreviations: M, mean; N, sample size; SD, standard deviation.
The results presented in Table 1 reveal that the average age of participants was 43.5 years. The majority (60.8%) were born in rural areas. Regarding education, 42.3% of participants had attained only elementary-level schooling. Most participants (70.8%) were either married or in a free union. Financial challenges were commonly reported among participants: 75.4% struggled to pay bills, while 68.4% experienced difficulty affording food. Around 30% of women faced challenges paying rent, although 53% reported not having rental expenses. Many participants (85.4%) did not receive any form of financial assistance. In terms of sexual behaviors, more than half of the participants (52.3%) reported never using condoms. Regarding CC screening, 10% had never undergone a pap test, while 33% had not been tested in over 3 years. Notably, only 33% perceived themselves as being at risk of developing CC. Out of the 130 participants, 117 women (90%) accepted the SS procedure, while 13 (10%) declined (Table 2).
Reasons for Accepting or Non-uptake SS Before Offering the Test.

n, sample size.
The 3 most commonly mentioned reasons for accepting SS were not needing an appointment (23%), the simplicity of the procedure (20%), and less embarrassing (20%). Among those who declined SS, 15% preferred a doctor to perform the test, 8% thought it would be painful, and another 8% were afraid of not performing the test correctly. Additionally, 69% of those who initially declined SS were menstruating at the time of the educational session and did not return later to perform SS despite being given the opportunity. Although menstruation is not a permanent exclusion criterion for SS, cultural considerations guided the decision not to perform SS during menstruation to avoid participant discomfort. This approach aligns with the manufacturer’s recommendations.
HPV Prevalence
Among the 117 participants who underwent SS, 70.1% tested negative for HPV, while 28.2% tested positive, with HR-HPV types comprising 75.7% of positive results. Coinfections were identified in 10.3% of cases, with HPV16 (15.6%) and HPV31 (13.3%) being the most prevalent genotypes detected. In 2 cases, it was not possible to obtain results due to a lack of DNA, resulting in 1.7% being classified as insufficient samples.
Attitudes Toward and User Experiences of Self-Sampling
Participants completed questionnaires before (Q2) and after (Q3) undergoing the SS procedure. Results summarizing the perception of SS are presented in Table 3. While 130 women initially participated in the study, the analysis of perceptions focuses exclusively on the 117 women who accepted SS to compare their perceptions about SS (after receiving the explanation) with the actual experience (after taking the SS; Table 4).
Results of Molecular Biology Test for HPV Diagnosis.

n, sample size.
HPV 59,42,81,51,6,33,82,45,66,43,18.
Perceptions Before and Experiences After SS.

n, sample size.
The questionnaire responses revealed significant differences in perceptions before and after the SS procedure. A notable increase in agreement regarding quick testing was observed from pre-test to post-test, with a rise from 22.2% to 56.4%, indicating an improvement in participants’ perception of the testing process. Regarding pain perception, 13.7% of participants disagreed with feeling pain in the pre-test, compared to 47% in the post-test, suggesting a more positive experience in the post-test. There was a substantial improvement in the perception of the test being easy, with 18.8% in the pre-test compared to 47% in the post-test, highlighting a more favorable response in the post-test. The need for additional information slightly decreased from 2.6% in the pre-test to 1.7% in the post-test, showing minimal change. The requirement for assistance also saw a slight reduction, from 4.3% in the pre-test to 1.7% in the post-test, though this change was not highly significant. Confidence in correctly taking the test increased significantly, from 24.8% in the pre-test to 41.9% in the post-test. Trust in the results showed a modest improvement, increasing from 39.3% in the pre-test to 47% in the post-test. The perception of embarrassment slightly increased from 57.3% in the pre-test to 59% in the post-test, showing minimal change. Comfort during the test significantly improved, rising from 27.4% in the pre-test to 46.2% post-test, indicating a more positive experience. Nervousness levels remained stable, with 5.1% reported in both the pre-test and post-test, showing no significant change. Perception of privacy notable increased notably, from 38.5% in the pre-test to 54.7% in the post-test, demonstrating a significant improvement.
Discussion
This study focused on addressing challenges in CC screening among hard-to-reach women in the rural community of Sinincay, Ecuador, and to evaluate SS as a potential strategy to increase participation in screening programs. Geographical and socio-economic barriers, coupled with perceptions of embarrassment related to clinician-collected Papanicolaou tests and the distance to healthcare facilities, contribute to low participation in routine CC screening leading to under-screened women.18,32
Socioeconomic and educational challenges were prevalent among the participants: 42.3% had only elementary-level education, and 23.8% had completed high school. Financial difficulties were significant, with 75.4% struggling to pay bills, 30% reporting difficulties in paying rent, and 68.4% finding it challenging to afford food. These economic constrains intersect with limited educational level, further exacerbating healthcare access disparities.
CC risk factors were also prominent. More than half of the participants (52.3%) reported never using condoms, while 43.8% used them occasionally, increasing their vulnerability to sexually transmitted infections (STIs), including HPV. Moreover, 33.1% of women had not undergone a Papanicolaou tests in over 3 years, and 10% had never had one. These data reflect a higher risk of HPV infection and CC development, exacerbating by socio-economic and education barriers. The lack of condom use, inadequate CC screening, and absence of prior Papanicolaou tests are further contributing risk factors.33,34 This is consistent with the findings that 28.2% of participants tested positive for HPV, with high-risk types HPV16 (15.6%) and HPV31 (13.3%) being the most common, consistent with trends observed in the region. 35
Barriers such as limited education and insufficient healthcare services impede CC awareness and contribute to under-screening.36,37 It is essential to highlight that CC prevention and screening strategies need an educational component to overcome these barriers. Only 33% of participants perceived themselves to be at risk of developing CC, reflecting inadequate knowledge about its causes, risks, and consequences. Educational interventions, as implemented in this study, have been shown to improve participation and adherence to CC prevention initiatives. 20
The acceptability of SS was high, with 90% of participants choosing to perform SS, underscoring its potential as a culturally sensitive and accessible alternative to clinician-administered Papanicolaou tests. This preference aligns with findings from the Di Gennaro study, 16 where women at higher risk, including those who had never undergone a pap test before, preferred SS over a doctor-administered pap test. Previous studies by Morán 38 and Levinson 39 reported similar preferences for SS, with acceptability rates of 68% and 81.4%, respectively. For under-screened populations, the high acceptability of SS is crucial for improving CC screening coverage and, consequently, reducing CC-related morbidity and mortality.
Despite its numerous advantages, SS has yet to become a standard component of routine CC screening in Ecuador, even though it holds significant potential to overcome barriers, particularly for underserved populations. In Ecuador, limited research has assessed the acceptability and utility of SS in hard-to-reach communities, reinforcing its high acceptance rate and the need for increased CC screening efforts.13,40 The advantages cited by participants include convenience, ease of use, painlessness, comfort, independence, lack of nervousness, confidence in accuracy, trust in results, minimal embarrassment, and preference for future testing (P < .05). These findings resonate with other studies that emphasize SS as a less invasive, efficient, and more private alternative to clinician sampling.24,38,39,41-50
The most cited reason for accepting SS (23%) was the convenience of not requiring an appointment, while menstruation was the primary barrier among those who initially declined SS. It is worth noting that 69% of women who rejected SS did so because they were menstruating at the time, not because of SS itself.
These findings reaffirm the efficacy of SS in overcoming barriers related to pain, ease of use, speed, and privacy, as demonstrated in previous research.38,51-53 Integrating SS into national screening programs could significantly enhance participation rates, particularly in rural and hard-to-reach communities.
Limitations of the Study
One limitation of the study is the potential for selection bias, as participants were women who voluntarily agreed to participate and met specific inclusion criteria. This could mean the sample predominantly consisted of women already interested in preventive health, which is reflected in the reported screening uptake: 57% of participants stated they had been screened in the past 3 years (besides the low number of reported pap smears in the local health center). However, self-reported screening uptake may be overestimated, as some women may not understand which procedures were performed during a past gynecological examination (women answered Q1 before the educational session so before receiving information about cervical cancer screening).
Additionally, the uptake of self-sampling (SS) may have been influenced by study exclusions. Many women were ineligible to participate because they were menstruating at the time, which could have affected overall SS uptake.
Conclusion
These findings emphasize the need for CC screening programs to be tailored to the specific needs and preferences of different communities, particularly in rural areas with limited access to healthcare services. The 90% acceptance rate of SS, along with the positive attitudes and experiences reported by participants, highlights the potential of SS to overcome significant barriers to screening. These results suggest that SS could play a pivotal role in enhancing CC screening efforts in underserved rural settings. To address existing disparities in education, economic status, and health awareness, further research and targeted interventions are crucial. Ensuring equitable access to screening and prevention services across all populations is imperative to reduce the burden of CC and improve health outcomes in marginalized communities.
Footnotes
Acknowledgements
We extend our heartfelt thanks to all the women who participated in this study. We are deeply grateful for your invaluable contributions to this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of the ELEVATE consortium, which has received funding from the European Union’s Horizon 2020 research and innovation program under grant agreement No 825747. It also receives funding from the Vicerrectorado de Investigación of the University of Cuenca, Ecuador.
Ethical Approval
The study received approval from the Ethics Committee for Health Research at the University of Cuenca-CEISH No: 2018-074EO-I, under the supervision of the Ministry of Public Health.
Consent to Participate and Publication
Written informed consent was obtained from all participants before their participation in the study.
Statements and Declarations
Not applicable
ORCID iDs
Data Availability
The data are available from the corresponding author upon reasonable request. Due to privacy and ethical concerns, data are not publicly available in a repository but will be shared with qualified researchers under specific conditions.