
Abstract
Introduction:
Parent training (PT) programs are recognized as effective interventions that enhance parenting techniques and improve the parent-child relationship. In Japan, these programs are increasingly implemented to help parents manage behavioral issues in children. This study evaluated the effectiveness of PT pamphlets designed and distributed in Shioya Town, Japan, by comparing outcomes between the intervention and control groups and within subgroups of parents, categorized based on their children’s need for follow-up health checkups.
Methods:
The study included an intervention group that received PT pamphlets during their 1.5-year health checkups and a control group that did not. Data were collected through self-administered questionnaires at the 3.5-year health checkups, assessing adherence to 3 recommended parenting techniques. The analysis focused on comparing intervention and control groups, evaluating adherence to 2 recommended parenting techniques versus one or none. The study also analyzed adherence to each recommended parenting technique within subgroups of parents whose children needed follow-up health checkups and those whose children did not.
Results:
The study included 114 participants, with 55 in the intervention group and 59 in the control group. Analysis revealed that 29.1% of the intervention group adhered to 2 recommended parenting techniques, compared with 24.6% in the control group. However, no significant differences were observed between the intervention and control groups in adherence to 2 recommended techniques versus one or none, or to any single technique among the 3. Subgroup analyses revealed significant differences in adherence among parents whose children were identified to have developmental concerns at the 1.5-year health checkup and were required to have follow-up checkups, specifically in the “avoid immediate reactions” approach between intervention and control groups.
Conclusions:
The PT pamphlets effectively increased adherence to recommended parenting techniques in the intervention group among children requiring follow-ups. This underscores the importance of culturally adapted PT programs and demonstrates the potential of simple educational interventions in improving parenting styles.
Introduction
The health care campaign “Sukoyaka Oyako 21,” meaning “healthy parents and children 21,” has played a critical role in Japan’s vision for family health. 1 The first phase was characterized by being based on a life-stage approach and including quality-of-life and mental health indicators with regard to delivery and parenting. This phase aimed to build a positive family environment. The second phase of the initiative was rooted in a community-based approach 2 and focused on supporting parents who experience difficulties in raising children, aiming for 95% of parents being able to cope when facing such difficulties. 1 The second phase was succeeded by a new policy under the Children and Family Agency Establishment Act enacted in 2023. It continues to focus on preventing parenting difficulties and providing mental health support for children and parents.
In Japan, studies indicate that experiencing difficulties in raising children is a common aspect of parenthood.3,4 Such challenges are often attributed to children’s negative emotional outbursts. Mothers tend to encounter frustration in response to these parenting hurdles, potentially leading to maladaptive coping mechanisms. Research has shown that parenting behaviors significantly affect the parent-child relationship by creating environmental contexts that can influence emotional development. This intricate dynamic represents one of the key difficulties in raising children and reflects the mental and emotional burdens borne by parents, which can occasionally lead to experiential avoidance and overcontrol.5,6 These, in turn, may contribute to the development of behavioral problems in children, thus fueling a destructive pattern. 5
Parent training (PT), as recommended by the Children and Family Agency, offers programs to help parents manage child-rearing challenges and improve their children’s behavior. The programs focus on identifying and praising positive aspects in children. They categorize behavior into 3 types: favorable, unfavorable, and inexcusable, while examining behavior by analyzing triggers, the behavior itself, and its consequences. Effective parenting techniques include praising favorable behavior, systematically ignoring unfavorable behavior, and adjusting the environment with clear instructions to support positive outcomes. This training is especially advantageous for parents dealing with behavioral issues in children, such as Attention Deficit Hyperactivity Disorder and other developmental disorders. 7 PT emphasizes teaching effective strategies and skills to improve parenting techniques, encourage positive behavior, and more effectively handle challenging behaviors. 8 Supported by research, PT is recognized as an effective intervention that benefits both child behavior and the parent-child relationship.9-11 Recommended as a primary treatment option, PT programs are diverse, ranging from individual or group sessions with therapists to flexible online courses that parents can undertake at their convenience. One example of a commonly implemented program in Japan is the “Triple P” Positive Parenting Program, which was imported from Australia.9,12 It is based on an ecological approach and can be tailored to parenting in different social contexts. The typical content of Triple P in Japan includes not only practical strategies for encouraging desirable behavior in children and managing misbehaviors, but also self-care for parents.
The effectiveness of PT programs in Japan has been demonstrated through various studies, showing that PT is not only associated with enhanced parenting practices and reduced parenting stress but also improves communication skills in children.13,14 These studies, along with comparative studies worldwide, suggest that tailoring PT programs to specific cultural contexts can maximize their effectiveness.13-16 These conclusions contributed, among other things, to the 2016 amendment of the Act on Support for Persons with Developmental Disabilities. This amendment strengthened commitments to family support and led the Japanese Ministry of Health, Labour and Welfare to actively promote the widespread implementation of PT programs. 17 This initiative is part of a broader effort to develop a comprehensive support system for individuals with developmental disabilities.
In Shioya Town, Tochigi Prefecture, Japan, health counseling services are provided for 5-year-old children aimed at the early detection of developmental disabilities. 18 This proactive initiative identifies and promptly addresses potential developmental challenges, thereby increasing the likelihood of effective intervention and support. Notably, over half of these children were found to need further observation, detailed examination, or medical intervention. 18 Consequently, PT is utilized and recommended as a critical approach in child health assessments to manage developmental disabilities effectively. 19 A baseline survey 19 was conducted to explore parents’ differing experiences and coping strategies in Shioya Town. This survey revealed that the use of PT techniques such as “conscious response” was less prevalent among parents of 3.5-half-year-olds than those of younger children. However, the parents of the older children who utilized PT techniques reported experiencing fewer difficulties in raising their children. This suggests that difficulty using effective PT techniques increases with the child’s age. 19 Taking the study as a basis, the researchers of the present study, in collaboration with public health nurses in Shioya Town, developed a PT pamphlet featuring 4 typical scenarios of challenging behaviors and guidance on suitable parenting responses. It recommends 3 different parenting techniques: “avoid immediate attention,” which encourages parents to avoid immediately paying their child attention in a way that rewards difficult behavior; “avoid immediate reactions,” which advises parents to take a moment to think before responding to their child’s troublesome behavior rather than reacting impulsively; and “conscious response,” which focuses on the importance of parents responding deliberately and thoughtfully to troublesome behaviors.
The study aims to evaluate the effectiveness of the PT pamphlet distributed in Shioya Town since 2019. The study compares 2 groups: 1 that received the pamphlet (intervention group) and 1 that did not (control group). Our hypothesis was that the intervention group would show greater improvement in adopting recommended parenting behaviors than the control group. The primary focus of our analysis was on measuring and comparing the degree of adherence to the parental techniques recommended in the pamphlet between the 2 groups. Additionally, focusing on subgroups of parents whose children were or were not required to have follow-up health checkups, the study compares adherence to each recommended parental technique between the intervention and control groups within each subgroup.
Methods
Procedure and Participants
The study employed a non-randomized intervention design with historical controls. It was conducted in Shioya Town, Tochigi Prefecture, Japan, from June 2019 to December 2022. Among the 155 parents who attended the health checkups of their 3.5-half-year-old children during this period, only those parents for whom there were records of their children’s attendance at 1.5-year health checkups were included as participants in the study (N = 114).
As shown in Figure 1, the intervention group comprised 55 parents of children who underwent health examinations at the age of 3.5-half years between June 2021 and December 2022. Members of this group received a PT pamphlet at their child’s 1.5-year health checkup. In contrast, the control group consisted of 59 parents of children who also underwent health examinations at the age of 3.5-half years between June 2019 and March 2021. Members of this group did not receive any PT pamphlet at their child’s 1.5-year health checkup.

Summary of study procedure.
Following the 1.5-year health checkups, parents of 29 children from the intervention group and parents of 22 children from the control group were instructed to bring their children for additional follow-up checkups as a result of an assessment of the child’s development. Before all children in both groups returned for their 3.5-half-year checkup, all parents received questionnaires along with the regular health checkup information packet. These questionnaires were self-administered, anonymous, and collected at the health checkup site, which was administered at a single location.
Creation of the PT Pamphlet
Municipal public health nurses and the first author engaged in iterative discussions to refine the structure and usability of the pamphlet, ensuring it was easily comprehensible and practical for parents. Illustrations crafted by co-author (Yokoyama)and featured in “Shogakukan 2nd Grade,” an educational magazine for elementary school children, were incorporated into the pamphlet, following consultations with public health nurses. The content was tailored with the following 3 objectives in mind: (1) Presenting concrete and actionable methods; (2) Ensuring accessibility for mothers and fostering an engaging reading experience; and (3) Demonstrating PT techniques through relatable examples.
The pamphlet was designed as a full-color A4 double-fold format, comprising a front cover, facing page, and back cover. Manga illustrations used in our tool are Japanese comic art that combine visualization and storytelling, and have been used in various health education in and outside Japan.20,21 In our tool, 4 common scenarios of troublesome behavior were illustrated alongside explanations of PT methods. These scenarios were based on stories about difficult parenting situations that the nurses commonly heard from parents. The depicted problematic behaviors comprised: (1) “Won’t stop saying no,” (2) “Running around,” (3) “Won’t tidy up,” and (4) “Doesn’t listen.” Additionally, the last page featured a concise overview of parenting techniques under the title “Practicing words of praise.” An excerpt from the PT pamphlet, covering the first of these problem behaviors, is shown in Figure 2.
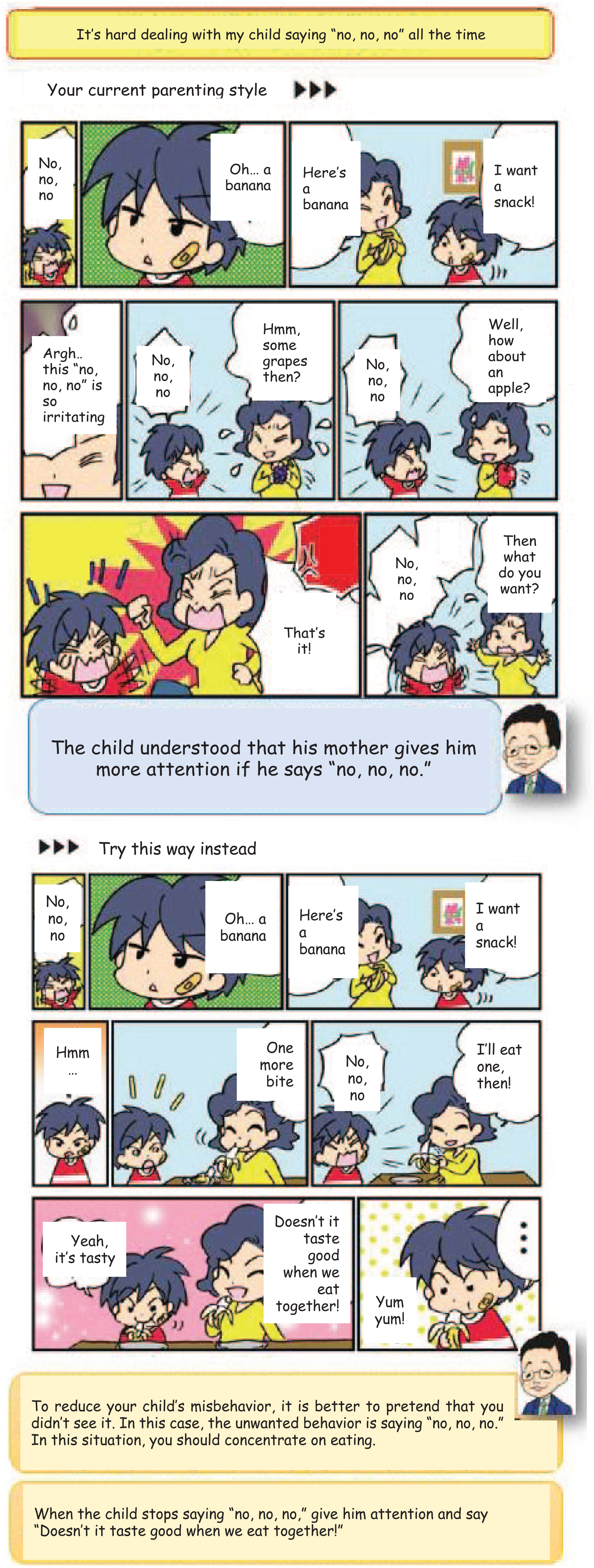
Pamphlet sample pages.
Measures
Parenting techniques used: We asked participants about situations that parents commonly find difficult to deal with using a modified version of the “Observation of Children’s Behavior—Home Situation Version” questionnaire developed by Tomizawa and Yokoyama, 22 whose results were reported previously. 19 The present study aimed to gauge parental self-awareness of their responses to these troublesome behaviors exhibited by their children, which elicit feelings of concern and irritation, prompting the desire to mitigate such behaviors. The following 3 specific questions that align with the PT instructions were presented to parents, with responses rated on a 4-point Likert scale (“frequently,” “occasionally,” “rarely,” and “never”). 19
Avoid immediate attention: Examining how often parents attend to troublesome behaviors when they arise (question: “Do you pay immediate attention when troublesome behavior occurs?”).
2. Avoid immediate reactions: Assessing how often parents consciously refrain from reacting immediately and instead respond thoughtfully when confronted with their child’s troublesome behavior (question: “Do you refrain from reacting immediately when your child exhibits troublesome behavior?”).
3. Conscious response: Exploring how frequently parents consciously respond when engaging with troublesome behavior (question: “Do you consciously respond when engaging with troublesome behavior?”).
Scores for this scale were calculated with reference to the methodology outlined by its developers. For each technique, responses were divided into 2 categories: “adhered” and “did not adhere.” Responses indicating “frequently” or “occasionally” were classified as adherent, while those indicating “rarely” or “never” were considered non-adherent. Because the structural nature of the first question (“avoid immediate attention”) was inverted, the response ratings were reversed.
Sociodemographic characteristics: The sociodemographic questionnaire encompassed inquiries regarding the parent, relationship to the child (father, mother), employment status (yes, no), subjective health assessment (poor, good), spouse’s employment status (yes, no), and subjective health assessment of the spouse (poor, good).
Additionally, data were gathered from each child handbook (a copy of which is held in the healthcare center in Shioya Town) regarding the child’s gender, gestational age at birth (less than 37 weeks, 37 weeks or more), and birth weight (less than 2500 g, 2500 g or more).
Ethical Considerations
This study was conducted with the approval of the Ethics Committee of Fukushima Medical University (2021-176). Participation in the questionnaire was voluntary, and individuals were assured that their participation would not result in any disadvantage. Furthermore, the anonymous questionnaire ensured that individuals could not be identified.
Data Analysis
All data were coded and analyzed using IBM SPSS Statistics, Version 28. Descriptive statistics were employed to outline participants’ characteristics and key variables. The chi-square test or Fisher’s exact probability test was conducted to assess variances between the intervention group and control group across sociodemographic characteristics (Table 1), adherence to 2 recommended parenting techniques versus adherence to one or none (Figure 3), and for comparing adherence to all 3 techniques (in Table 2). Statistically significant P-values were defined as those less than .05. All responses were accounted for, and items with no response were treated as missing values.
Participants’ Sociodemographic Characteristics, by Group.
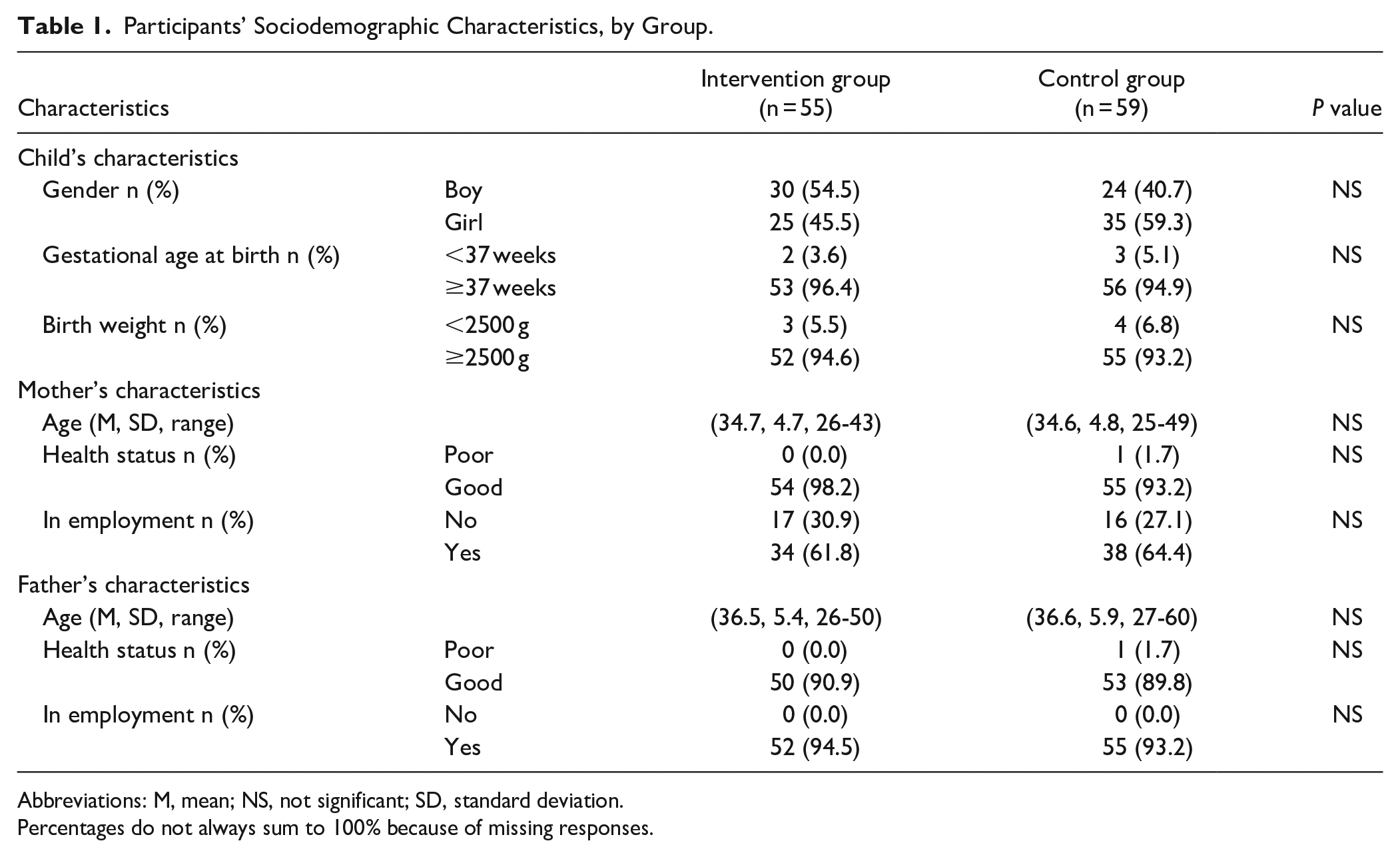
Abbreviations: M, mean; NS, not significant; SD, standard deviation.
Percentages do not always sum to 100% because of missing responses.

Degree of adherence to recommended parenting techniques, by group.
Comparison of Adherence to Each Recommended Parenting Technique Between Intervention and Control Groups, Stratified by the Necessity of Follow-up Health Checkups.

Abbreviation: NS, not significant.
Proportions were calculated without missing values.
Results
Participants’ Characteristics
The characteristics of the participants are shown in Table 1. The total study sample was 114 participants. Mothers completed the questionnaires in all cases except 2, where the child’s father was the respondent. Examining the characteristics of the participants’ children, in the intervention group where the pamphlet was provided, 54.5% were male, with the majority born at more than 37 weeks’ gestation and weighing over 2500 g at birth. Conversely, in the control group, over half of the participants’ children were female, yet they exhibited comparable characteristics to those in the intervention group regarding gestational age and birth weight.
Among the mothers, the average age was 34.7 years, ranging from 25 to 49 years. All mothers in both the intervention and control groups reported good health except for 1 participant in the control group. Nearly half of the mothers in each group were in employment. Regarding the fathers, the average age was 36.5 years, ranging from 26 to 60 years. Similar characteristics were observed in terms of health conditions among the fathers as among the mothers, with all fathers in both groups being employed. No statistically significant differences were observed in any of the characteristics between the intervention and control groups.
Adherence to 2 Recommended Parenting Techniques versus One or None
Figure 3 illustrates the degree of adherence to recommended parenting techniques in 3 segments for comparison. Segment 1, “All participants,” reveals that within the entire intervention group, 29.1% of participants adhered to 2 recommended parenting techniques outlined in the pamphlet, while 70.9% followed either one recommendation or none. Similarly, in the entire control group, 24.6% of participants adhered to 2 recommended parenting techniques, with 75.4% adhering to one or none. No significant differences were observed between the 2 groups regarding adherence rates.
Segment 2, “No follow-up,” offers insights into participants from the intervention group whose children were not required to attend follow-up checkups after the 1.5-year examination. In this subgroup, 19.2% adhered to 2 recommended parenting techniques, and 80.8% followed one or none. In contrast, for the control group without follow-up checkups, 34.3% adhered to 2 parenting techniques, and 65.7% followed one or none. Here, no significant differences were detected between the 2 groups.
The final segment, “Follow-up required,” details the adherence among participants from the intervention group whose children were required to have follow-up checkups after their 1.5-half-year examination. Of these, 37.9% adhered to 2 recommended parenting techniques, while 62.1% followed one or none. On the other hand, in the control group requiring follow-up checkups, only 9.1% adhered to 2 parenting techniques, with 90.9% following one or none. This comparison revealed significant differences in adherence rates between the 2 groups, with χ2 = 2.50 (P = .025).
Adherence to Specific Recommended Parenting Techniques
The study compared the intervention group (n = 55) with the control group (n = 59) across 3 recommended parenting techniques, with additional insights from subgroups differentiated by their child’s need for a follow-up checkup. Nearly all participants in both groups did not demonstrate adherence to the “avoid immediate attention” technique, with 5.5% adherence in the intervention group and 0% adherence in the control group. This pattern of low adherence was consistent, irrespective of whether follow-up checkups were needed, indicating no significant differences by group. There was a marginal difference in adherence for the “avoid immediate reactions” approach. In the intervention group, 29.1% adhered to the recommendation, while the control group showed 26.3% adherence. Notably, in the subgroup requiring follow-up checkups, the intervention group’s adherence rate was 34.5%, which exceeded that of the control group at 9.1%, with a P-value of .04. This finding suggests a significant underlying difference that warrants further examination. Reported adherence to the “conscious response” technique was relatively high in both groups, with 92.7% adherence in the intervention group and 98.3% in the control group, and no significant differences emerged within the subgroups.
Discussion
The primary objective of this study was to pilot test an intervention devised and implemented by the research team. Although the differences were not statistically significant and further study is warranted, parents in the intervention group (who received the PT pamphlet during their child’s 1.5-year health checkup) demonstrated higher adherence to 2 of the recommended parenting techniques than those in the control group (who did not receive the pamphlet). Notably, stratified analyses of children who were identified as having development concerns at 1.5-year health checkup and were required to attend follow-up health checkups and those who were not showed a striking contrast. In the subgroup of parents whose children were required to have follow-up checkups, adherence to 2 recommended parenting techniques was significantly higher in the intervention group than in the control group.
Of note, the characteristics of the study participants did not differ significantly from those reported in national-level health statistics: according to the Ministry of Health, Labour and Welfare’s summary of birth statistics for the fiscal year 2021, 4.7% of babies were born at less than 37 weeks, and 9.0% had a birth weight less than 2500 g. Additionally, the findings related to the baseline characteristics were detailed in a previous report, 19 and using these data, we found that there was no significant difference between the intervention and control groups in the proportion of parents reporting parenting difficulties or a lack of knowledge about how to deal with these difficulties.
The marked difference between the intervention and control groups among children who were required to attend follow-ups warrants particular attention, particularly given that the “Sukoyaka Oyako 21” national maternal and child health plan seeks to enhance the proportion of parents who are equipped to cope when confronted with parenting challenges. The reported percentage in 2021 was 81%, whereas the plan aims to achieve 95%. 1 Our observed increased adherence may indicate the potential of the PT pamphlet being a relatable and understandable tool for recommending PT strategies in contexts where children face developmental or health challenges that necessitate follow-up checkups. Typically, parenting programs targeting parents of children with various difficulties tend to yield more effective results when comparing before and after the intervention or when comparing intervention groups to control groups.23,24 This may be because parents of children facing certain challenges are more responsive to targeted intervention programs. Another possible explanation for our results is that increased interaction with healthcare professionals during the follow-up checkups may have enhanced the parents’ engagement and responsiveness to the intervention.
Conversely, for parents whose children did not require follow-up checkups after the 1.5-year health checkup, the adherence rates to 2 recommended parenting techniques were lower in the intervention group than in the control group, but not significantly so. This suggests that the intervention may yield equal outcomes across all parent segments with low perceived needs. Similarly, a previous systematic review indicated that mindfulness-related PT programs can produce comparable outcomes for parents in both intervention and control groups when there is no expressed need for support. 25
To further assess the intervention’s effectiveness, we separately analyzed the 3 parenting techniques recommended in the PT pamphlet. This analysis was conducted both within and between the intervention and control groups, as well as among different subgroups, particularly comparing those required to attend follow-up health checkups with those who were not. For the “avoid immediate attention” and “conscious response” techniques, no significant differences were observed either between the intervention and control groups in general or within the subgroups defined by follow-up checkup requirements. However, for the “avoid immediate reactions” technique, significant differences were found only among parents who attended follow-up health checkups. Generally, it is indeed challenging for parents not to react immediately to problematic behaviors in their children. 24 Research suggests that effective parenting often involves managing the urge to respond hastily and instead using strategies that focus on long-term behavior modification rather than immediate correction. Therefore, many recommendations and techniques, such as “active ignoring,” which involves parents intentionally withdrawing attention for minor misbehaviors, have been developed to help parents overcome the challenge of reacting immediately to their children’s problematic behaviors. 26
Limitations and Recommendations for Future Studies
This study has several limitations. The study included only a limited number of parents in both the intervention and control groups. Estimated power for a 2-sample proportions test for the significant item in Table 2 was 0.5894, suggesting that it may not be sufficient for making a robust conclusion. Furthermore, it was conducted in a single geographical area and utilized a historical control method. We lacked the baseline 1.5 year data on parenting behavior for the control group, but we included parents of all children who attended 3.5-half-year health checkups and considered it unlikely that significant demographic changes would occur during the short study period. We thus assumed that the background information of the intervention and control groups was comparable. However, to thoroughly examine the effectiveness of the intervention, future studies should involve a larger sample of parents across diverse geographical areas and employ a randomized controlled trial design. Additionally, it is recommended that follow-up studies explore the effectiveness of the intervention among different subgroups by assessing various variables that may affect parents’ adherence to the recommended parenting techniques.
Implications and Conclusions
This study in Shioya Town pilot tested a PT pamphlet, revealing its potential to improve parenting approaches for raising children. The PT pamphlet showed potential to be particularly effective for parents whose children needed follow-up examinations, underscoring the importance of supporting parents facing challenges. A similar initiative was taken at another health center in Japan. They distributed a pamphlet addressing parental concerns about their children’s development and confirmed that parents recognized the health center as a place for consultation. 27 Overall, our research and existing evidence indicate that the PT pamphlet successfully aligns with and contributes to parenting support policy, which aims to help parents manage the difficulties of raising children.
Furthermore, our research underscores the significance of creating support materials that are not only informative but also accessible, engaging, and tailored to parental needs. The PT pamphlet’s design, which included clear instructions and relatable scenarios, likely played a crucial role in enhancing parent engagement. This emphasizes the value of investing in high-quality, visually appealing educational content that is easy for the target audience to understand. 28
This study shows that the effectiveness of parental interventions often depends on the context and varies according to different variables. It highlights the importance of tailored PT programs as crucial tools for supporting parents. Although this research was conducted in Japan, there is significant potential for adapting the PT pamphlet for use in other regions, considering social, cultural, and linguistic differences.
Footnotes
Acknowledgements
The authors wish to thank the public health nurses who participated in the leaflet distribution and data collection. The authors also thank Oliver Stanyon for editing this manuscript.
Correction (April 2025):
Figure 3 has been updated since the original online publication.
Authors Contribution
Akutsu and Yokoyama designed the study and Yokoyama developed the leaflet. Akutsu managed and analyzed the data. Akutsu and Goto designed the analyses and interpreted the results. Abo-Rass advised on the data interpretation and edited the draft. All authors were involved in finalizing the manuscript and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This was supported in part by a departmental grant at Fukushima Medical University
IRB Approval
This study was approved by the Ethics Committee of Fukushima Medical University (2021-176 and 30156).