
Abstract
Introduction:
People in rural regions frequently lack resources for mental health support. Changing Our Mental and Emotional Trajectory (COMET) is a universal, community-based program designed to address mental and emotional health issues early and prevent crises. COMET Community Training is a short, interactive training that teaches people how to initiate a supportive and potentially emotional conversation using the simple, 7-item COMET Conversational Gravity Assist. This article describes and reports on the feasibility and acceptability of COMET and its Community Training.
Methods:
COMET was developed using a participatory research approach by community members and health professionals living in a rural region and their research partners. COMET Community Trainings were conducted over a 22-month period. Surveys were administered to attendees before and after training to describe attendees’ characteristics, view on content, and impact on intention to use COMET components. Field notes were completed by trainers to document the date and number of attendees.
Results:
Over 700 people attended 60 Community Trainings. Questionnaires were completed by 644 trainees before and 580 after training. Of pre-survey respondents, 25% worked in education and 15% in farming/ranching. Post-survey respondents were 62% female, and 32% were between age 18 and 36. High levels of training satisfaction were reported. Average likelihood of using items in the COMET conversational guide increased significantly from pre to post training. On a scale of 1 to 10, nearly 80% of respondents rated their likelihood of using COMET in the next 3 months a 7 or higher.
Conclusions:
COMET Community Training is a feasible program that effectively reaches a range of community members and improves the likelihood that they will initiate conversations when concerned about someone else’s mental health. Results lay the groundwork for COMET as an intervention that promotes mental and emotional well-being to address inequality in mental health for people living in rural communities.
Purpose
More than 20% of American adults suffer from a diagnosed mental illness. 1 An additional 25% of the population suffers from psychological and emotional distress that does not meet clinical diagnostic criteria. 2 Undiagnosed and under-treated mental illness or psychologic distress results in significant morbidity, early mortality, missed days of work, lower productivity at work, and missed school days. 3 People living in rural communities typically have access to fewer resources for mental health and emotional health support than their urban counterparts. Over 65% of Mental Health Professional Shortage Areas in the United States are in rural areas, 4 and non-metropolitan counties have many fewer mental health providers per capita compared to metropolitan counties. 5 Access to these scarce health professionals is often hampered by travel barriers, insurance issues, and stigma and shame in rural communities. 6 Community-based programs striving to help address these gaps often focus on the person experiencing the problem, often a crisis such as suicidal thoughts or psychosis. 7 Faced with these realities and concerned about increased farming stress, depression and anxiety, and suicides in rural eastern Colorado, the High Plains Research Network (HPRN) Community Advisory Council (C.A.C.) used a community-based participatory approach to create an intervention called Changing Our Mental and Emotional Trajectory (COMET) to help community members acknowledge and address concerns about another person’s mental and emotional health in everyday settings and interactions.
The HPRN works with communities and primary care practices in 16 rural counties of eastern Colorado, as designated by the Office of Management and Budget and the US Department of Agriculture. 8 The HPRN C.A.C. was formed in 2003 and is a grassroots group of farmers/ranchers, teachers, small business managers, students, and retirees living in rural eastern Colorado.9,10 The C.A.C. conducted a rigorous 18-month exploration of mental health in their communities and identified access to support that prevents mental health problems as a priority health issue and gap in care in critical need of attention. We note here that the C.A.C. chose to use the term mental and emotional health rather than behavioral health as it is a more understood term in the community.
Given the scant evidence for how community members can successfully access mental health care, the HPRN C.A.C. used an Appreciative Inquiry (AI) approach11 -14 to study what worked for local community members to access mental health care and support. The AI process revealed the concept of the “other person”—usually not a spouse, partner, or health professional—who noticed another person’s need, initiated a conversation (sometimes multiple times), and provided support, including emotional support and, in some cases, helped make phone calls or provided transportation to some type of care. Conversations often occurred in regular community gathering places such as homes, golf courses, fields, sporting events, and parking lots. The C.A.C. defined these non-clinical settings as “safe venues” for emotional expression. The Boot Camp Translation (BCT) process was used to translate these AI data into the culturally relevant, actionable COMET program. BCT is an evidence-based method to engage community members and academic researchers in a process of translating complex medical jargon and clinical guidelines into locally relevant actionable messages and materials for community and practice interventions.15 -20 A thorough description of the development process is described elsewhere.21,22
The resulting COMET program taps into the rural cultural value of neighbor helping neighbor and aims to provide community members with the language, tools, and confidence to intervene when they notice someone around them is unwell—before a crisis occurs. Designed for older youth and adults, the intervention takes a universal approach to prevention rather than focusing on a single mental health condition or demographic. COMET addresses fear of engagement in potentially emotional conversations by teaching lay community members to initiate a supportive interaction when they encounter someone who is in a mental or emotional “vulnerable space.” COMET does not expect “the other person” to solve a complex problem but to be actively present. The goal is to start a shift in the person’s mental health trajectory back to a place of wellness instead of proceeding toward crisis. See Figure 1.
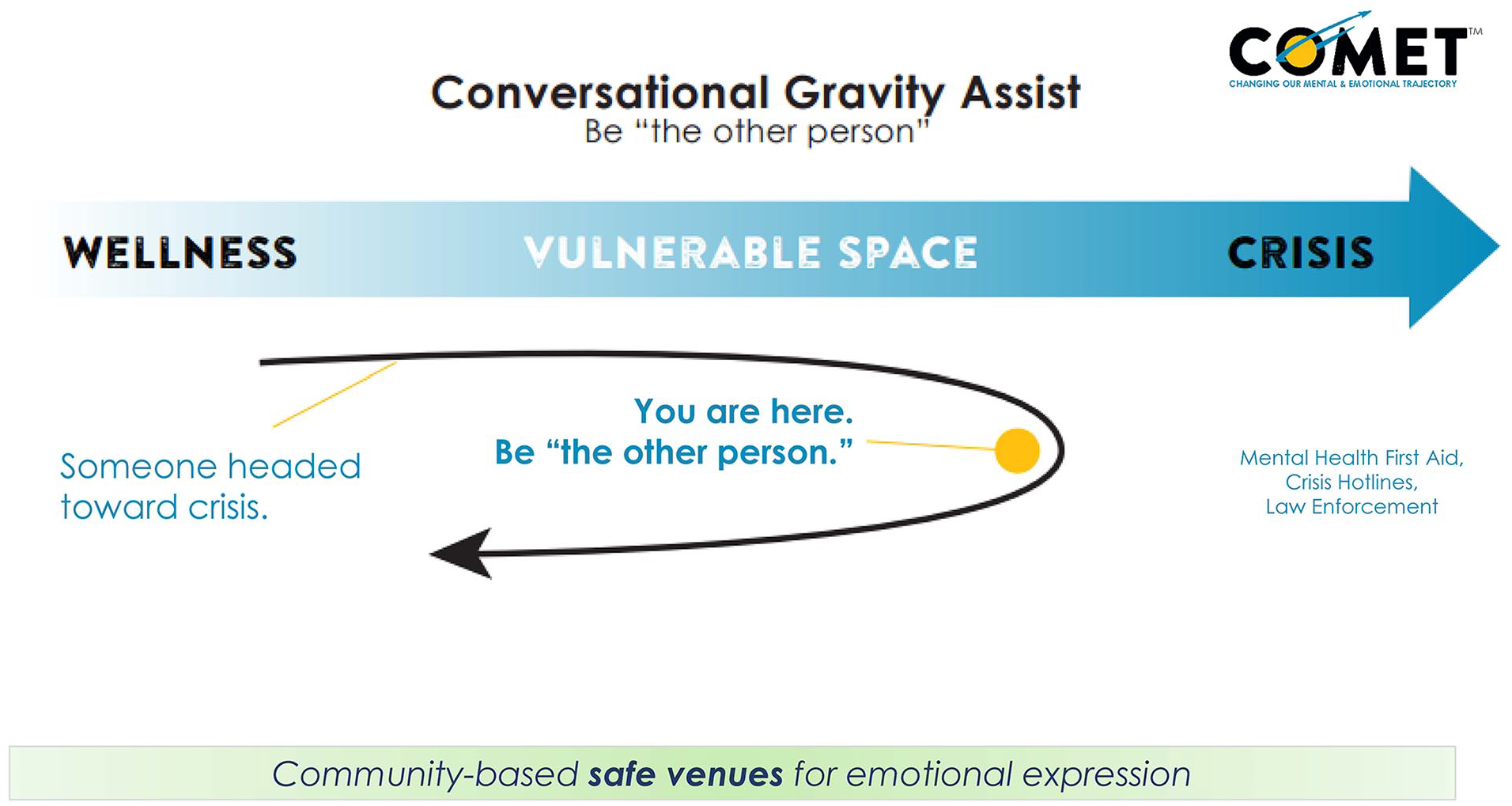
COMET conversational gravity assist model.
The program is anchored in the C.A.C.-named Conversational Gravity Assist Model, which consists of 7 simple, conversational components. See Table 1. Specific questions and statements for each of the 7 components further guide these conversations and reflect the AI data and the lived experience of rural community members.
The COMET Questions and Statements.

To mirror the Patient Health Questionnaire (PHQ) used in clinical settings, the HPRN C.A.C. initially called the COMET components the “Conversational PHQ” but were worried about copyright infringement. The group realized that “the other person” was present for their peer at the right time and place. The idea that the presence of something can redirect the trajectory of another object to a more desirable position is similar to the concept of a “gravity assist” orbital maneuver used in space exploration, 23 which led to the Conversational Gravity Assist name.
COMET is disseminated through a 2-h COMET Community Training course. COMET Community Training is designed for a broad community of older youth and adults. The training curriculum pulls from the evidence-based techniques of using lay educators, mindfulness, and motivational interviewing.24 -29 Experiential and didactic sections cover a range of mental and emotional health problems, examples of when participants have been “the other person,” and a thorough review of the COMET questions. Participants practice having conversations that incorporate the COMET questions using scenarios tailored to the local region, receive feedback, and share action plans. The training includes a discussion of local resources to which a person could be referred. Materials include a comprehensive companion script for trainers. A member of the C.A.C. with 25 years of experience developing learning curricula and college instruction led the development of the curriculum, in collaboration with mental and public health professionals, researchers, and other C.A.C. members. Materials are available in English and Spanish.
Almost any organization, social club, professional group, friends circle, or business can host a training. The training can be delivered in-person in a wide range of settings or virtually and is conducted by a certified, 2-person team that intentionally includes non-clinical mental health care providers, which the C.A.C. posited could appeal to a range of community members.
The purpose of this article is to describe COMET and its Community Training and report on the initial assessment of the training feasibility and acceptability.
Methods
This work was conducted to assess the feasibility and acceptability of COMET and the Community Training, constructs particularly relevant to early intervention evaluation.30 -32 The C.A.C. asked: Can we conduct trainings? Will anyone come? Who will come? What will they think of COMET and the training? Feasibility was measured by the number of trainings, attendee numbers, and delivery mode (virtual or in-person), which were recorded by the COMET trainers in a field note for each session. Attendee characteristics were collected via survey (described below). Acceptability was measured by trainees’ view of content, recommendation of training, and initial impact on intention to use COMET.
Self-report surveys were distributed to training attendees before and after training. The pre-training survey collected occupation and training in Mental Health First Aid. The post-training survey collected age, sex, view of amount of content, and intention to use COMET overall. Pre- and post-training surveys included repeated measures on participants’ likelihood of using specific COMET components. Pre- and post-trainings surveys were not linked. The survey was administered via paper copy or a link to REDCap.33,34
Descriptive statistics (mean, standard deviation, frequencies) were computed for participant characteristics (race, ethnicity, age, position type, sex, education), program satisfaction, and survey responses. Since surveys were not linked, unmatched t-tests were used to compare individual pre- and post-training mean scores for 4 evaluation (Likert scale) items on the likelihood of using specific COMET conversational questions. Likert scale responses for the likelihood to use COMET questions ranged from 1 (Not at all likely) to 5 (Very likely). Independent sample t-tests were also conducted with post-training survey data to analyze likelihood to use COMET in the next 3 months (on a scale of 1-10) by respondent age and sex. P values are reported, and all analyses were performed using SAS 9.4. The Colorado Multiple Institutional Review Board reviewed the evaluation protocol and determined it qualified as a program evaluation and was not human subjects research.
Results
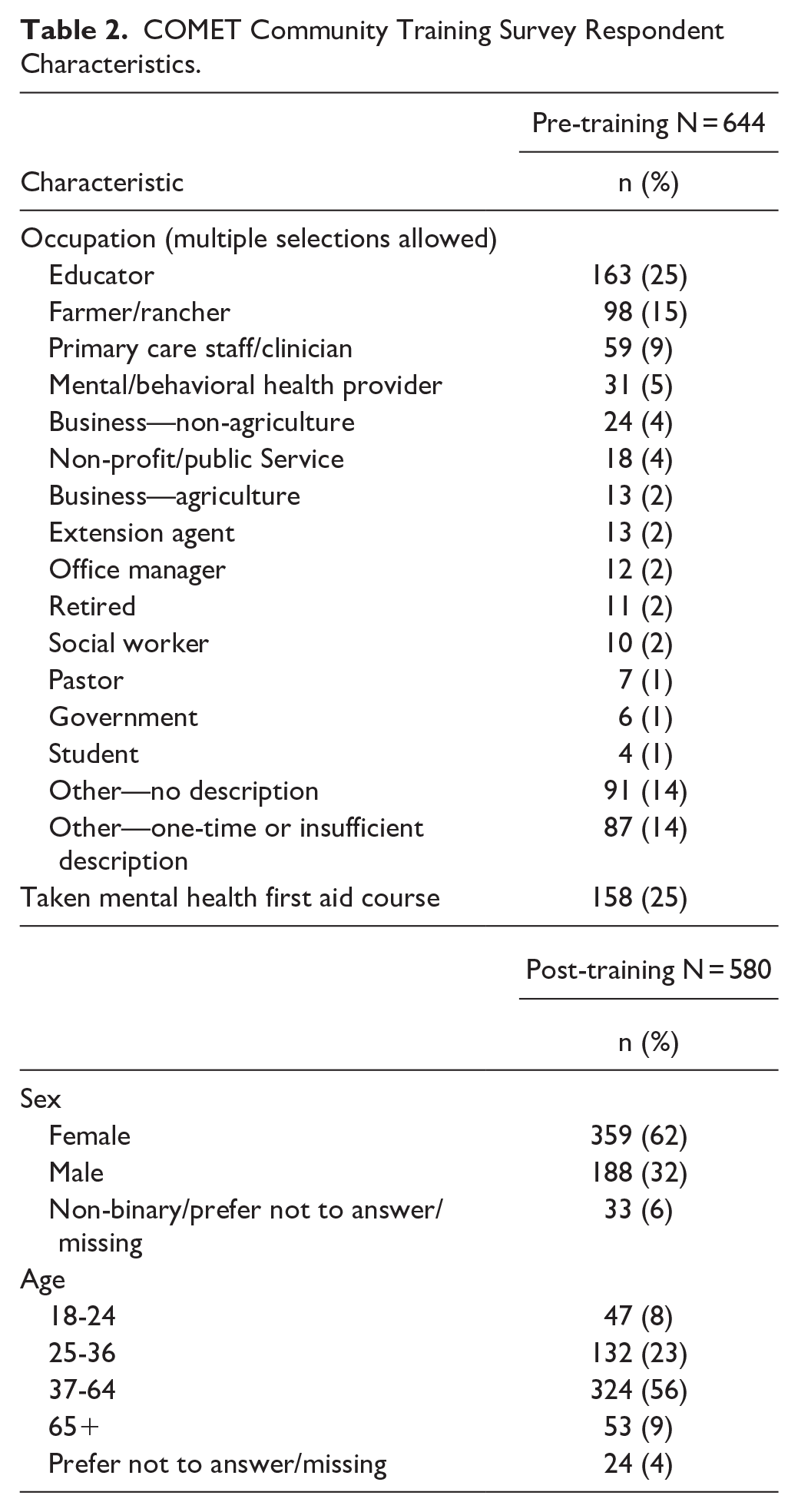
The COMET Community Training was conducted 60 times during this evaluation period (January 2021–October 2022). Of these, 42 were conducted in-person and 18 virtually. Trainings were attended by 707 people. Attendance ranged from 1 to 60 people, with an average of 12. The evaluation survey was completed by 644 participants before training and 580 participants after training. Table 2 shows the respondents’ characteristics. Respondents reported a wide range of occupations. Most common were educators (25%), farmer/rancher (15%), and primary care (9%). A quarter (25%) of pre-training survey respondents reported taking the Mental Health First Aid course. Nearly 62% of respondents were female, and 31% were between 18 and 36 years old.
COMET Community Training Survey Respondent Characteristics.
High levels of satisfaction with the training were reported. Ninety-five percent of respondents reported that the amount of information provided was just right. Nearly 94% agreed or strongly agreed that the training provided resources that can help them use COMET successfully, and 92% agreed or strongly agreed that they would recommend the training to others.
Overall, respondents rated their likelihood of using specific COMET questions higher after training than before across all measures. Table 3 shows reductions in the “not very likely” and “somewhat likely” categories and increases in “likely” and “very likely” categories. The percent of respondents reporting that they are likely or very likely to ask someone how they are really doing increased from 69% to 84% after training, to comment on an observed change in mood or behavior increased from 45% to 76%, to invite family or friends to talk more about a potentially emotional situation increased from 62% to 81%, and to invite an acquaintance increased from 47% to 77%. After training, the percent reporting being not at all likely to engage in these COMET behaviors was zero or nearly zero. The average level of likelihood increased significantly from pre to post training for each of the questions assessed. See Table 3.
Likelihood of Using Specific COMET Questions Before and After COMET Community Training Among Survey Respondents.

When asked how likely they were to use COMET in the next 3 months on a scale of 1 to 10, 78% reported a 7 or higher, and 30% reported a 10. Average likelihood of using COMET in the next 3 months differed between males and females (men = 7.5, women = 8.4, P < .0001). However, no significant differences by age group were found (age 18-24 = 7.5, age 25-36 = 8.2, age 37-64 = 8.2, age ≥ 65 = 7.9).
Discussion
In many rural regions, challenges to attract and retain mental health care professionals persist, and seeking care from the existing workforce remains frustratingly stigmatized. Many people suffer from distress, moderate depression, anxiety, or some combination for which they do not seek professional care but that significantly impacts their health and well-being and could develop into more a serious or persistent problem if unaddressed. Results of this evaluation demonstrate feasibility and acceptability of the COMET program, a new intervention designed to help community members prevent mental and emotional health crisis in rural regions. These results are timely as demand for the COMET Community Training is growing. Depression and anxiety reportedly increased 25% globally during the first year of the COVID-19 pandemic, 35 and the mental strain caused by financial hardships and farm stress resulting from severe drought in agricultural communities cannot be overstated. With primary care physicians providing 45% of visits to patients with depression and/or anxiety, 36 requests from rural practices for COMET training are increasing as practice staff need additional tools to support their use of screening protocols and brief interventions. This report is an important first step to answer questions about community response to and initial impact of COMET.37,38
The number of trainings and attendees and participant characteristics suggest that the COMET Community Training is a feasible method to reach and teach a broad group of community members about COMET. Trainings were attended by people across age groups and sex. The range of occupations reported suggests that COMET can reach community members from many walks of life, as designed. The ability to reach the farming and ranching community is particularly important as suicide rates in rural areas are substantially higher than in urban communities, especially for older males. 39
COMET complements programs that focus on crisis and immediate suicide risk, such as Mental Health First Aid (MHFA). 40 However, in the HPRN region, local MHFA classes are frequently canceled due to low enrollment. This led the C.A.C. to have lengthy discussions about the duration of the COMET training and amount of information to include. They decided to create a shorter training and focus on prevention. This structure appears acceptable as nearly all respondents indicated that the amount of information in the training was just right and that they would recommend the training to others.
Our statistically significant results support the acceptability of the COMET concept and suggest that training increases the likelihood that trainees will engage in a conversation about mental and emotional health when concerned about another person. The positive initial impact on attendees’ intentions to take action when someone is in a vulnerable space is important as change in behavior intention is associated with actual behavior change.41,42 Further, likelihood of using COMET scores of 7 or higher on a scale of 1 to 10 from both males and females are meaningful because they indicate high motivation for readiness to take action. 43 While this study does not report on the effectiveness of COMET, supportive conversations promote early intervention and treatment, which in turn improve health outcomes and lower cost.44 -47
Limitations include self-reported data, cross-sectional surveys, and the lack of health outcomes in COMET recipients. However, self-reported data are standard for this type of training evaluation. Linking of surveys was not a reasonable protocol, and fidelity could not be ensured. Assessing the impact on COMET recipients was beyond the scope of this evaluation but is a priority for future work.
Key next steps include refining program implementation and expanding our evaluation to include the impact on COMET recipients and the role of the program in reported health changes. The evaluation team is initiating a protocol to obtain training participants’ reports of using COMET up to 12 months post-training. The COMET Regional Trainer Workshop, which was developed to train, certify, and support individuals to deliver the Community Training in their local regions, and has been conducted in 11 states and will be further disseminated and evaluated to meet the demand for COMET. Current findings will be used to guide and inform these activities.
Conclusion
Changing Our Mental and Emotional Trajectory (COMET) aims to help people living in rural communities address mental and emotional health issues well before they become a crisis. This evaluation demonstrates the feasibility and acceptability of the COMET Community Training to reach a range of community members and improve the likelihood that they will engage in caring conversations with others when concerned about someone else’s mental and emotional health. These results lay the groundwork for COMET as an intervention that promotes mental and emotional well-being to address inequality in mental health for people living in rural communities.
Footnotes
Acknowledgements
The authors wish to acknowledge all other members of the High Plains Research Network Community Advisory Council who developed Changing Our Mental and Emotional Trajectory (COMET) to improve the mental and emotional health of people living in rural eastern Colorado: Lois Christiansen, Ashley Espinoza, Mike Hernandez, Ned Norman, Mary Rodriquez, Norah Sanchez, Sergio Sanchez, Kathy Winkelman, Steve Winkelman, and Liz Hickman. Thanks also to Hannah Bates, Chris Frakes, Maranda Miller, Chad Reznicek, and Clinton Wilson for their amazing work introducing COMET to people living in rural eastern Colorado and around the country.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Program development supported by the Patient Centered Outcomes Research Institute contract number ME-1303-5843. Contents are the authors’ sole responsibility and do not necessarily represent official views of the authors’ affiliated institutions or PCORI.
Ethical Considerations
The Colorado Multiple Institutional Review Board reviewed the evaluation protocol and determined it not human subjects research because it qualifies as a program evaluation.
Data Availability
Not applicable