
Abstract
Introduction/Objectives:
Since the COVID-19 pandemic, few studies have examined how participation in Supplemental Nutrition Assistance Program (SNAP) and/or Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) impacts diet quality in families with young children. This study aims to explore the association between SNAP and/or WIC participation and diet quality in mother-child dyads in Greater Boston, MA.
Methods:
A mixed-method approach involving cross-sectional surveys and in-depth interviews were utilized. Participants included 69 mother-child dyads for quantitative and 18 mothers for qualitative data collection. Analysis of covariance using generalized linear models was employed to compare differences in Healthy Eating Index-2015 (HEI-2015) scores based on SNAP and/or WIC participation, and thematic analysis was used for coding themes.
Results:
Mothers who participated in SNAP and/or WIC were more from lower socioeconomic backgrounds. After adjusting for age, race/ethnicity, and education, no significant differences in diet quality were found for both mothers and their children. However, qualitative results showed that mothers prioritized their children’s nutrition, used benefits to buy fruits and vegetables, and experienced stress that impacted their own diet quality.
Conclusions:
Since the pandemic, SNAP and WIC appeared to support families experiencing socioeconomic disadvantage (e.g., lower income and educational attainment) to improve diet quality, particularly through increased access to fruits and vegetables. However, these programs have not fully eliminated persistent disparities in diet quality, which seems to continue even the pandemic’s immediate effects have subsided.
Keywords
Introduction
Food insecurity—household-level economic and social condition of limited or uncertain access to adequate food 1 —has been shown to negatively impact dietary behaviors, leading to lower diet quality in adults and children, 2 especially in women, given their common roles in food production and preparation in families. 3 Challenges to achieve proper nutrition in families experiencing food insecurity may lead to increased risk of obesity and chronic diseases in families. 4 The prevalence of food insecurity in families with children was 12.5% in 2021, relatively consistent since the start of the Coronavirus Diseases 2019 (COVID-19) pandemic in the U.S. in 2020. 5 However, experiences of food insecurity are highly variable across the U.S. population, 6 as the risk of experiencing food insecurity is higher among families experiencing socioeconomic disadvantage—conditions of living that are less favorable socially and economically compared to others in society. Younger mothers and those with lower income and educational attainment often face greater socioeconomic challenges, which negatively influence dietary patterns and increase the reliance on food assistance programs. 7 Moreover, race/ethnicity is linked to disparities in food access due to systemic inequities and cultural differences in dietary habits, particularly among families of color, who are more likely to experience impacts of structural racism that unfavorably impact their access to resources and health. 8 Food insecurity may also drive parenting stress 9 and reductions in diet quality within families due to the affordability of energy-dense foods (likely high in sodium, saturated fat, and sugar, e.g., fast foods, sugar-sweetened beverages, etc.) versus nutrient-dense foods. 10
Furthermore, the recent COVID-19 pandemic worsened existing socioeconomic hardships including increases in employment income loss and housing instability, which further increased parenting stress, 11 and the risk and severity of food insecurity among families experiencing socioeconomic disadvantage before the pandemic. 12 The Pandemic Electronic Benefits Transfer (P-EBT) programs were introduced in Spring 2020 to temporarily address the additional challenges. However, how the programs were utilized has not been adequately studied. 13
In the U.S., the Supplemental Nutrition Assistance Program (SNAP) and Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) are 2 leading public health nutrition programs funded by the federal government to allow families experiencing low socioeconomic status to access quality and healthful foods, associated with reductions in food insecurity 14 and improvements in diet quality. 15 However, during the COVID-19 pandemic, despite federal efforts to increase participation, many families discontinued participating in SNAP and/or WIC due to difficulty recertifying benefits and virus exposure concerns. 16 Such discontinuation likely increased the risk of food insecurity and lowered diet quality in families experiencing socioeconomic disadvantages. 17
Since the COVID-19 pandemic, few studies have examined how SNAP and/or WIC participation impacts diet quality in families experiencing socioeconomic disadvantage, despite the increased importance of these programs during and after the pandemic, which disrupted food systems, strained household budgets, and exacerbated socioeconomic disparities, 12 likely making access to nutrition assistance programs even more critical for vulnerable families. Assessing the post-pandemic impact of these programs is also important to understand how they supported diet quality during a period of unprecedented stress and whether they continue to mitigate the effects of persistent socioeconomic challenges. Therefore, the objective of this study is to quantitatively explore whether the diet quality differs among mother-child dyads based on SNAP and/or WIC participation during the COVID-19 pandemic, and whether the differences in diet quality according to SNAP and/or WIC participation attenuates when including indicators of socioeconomic disadvantage in the analytic models. Additionally, we utilized a qualitative approach to explore how socioeconomic disadvantages and SNAP and/or WIC participation influence food choices and diet quality. The use of a mixed-methods approach allows for a more comprehensive understanding of how SNAP and/or WIC participation impacts diet quality by providing statistics along with perspectives on the lived experiences of mothers, offering deeper insights to strengthen these nutrition assistance programs to better support families in the face of future public health or economic crises.
Methods
Research Design
This is a sequential explanatory mixed-method study, 18 as the qualitative data were collected after the quantitative analysis to provide deeper context and explanations for the quantitative findings. The study was conducted with 69 mother-child dyads living in the greater Boston area from March to August 2022 (Figure 1). For quantitative data collection, we employed cross-sectional surveys in which the mothers completed self-administered questionnaires for themselves and their children to identify differences in diet quality based on SNAP and/or WIC participation. For qualitative data collection, we conducted in-depth interviews to complement quantitative data and further understand how socioeconomic disadvantage and other social factors impact food choices and diet quality in the family through mothers’ lived experiences.

Consort flow diagram for a cross-sectional study investigating the association between SNAP and/or WIC participation, diet quality, and parenting stress in mother-child dyads.
Study Population
Mothers were eligible for the quantitative component of the study if they met the following criteria:
1) They had a child between 2 and 5 years old. If a mother had more than 1 child within this age range, the younger child was included in the study.
2) They resided in the Greater Boston area during the data collection period.
3) They could communicate in English or Spanish without requiring an interpreter.
Mothers were excluded if:
1) They were pregnant during the study recruitment or data collection period.
2) Either the mother or child had a medical condition affecting their ability to consume food orally or requiring artificial nutrition support (enteral or parenteral).
3) They were unwilling to sign the informed consent form.
Mothers were eligible for the qualitative component of the study if they:
1) Met the eligibility criteria and participated in the quantitative component of the study.
2) Reported current participation in SNAP and/or WIC or had participated within the past 3 months.
Mothers were excluded from the qualitative component if they were unwilling to participate in the interviews or declined to sign the informed consent form.
Sampling Methods
We employed a non-probability sampling method based on voluntary responses of participants through the screening survey to participate in the quantitative data collection process. Subsequently, we invited mothers enrolled in the quantitative study who were participating in SNAP and/or WIC to participate in in-depth interviews to explore how socioeconomic disadvantage and SNAP and/or WIC participation impact food choices in the family. Sampling for qualitative data collection was based on data saturation, defined as the point at which linking concepts from 2 individual interviews reveals no additional major information. 19 Studies involving individual in-depth interviews have consistently found that approximately 90% of concepts are identifiable within the first 10 interviews and that additional interviews provide minimal additional information.19,20
Recruitment Strategies
To reach the target population, we created recruitment materials and distributed them by e-mail to 30 home visiting and family support programs (e.g., Healthy Family Massachusetts, Parenting Journey) in the greater Boston area, identified through personal connections with the research team and online searches for available programs in the area. Of 30 programs contacted, 5 responded to research team inquiries. The research team held discussions with program administrators via e-mail, phone, and Zoom® virtual meetings to explain the purpose of the study. In 4 programs, the program administrators distributed the recruitment materials to mothers who participated in their programs. In 1 program, the program administrators provided participants’ e-mails and phone numbers, and the study team contacted the mothers directly. Additionally, we distributed the recruitment materials through online social media platforms (Facebook® and Instagram®: The Family Eating Habits Study) and utilized selective paid online advertisement through Facebook® and Instagram® to reach the target audience using keywords: “mothers,” “young children,” “parenting,” and “supplemental nutrition assistance program.”
Mothers interested in participating in this study completed the screening survey online to determine their eligibility and were contacted by the research team by phone or e-mail, if eligible, for more details about the study. Mothers then electronically signed a consent form to participate in the study for themselves and their children if they agreed to participate. The consent form asked for consent to participate in the survey (quantitative) and interview (qualitative), if eligible. Mothers could choose to participate in the survey only or both the survey and the interview, if eligible. Mothers who reported participating in SNAP and/or WIC were invited to participate in in-depth interviews (qualitative part of the study) with trained researchers. Verbal consent was obtained by mothers and recorded before the start of every interview.
Measurement Instruments and Quantitative Data Collection Procedures
Data collection took place from March to August 2022. Due to concerns related to the COVID-19 pandemic from several participants, we minimized in-person contact and connected with participants by phone or e-mail, and participants self-administered all questionnaires online. Unless specified otherwise, data from questionnaires were collected and managed using Redcap® electronic data capture system. Redcap® is a secure, web-based software platform to support online questionnaire administration for research studies. 21
Descriptive characteristics
We collected descriptive characteristics and other personal data using online self-administered questionnaires completed by mothers. Mothers reported their age in years, race and ethnicity, highest education level, and annual income. Mothers also reported their child’s age in months, child’s biological sex, days in daycare per week. Race and ethnicity data were self-reported by mothers using 2 separate questions. Mothers were asked if they described themselves as Hispanic or Non-Hispanic in the first question. They were then asked to choose the race and ethnicity they identified with from a list, including African American, Black, American Indian, Asian, Latinx, Spanish, White, Mixed, or others (specify). Race/ethnicity and education level were used as indicators of socioeconomic disadvantage in the regression models; income was not used due to issues with collinearity since income is among the eligibility criteria to participate in SNAP and/or WIC.22,23
SNAP and/or WIC participation
We also collected SNAP and/or WIC participation status using online self-administered questionnaires completed by mothers. Mothers reported their SNAP and WIC participation status (yes/no) at the time of data collection. Among the 33 participants who participated in either SNAP or WIC, 21 (64%) participated in both. Thus, we created a combined SNAP and/or WIC participation binary variable (SNAP and/or WIC vs neither SNAP nor WIC).
Dietary quality
Mothers completed dietary intake questionnaires online both for themselves and their children. For mother’s diet, we utilized the Diet History Questionnaire III (DHQ III) developed by the National Cancer Institute that asks participants to report the frequency and portion size of 135 foods and beverages consumed in the past month. The questionnaire was previously validated in U.S. adults of varying race and ethnicity. 24 We assessed children’s diet using a Food Frequency Questionnaire (FFQ) previously validated in young children from multiple ethnic backgrounds that asks about 185 food items and portion size consumed in the last month. 25 We then calculated the intake of food group and nutrient intake using the Nutrition Data System for Research 2022 (NDSR 2022) developed by the Nutrition Coordinating Center of the University of Minnesota (Minneapolis, MN). For both mothers and children, we calculated the Healthy Eating Index-2015 (HEI-2015) scores as an overall measure of diet quality. The HEI-2015 measures how well a person’s diet adheres to the 2015-2020 Dietary Guidelines for Americans and has 13 components. Participants were scored for each component, and the HEI-2015 total score was calculated as the sum of each component score. The total score ranged between 0 and 100, with higher scores corresponding to better diet quality. 26 The DHQIII automatically generated HEI-2015 scores based on mothers’ food intake data. However, for children, HEI-2015 scores were calculated by the researchers using food intake data from the FFQ, utilizing the SAS code developed by the National Cancer Institute. 26
Statistical Analyses
Descriptive statistics were used to present the baseline characteristics of mother-child dyads by SNAP and/or WIC participation status. Continuous variables were reported using mean (standard deviation), and categorical variables were reported as frequencies (percentage). We used the independent t-test to examine differences in means between groups (SNAP and/or WIC vs no SNAP and/or WIC participation) for the following variables: mother’s age, child’s age, and the number of days in daycare per week. We used chi-square test to examine differences in proportion between groups for the following variables: mother’s race/ethnicity, education level, annual income, and child’s sex. The tests were computed to confirm that the selected variables were appropriate for inclusion as covariates in the adjusted models for regression analysis.
To ensure the reliability of dietary intake data, we performed log-transformation on total energy intake (calculated from DHQ III in mothers and FFQ in children) and marked the values greater than mean +3SD or less than mean – 3SD as unreliable (mothers n = 7, children n = 12). We performed log-transformation on total energy intake values from the DHQ III (mothers) and FFQ (children) to reduce skewness and stabilize variance. Following standard statistical practice for detecting outliers in nutrition research, we identified values beyond ±3 SD from the mean as potentially unreliable, as these extreme intakes are unlikely to reflect habitual dietary patterns and may result from reporting errors or misinterpretation of portion sizes. This method is commonly used in nutritional epidemiology to enhance data validity by reducing the influence of implausible dietary intake estimates. 27 To account for missing and unreliable data in mother’s (n = 11; 16%) and children’s dietary intake (n = 17; 25%), we used multiple imputation to impute missing data with mother’s age, race/ethnicity, education level, income level, SNAP participation, and WIC participation as auxiliary variables. Multiple imputation was used as it is a robust method for handling missing data under the assumption that the data are missing at random, meaning that the probability of missingness depends on observed variables but not on unobserved values. 28 Given the sociodemographic and program participation data collected, this assumption was likely reasonable, as missingness in dietary intake data was likely related to observable characteristics such as mother’s age, race/ethnicity, education level, income level, and SNAP/WIC participation status. PROC MI function in SAS was used to create 20 imputed datasets, incorporating these sociodemographic characteristics as auxiliary variables.
Pearson’s correlation was used to assess the degree of association between mothers’ and children’s HEI-2015 scores. To compare differences in mean total HEI-2015 scores between groups according to SNAP and/or WIC participation status, we conducted analysis of covariance (ANCOVA) with generalized linear models (using PROC GLM function). Two models were used: Model 1 (unadjusted) and Model 2 (adjusted for mother’s age, race/ethnicity, and education level). Separate models were computed for mothers’ and children’s HEI-2015 scores. The models for children’s HEI-2015 scores included the same covariates as the mothers’ models, with the addition of the child’s age and sex. Due to the limited number of observations relative to the number of potential predictors, we included only mother’s age, race/ethnicity, education level, and child’s age and sex as covariates in the regression models to avoid overfitting the models. Dummy variables were created for race/ethnicity and education level data in which White and master’s degree or higher were used as omitted referents in all regression models. All statistical analyses were computed using SAS (version 9.4; SAS Institute, Cary, NC) for quantitative data. The statistical significance was determined at P-value < .05.
Qualitative Data Collection Procedures and Analysis
We conducted in-depth virtual interviews using online password-protected Zoom® meeting rooms. Mothers from the quantitative study who participated in SNAP and/or WIC (n = 33) were invited to participate in the in-depth interview and 18 agreed to participate. Before each interview, participants signed a written consent form and provided verbal consent for audio recording. Trained interviewers, including researchers and research assistants (all nutritionists/dietitians with graduate-level training in qualitative research), conducted 30- to 45-min interviews with mothers (n = 18) in English or Spanish. The interviewers included both male and female researchers. Participants had no prior relationship with the interviewers but were aware of their professional backgrounds as nutritionists. This awareness may have influenced participants’ responses due to perceived expectations about nutrition-related answers. To minimize this potential bias, interviewers emphasized at the beginning of each session that they would not provide any recommendations or suggestions during the interview. They explained that the purpose of the interview was to understand participants’ actual dietary behaviors and experiences, encouraging participants to speak openly and honestly. Interviewers also assured participants that any nutrition-related questions could be addressed after the interview session if needed.
We used the Theory of Planned Behavior (TPB) as a theoretical framework to design the interview guide. TPB explains individual behavior as resulting from intentions, which in turn are influenced by attitudes, subjective norms, and perceived behavioral control. Attitude is defined as the degree to which a person has a favorable or unfavorable evaluation of the behavior of interest. Subjective norm is defined as the belief about whether peers and people of importance to the person think they should engage in the behavior. Perceived behavioral control is defined as the perception of the ease or difficulty of performing the behavior of interest. 29 TPB has been previously used in studies to understand a wide range of health behaviors including dietary behaviors 30 and dietary patterns. 31 Questions were designed to gather open-ended answers which were then coded according to the theoretical constructs of the TPB. The first set of questions was aimed to explore factors that affected how mothers made food choices in the family through theoretical constructs. The second theme was aimed at exploring how theoretical constructs lead to the intention to make food choices (through grocery shopping and meal planning), and factors that prevented mothers from performing the behaviors as they intended.
The audio recordings were professionally transcribed verbatim. Spanish-language interviews were translated into English by a bilingual research assistant who is also a nutritionist. This process ensured both linguistic accuracy and cultural relevance while preserving the accuracy of nutrition information. Qualitative data were analyzed using a thematic analysis approach involving 2 trained coders (both male and female nutritionists with graduate-level training in qualitative research) throughout the process. Before coding, both coders participated in a calibration session to review the interview guide and theoretical framework (Theory of Planned Behavior). The first coder then developed a codebook based on the initial reading of the transcripts using a combination of deductive (based on the constructs from the TPB) and inductive approach (based on identified concepts by the researchers). The 2 coders independently coded 4 interviews then combined the codes to assess inter-rater reliability. Codes with Kappa coefficient <0.7 were discussed and refined until reaching a consensus with Kappa coefficient >0.7, indicating a substantial agreement. The coders then independently coded the remaining transcripts and met to discuss and reach a final consensus. Nvivo® (Version 12; QSR International) was used for coding and thematic analysis.
Results
Descriptive Characteristics
A total of 69 participants were included in the quantitative data collection of this study, with 48% (n = 33) reported currently or recently participated in SNAP and/or WIC. Of 33 SNAP and/or WIC participants, 55% (n = 18) agreed to participate in the qualitative data collection. Descriptive characteristics were described in Table 1. Overall, we observed significant differences in mother’s age (P < .01), and proportions of mother’s race/ethnicity (P < .001), education level (P < .0001), and annual income (P < .0001) based on SNAP and/or WIC participation. Mothers who participated in SNAP and/or WIC tended to be younger, more likely be non-White, had lower educational levels and annual income, and were less likely to exclusively breastfeed their child than mothers not participating in SNAP and/or WIC in this study.
Sociodemographic Characteristics of Mother-child Dyads Participated in The Family Eating Habits Study According to Mother’s SNAP and/or WIC Participation (n = 69).

Abbreviations: SNAP, supplemental nutrition assistance program; WIC, special supplemental nutrition program for women, infants, and children.
P-values < .05 are considered statistically significant and are bolded.
Independent T-test P-value.
Chi-Square P-value.
Fisher’s exact test P-value.
Diet Quality in Mothers and Children
We examined the correlation between mother-child dyads’ HEI-2015 scores to explore potential associations. Pearson correlation analysis revealed a non-statistically significant positive relationship (Suppl. Figure 1.) between the HEI-2015 scores of mothers and their children (r = 0.26 p = 0.07). suggesting only mild level of shared dietary patterns within dyads in this study. Differences in HEI-2015 scores by mother’s SNAP and/or WIC participation status were described in Table 2. The unadjusted model (Model 1) showed that mothers who participated in SNAP and/or WIC had a lower total HEI-2015 score compared to those who did not participate (63.8 vs 70.8 points; p = 0.004). However, after adjusting for covariates including indicators of socioeconomic disadvantage (race/ethnicity and education level) in Model 2, the difference for total HEI-2015 scores in mothers became smaller and were no longer statistically significant (68.5 vs 66.3 points; P = 0.95). In children, total HEI-2015 scores were not significantly different among children of mothers who participated in SNAP and/or WIC compared to those of mothers who had not participated in both unadjusted (64.6 vs 63.2 points; P = 0.56) and adjusted models (64.4 vs 63.5 points; P = 0.82).
Differences in HEI-2015 Scores in Mothers and Children Who Participated in The Family Eating Habits Study According to Mother’s SNAP and/or WIC Participation (n = 69).

Abbreviations: HEI-2015, healthy eating index-2015; SNAP, supplemental nutrition assistance program; WIC, Special supplemental nutrition program for women, infants, and children.
Results are shown as mean (95% CI) and P-values < .05 are considered statistically significant and are bolded.
Model 1 was unadjusted.
Model 2 was adjusted for mother’s age, race/ethnicity, and education level.
Model 2 for children’s HEI-2015 score were further adjusted for child’s age and sex.
The Relationship between Socioeconomic Disadvantages, SNAP and/Or WIC Participation, and Food Choices in the Families
Key themes and representative quotes from in-depth interviews with mothers who participated in SNAP and/or WIC (n = 18) are shown in Table 3. Overall, we observed 6 key themes based on 3 theoretical constructs according to the Theory of Planned Behavior (attitudes, subjective norms, and perceived behavioral control). These qualitative findings provide further explanations for the quantitative findings.
Example Quotes for Each Theme Emerged From the In-depth Interviews With Mothers in The Family Eating Habits Study That Participated in SNAP and/or WIC (n = 18).
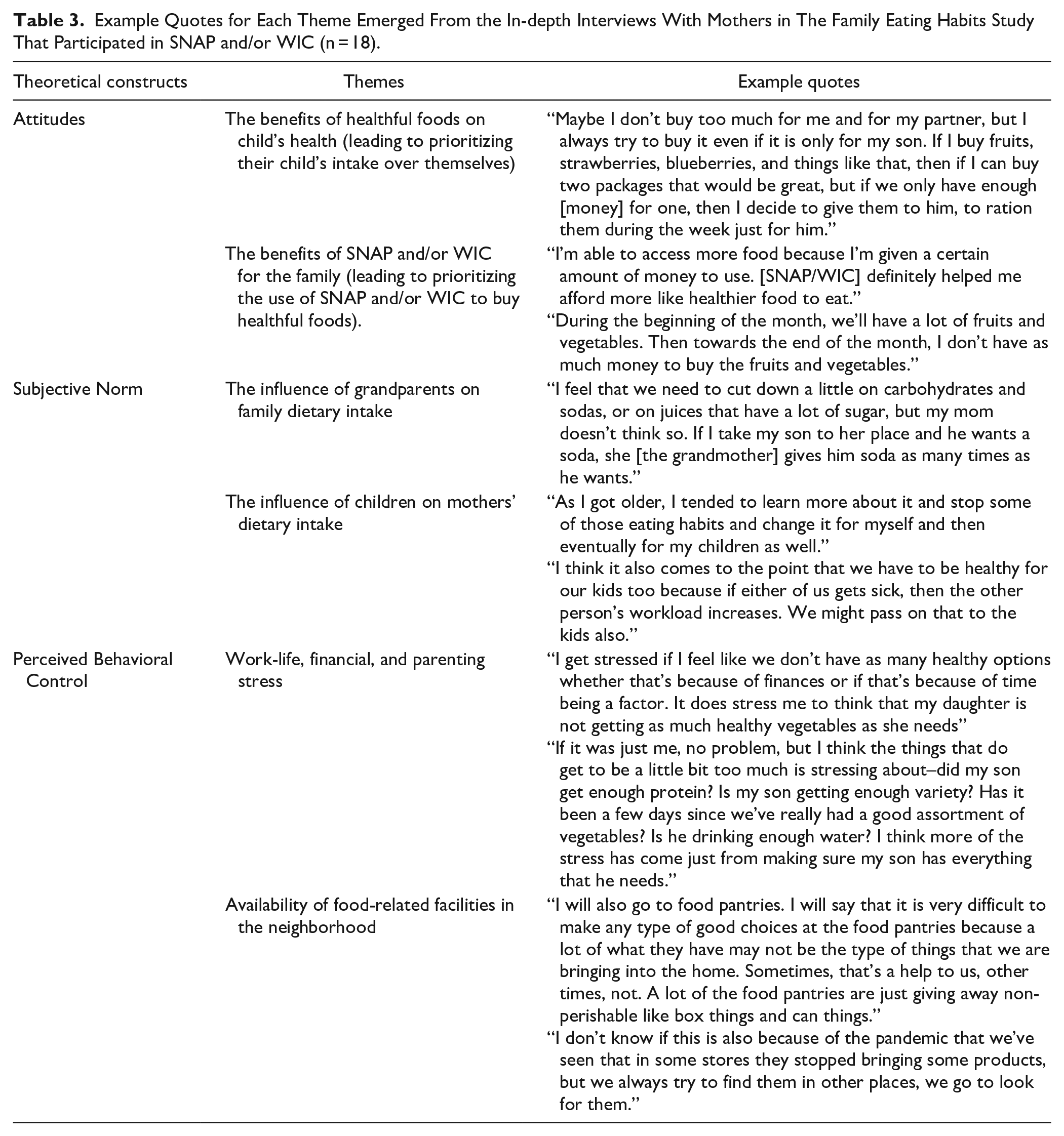
Attitudes: The benefits of healthful foods on child’s health (leading to prioritizing their child’s intake over themselves)
Overall, the themes reflected mothers’ behavioral beliefs toward healthful foods and positive outcome evaluation of healthful foods more toward their child’s health. Thus, mothers reported that they prioritized their child’s dietary intake over their own, ensuring their children had access to healthy food, as reflected by a participant, “If I can buy two packages [of fruits], that would be great, but if we only have enough [money] for one, then I decide to give them to [my son].” However, the degree of prioritization depended on the financial status of the family. When mothers could not afford enough healthy foods for every family member, some mothers and other adult family members compromised the quality of their food to ensure that their children were able to consume healthy foods.
Attitudes: The benefits of SNAP and/or WIC for the family (leading to prioritizing the use of SNAP and/or WIC to buy healthful foods)
The themes reflected mothers’ positive behavioral beliefs toward SNAP and/or WIC participation, particularly related to favorable outcome evaluation of healthful eating and that SNAP and/or WIC participation could help them with accessing healthful foods. However, mothers were concerned about increasing food prices since the peak of the COVID-19 pandemic. SNAP and WIC appeared to help families to afford more foods that they perceived to be healthful, particularly fresh fruits and vegetables, as described by a mother, “I’m able to access more food because I’m given a certain amount of money to use. [SNAP/WIC] definitely helped me afford more like healthier food to eat.” However, healthful foods were perceived to be expensive, and some families could only afford to purchase them early in the month using SNAP and/or WIC benefits. This led several families to have more limited healthful food choices toward the end of each month, as reflected by a participant, “. . . towards the end of the month, I don’t have as much money to buy the fruits and vegetables.” Thus, several mothers stated that fruit and vegetable intake in the family was simply reduced.
Subjective norm: The influence of grandparents on family dietary intake
The themes reflected normative beliefs of mothers towards grandmothers’ approval of their child feeding behaviors. Mothers reflected high motivation to comply if they perceived that grandmothers’ attitudes toward child feeding aligned well with theirs. However, motivation to comply could be low if the mothers perceived that the grandmothers disapprove their child feeding behaviors by, instead, providing foods that mothers perceived as unhealthful. This conflict in beliefs was reported by some mothers as a source of parenting stress, as mothers may have limited control over the grandmother’s behaviors. For example, a mother reflected that, “If I take my son to [the grandmother’s] place and he wants a soda, she gives him soda as many times as he wants.”
Subjective norm: The influence of children on mothers’ dietary intake
Themes reflected normative beliefs regarding perceptions of mothers that their child approved their “good mother” behaviors (e.g., providing healthful foods, being a good role model regarding healthful eating, etc.) and that mothers had high motivation to comply with the beliefs. With regards to their own intake, several mothers reported that they were not eating “healthy” when they were growing up, particularly due to the fact that healthful eating was not emphasized by their parents (who are now the children’s grandparents). However, as the mothers grew up and became mothers, they wanted their children to have healthy eating habits starting in the early years. Thus, they felt the need to change their own dietary intake, mainly to be a good model for their child and to make sure that they would stay strong and healthy to care for their children, as shared by a mother, “I think it also comes to the point that we have to be healthy for our kids too because if either of us gets sick, then the other person’s workload increases.”
Perceived behavioral control: Work-life, financial, and parenting stress
Themes reflected control beliefs that mothers perceived work-life, financial, and parenting stress all impacted how they made food choices for the family. Moreover, they reflected low perceived power as they stated that these stress factors limited their ability to make healthful food choices. Additionally, Stressors related to balancing work and family life and economic strain affected participants’ food choices—further elevated during the pandemic—more than issues related to parenting. Mothers reported that not having enough money to purchase enough healthful foods for the family was the major source of stress related to food choices. Stress related to parenting was more likely secondary to stress related to economic constraints as several mothers stated that they could not take care of their children as well as they expected because of financial constraints, mainly that the child could not eat as healthfully as the mother hoped, as a mother reflected, “I think more of the stress has come just from making sure my son has everything that he needs.” Mothers reported that this type of stress compromised healthy eating in the family but may affect their intake more than their children’s intake.
Perceived behavioral control: Availability of food-related facilities in the neighborhood
Themes reflected control beliefs related to the availability of grocery stores in their neighborhoods, which was perceived by mothers to be another factor in determining food choices for the family. As one mother explained, “I don’t know if this is also because of the pandemic that we’ve seen that in some stores they stopped bringing some products, but we always try to find them in other places, we go to look for them,” mothers needed to travel a distance to find the food products they wanted, especially foods from their cultural backgrounds. Some mothers reported difficulties accessing stores that offered fresh fruits and vegetables, particularly those without personal vehicles. Mothers described relying on public transportation, which often involved long travel times, multiple transit routes, and logistical challenges, especially when traveling with children or managing heavy grocery loads. Some mothers chose to visit farmers’ markets to use SNAP and/or WIC benefits to purchase fruits and vegetables since the prices are less expensive than those in grocery stores. They also reported that they were able to acquire staple foods (e.g., milk, cereals, rice and grains, peanut butter, cheese, etc.) at food pantries and other food-related facilities, though mothers perceived several items from food pantries as not very healthy, as one mother shared, “It is very difficult to make any type of good choices at the food pantries because a lot of what they have may not be the type of things that we are bringing into the home.” Nevertheless, because they did not have to use SNAP and/or WIC benefits on purchasing staple foods, they could afford to buy fresh fruits and vegetables (using SNAP and/or WIC benefits) at grocery stores. However, others reflected low perceived power as they experienced logistic challenges (e.g., the need to use multiple routes of public transit and longer time for each grocery shopping attempt) that make healthful food choices more challenging.
Discussion
The results from this mixed-method study showed that socioeconomic disadvantage accounted for differences in diet quality among mothers based on receipt of SNAP and/or WIC. We did not observe differences in diet quality of children in mothers based on SNAP and/or WIC participation in mothers. Qualitative data revealed that the impact of socioeconomic disadvantage on food choices in the family could be described using theoretical constructs from the Theory of Planned Behavior, particularly attitudes and perceived behavioral control. First, mothers had positive attitudes toward healthful foods and SNAP and/or WIC, as SNAP and/or WIC allowed them to purchase more foods that they perceived as healthful, such as fresh fruits and vegetables, which could help improve diet quality. However, mothers also expressed limited perceived behavioral control related to family food choices, particularly due to work-life, financial, and parenting stress, though parenting stress seems to play a minimal role in diet quality within families compared to those from work-life and financial constraints. Additionally, SNAP and/or WIC benefits received were likely not enough to allow the families to purchase healthful foods throughout the month. Therefore, the mothers prioritized giving such food to their children over themselves.
The total HEI-2015 score, an indicator of diet quality, assessed in this population was higher than what was reported in other studies. 32 33 The differences in the scores could be due to differences in characteristics of the sample population, 34 geographical location, 35 and dietary assessment tools used.36,37 Therefore, we only compare the means within the sample population utilizing the same dietary assessment method (DHQ III in mothers and FFQ in children) and not to the scores from the general population. Additionally, this study found a non-statistically significant positive-trend association between mothers’ and children’s HEI-2015 scores. This finding partially aligns with previous research indicating that parental dietary behaviors often influence children’s eating habits due to shared meals, modeling of food preferences, and similar food environments. 38 However, the strength of this correlation was not strong enough to suggest a complete overlap, likely reflecting differences in individual dietary needs, preferences, and other social factors.
Regarding total HEI-2015 scores in mothers, we found that socioeconomic disadvantage primarily accounted for differences in HEI-2015 scores among mothers. This suggests that the observed differences in diet quality were likely influenced by these underlying socioeconomic factors rather than by SNAP and WIC participation alone. Given that SNAP and WIC enrollment is closely linked to socioeconomic status, 15 our findings indicate that the programs may serve as essential support but do not fully mitigate disparities in diet quality. While SNAP and WIC participation may provide healthful food access, broader structural factors related to socioeconomic disadvantage continue to shape dietary outcomes. The results were supported by qualitative findings suggesting that mothers utilized SNAP and/or WIC benefits to purchase healthful foods, which could lead to increased consumption of healthful foods, particularly fruits and vegetables, in families. However, various stressors, including work-life balance, financial strain, and parenting challenges, also influenced diet quality. These stressors were more likely to compromise mothers’ own diet quality than that of their children, as mothers often prioritized their children’s nutritional needs over their own.
In children, we did not observe statistical differences in diet quality among children of mothers based on receipt of SNAP and/or WIC. The results may indicate that the influence of socioeconomic disadvantage on diet quality in families affects mothers more than their children. SNAP and/or WIC may increase families’ access to healthful foods, thus improving the diet quality, based on the results from previous longitudinal studies showing that longer participation in WIC is associated with higher diet quality in children.39,40 Qualitative findings supported these findings with the fact that mothers rather spent their SNAP and/or WIC benefits mainly on fruits and vegetables. Furthermore, mothers prioritized their child’s dietary intake before themselves, hoping to provide their children with as much healthy food as they could afford. The degree of prioritization, and compromise on the mother’s part, depended on financial constraints. These results may partly explain why, in this study, unadjusted differences in diet quality according to SNAP and/or WIC participation were observed in mothers but not children. Previous studies have shown that mothers experiencing food insecurity may compromise their own nutritional intake to preserve adequacy for their children’s diet. 41 The findings from this study add to the literature that this compromise may impact mothers’ overall diet quality.
An important point communicated in the qualitative results was the fact that SNAP and/or WIC benefits are insufficient to cover families’ healthful grocery costs for the month, leading to lower diet quality towards the end of the month. This is consistent with studies before the pandemic showing that adult SNAP participants purchased less healthy foods once their benefits were spent,42,43 and that fruits and vegetables were purchased more at the beginning of the SNAP benefit cycle. 44 WIC beneficiaries exhibited similar purchasing patterns of fruits and vegetables. 45 The qualitative findings suggest that families would purchase more fruits and vegetables if their benefit levels are increased, and, in contrast, fewer fruits and vegetables if benefits are reduced. Several states plan to end the temporary pandemic SNAP benefits shortly (by Spring/Summer 2023), which may have implications for families’ ability to purchase fruits and vegetables and other healthful foods. 46
Overall, the findings from this mixed-method study contribute to the literature by contextualizing how food assistance programs function post-pandemic and under economic strain. Although the acute impact of COVID-19 has diminished, economic challenges persist, as mothers in this study frequently reported that rising food prices, reduced SNAP/WIC benefits, and ongoing financial stress continued to limit their ability to maintain a healthful diet, even as the immediate disruptions of the pandemic subsided. These findings extend the current literature by illustrating how food insecurity dynamics have shifted since the pandemic, underscoring the continued need for policy responses that address persistent economic and food access challenges. The results also suggested that financial, work-life, and parenting stressors limited mothers’ perceived control over food choices and diet quality. However, SNAP and WIC participation may have helped mitigate some negative effects of socioeconomic disadvantage on maternal diet quality, though benefits were often insufficient to maintain healthy eating throughout the month. Thus, mothers frequently prioritized their children’s dietary needs over their own, reflecting a protective buffering effect that may have intensified during the pandemic and remain as long-term adaptive behaviors.
Primary care providers and community health workers can play a crucial role in improving families’ food choices and diet quality by advocating for policy changes that increase SNAP and WIC benefit levels and enhance access to affordable, nutritious foods in adequate quantities. This advocacy is especially critical in preparing for future public health crises like the COVID-19 pandemic. Providers can also address the current enrollment gap by encouraging eligible families to participate in these programs, addressing the current gap in enrollment among eligible families.47,48 Additionally, they can offer tailored nutrition education to improve food access, promote positive child-feeding practices, and provide stress management resources to help alleviate economic and parenting-related stressors. Establishing partnerships with local food banks and farmers’ markets may also help support food access and improve families’ overall well-being.
Strengths and Limitations
There were several strengths of this study. First, we were able to collect long-term food intake data online from mother-child dyads using validated FFQs, which may be challenging to obtain given the length of both questionnaires. This dyadic dietary intake data allowed us to explore the relationship between diet quality among different family members, in which the literature is currently inadequate. Second, given the small but specific population selected, the mixed-method approach of this study allowed us to understand in detail and contextualize the observed results from quantitative surveys that could be more challenging if interpreted using quantitative data alone.
However, despite a careful study design, there are limitations to this study. First, the cross-sectional nature of this study limited the ability to establish temporality. Therefore, associations observed (and not observed) do not imply causality. However, given findings related to associations between socioeconomic disadvantage and SNAP and/or WIC participation, some exploratory findings may warrant further exploration to confirm, especially in cohort studies (i.e., how participating in SNAP and/or WIC impacts the diet quality of mothers and children over time post-pandemic). Second, several aims in this study were considered exploratory due to a very limited sample size. As mentioned earlier, the aim of the study was not to generalize the results to a broader population but to provide in-depth insights and develop initial understanding of mothers’ lived experience, which could be used as a foundational information for future studies. Third, to reduce the complexity of data analysis, this study only focused on mothers and their children and limited demographic characteristics. Additionally, we did not gather detailed data on the length of time participants had been enrolled in SNAP and/or WIC, and whether mothers’ participation in WIC include nutrition education modules, which could be an important factor influencing dietary behaviors. Future studies should collect more details regarding food assistance program participation, along with exploring how other family members (e.g., father, grandparents) play a role in determining family food choices and also examine factors that were not measured in the current study that could potentially drive differences between SNAP and/or WIC and non-SNAP and/or WIC participants such as geographical location, employment status, immigration status, etc. to better understand the multifaceted role of food assistance programs. Fourth, due to study feasibility in the context of the pandemic, we only collected data from families living in the greater Boston area that spoke English or Spanish. This language barrier may have excluded families that mainly speak other languages (e.g., Chinese, Portuguese) in which dietary intake and food-related parenting practices may differ, further limiting external validity.
Conclusion
The findings from this exploratory study suggest that while SNAP and WIC participation supports families experiencing socioeconomic disadvantage (e.g., lower income and educational attainment), it does not fully eliminate disparities in diet quality. With most states announcing the end of federal emergency allotments introduced during the pandemic, reductions in SNAP and WIC benefits could further jeopardize diet quality among already vulnerable families. 46 Although preliminary, the study highlights the likely interrelationship between mothers’ and children’s diet quality, emphasizing the need for comprehensive support. Primary care providers and community health workers can play a critical role by encouraging eligible families to enroll in these programs and advocating for policy changes that enhance both access and benefit levels to promote long-term nutritional well-being.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251317334 – Supplemental material for SNAP and/or WIC Participation and Diet Quality in Mother-Child Dyads living in Greater Boston after Pandemic: A Mixed-Method Study
Supplemental material, sj-docx-1-jpc-10.1177_21501319251317334 for SNAP and/or WIC Participation and Diet Quality in Mother-Child Dyads living in Greater Boston after Pandemic: A Mixed-Method Study by Thanit Vinitchagoon, Fang Fang Zhang, Rebecca C. Fauth, Erin Hennessy, Ana G. Maafs, Emma M. Browning and Christina D. Economos in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We would like to thank all mothers and children that devoted their time to participate in this study, and also program directors and administrators of family support programs that allowed us to connect with the mothers and their children. We would also like to thank Mengxi Du and Zhongyu Li for their assistance with SAS programming. Mengxi Du and Zhongyu Li gave permission to be acknowledged in this study.
Authors’ Contributions
TV was a doctoral candidate and the principal investigator for The Family Eating Habits Study under supervision from CE. TV and CE conceptualized the current study. AM and EB, as research assistants, assisted in recruiting participants and collecting data. TV performed quantitative data analyses with contributions from FZ. TV and AM performed qualitative data analyses. TV wrote the first draft of the manuscript with contributions from FZ, RF, EH, AM, EB, and CE. All authors reviewed and commented on subsequent drafts of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for The Family Eating Habits Study was provided as part of the 2019–2023 doctoral training scholarship for Thanit Vinitchagoon by Mahidol University, Thailand. The funder had no role or involvement in any of the process.
Ethical Approval and Informed Consent Statement
This study was approved by Tufts University Social, Behavioral, and Educational Research Institutional Review Board (STUDY00002042). Participants were informed about the objectives and processes of the study. They voluntarily provided electronic consent before completing the questionnaires, and verbal assent before the interview.
Data Availability Statement
The datasets generated and analyzed in this study are not publicly available but are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.