
Abstract
Objective:
Adolescents encounter numerous healthcare access barriers, leading to poor health outcomes. Researchers developed the Total Teen (TT) program to improve access to sexual and reproductive health (SRH) and mental health (MH) services in settings providing adolescents and young adults (12-25) health services. This pilot study assessed the TT’s impact on care across three settings: school-based health clinics, a federally qualified health center, and an adolescent health clinic for 12 weeks.
Methods:
Sociodemographic data, including age, race/ethnicity, gender, and insurance status, were collected. MH was assessed using patient health questionnaire (PHQ)-9 and generalized anxiety disorder (GAD)-2 scales, and sexual health was evaluated based on CDC guidelines and additional evidence-based questions. One-on-one time, confidential consultations, SRH and MH micro visits, and referrals measured access. Descriptive statistics, Pearson Chi-square tests, and Kruskal–Wallis tests compared site outcomes, while logistic regression models adjusted for age, gender, race, and site.
Results:
Four hundred and fifty-one participated in the TT program across the three sites. Concerning micro visits and referrals, being male was associated with lower depression rates (P = .0003) and generalized anxiety disorder (P = .0099). Being males also predicted micro visit receipt (P = .0199). Concerning SRH micro visits, higher sexual behavior scores (P < .0001) were significantly associated with a greater likelihood of utilizing SRH micro visits.
Conclusions:
Results indicate that TT improves access to SRH and MH services and referrals for at-risk adolescents. Findings underscore the importance of integrating SRH and MH services into routine adolescent care and involving health organizations and providers as key stakeholders in enhancing preventive healthcare access.
Introduction
Adolescence is a distinctive and dynamic phase of human development characterized by marked physical, intellectual, emotional, psychological, and social changes.1 -3 During this period, adolescents are vulnerable to engaging in risky behaviors such as unsafe sexual practices, substance misuse, and other behaviors that may lead to unintended injuries, diseases, poor mental health (MH), and unintended pregnancy.1 -7 These outcomes can have severe and lasting health consequences.3 -7 The American Academy of Pediatrics (AAP) established a preventative care schedule recommending annual wellness visits up to age 21 to address adolescent health. During these visits, primary care providers are advised to adhere to age-specific screening guidelines for MH, substance use, behavioral, social, and emotional needs, as well as for HIV and sexually transmitted infections (STI). 8 The AAP also recommends initiating annual MH screening at age 12 and assessing the risk for substance misuse. For sexually active youth, the recommendations are to begin STI testing at age 12 and to conduct HIV testing at least once between the ages of 15 and 21.
Even though pediatric and family medicine providers in the United States (US) generally adhere to age-appropriate guidelines for wellness visits, research indicates a gap in comprehensive preventative health screenings.9,10 Standard screenings and testing procedures may not fully address an adolescent’s developmental needs. 11 Moreover, while these procedures can assess risk or detect infections, they often lack youth-friendly elements and best practices for building provider-patient trust.12,13 Essential practices such as ensuring confidentiality and demonstrating interpersonal skills are crucial for making adolescents feel comfortable disclosing sensitive information. Thrall and colleagues found that adolescents in grades 9 to 12 who were assured of confidentiality were almost 3 times more likely to discuss sex-related topics with a physician than those who were not assured of confidentiality. 14
Furthermore, previous research reported that 46.4% of adolescents and young adults (ages 17-29) altered or withheld information from healthcare providers. 15 The authors also found that adolescents and young adults were more likely to be honest with female providers, introduce themselves, and appear friendly. These factors can act as facilitators or barriers to effective healthcare and affect adolescents’ decisions to disclose confidential information or access medical care altogether. In addition to these barriers, a lack of comprehensive health insurance coverage, uninsurance, and stringent health policies that restrict adolescents’ privacy, autonomy, and confidentiality significantly hinder access to comprehensive preventative care.1,3,16,17 Other notable barriers include: (1) cultural and societal norms that undermine adolescents’ perceived ability to seek or make decisions about their care; (2) socioeconomic factors, such as age, race and ethnicity, and gender; (3) strained familial relationships; and (4) inadequate or non-adolescent-friendly care protocols and processes.3,17 -19
To address these barriers, there is a growing advocacy for an adolescent-centered care framework that prioritizes the developmental needs of adolescents within healthcare services. Adolescent-centered care integrates quality patient-centered care practices with considerations specific to adolescents’ developmental stages. The World Health Organization (WHO) outlines five essential domains for delivering adolescent-friendly healthcare (ie, equity, accessibility, acceptability, appropriateness, and effectiveness). 20 Evidence suggests implementing adolescent-centered care frameworks improves health-seeking behaviors and improves adolescent health outcomes.21 -23
The Total Teen Program
The Total Teen (TT) program is an initiative of the Comprehensive Healthcare for Adolescents Initiative (CHAI), which was established to address gaps and develop innovative solutions for the ongoing challenges in adolescent healthcare access. CHAI collaborated with adolescents, healthcare providers (i.e., psychologists, nurse practitioners, obstetrician-gynecologists), youth outreach workers, child and adolescent health researchers, hospital administrators, and youth-serving professionals to create innovative programs to improve young adult’s healthcare access and experience. This study focuses on the outcomes of the pilot TT program.
TT is a systems intervention designed for implementation in any non-emergency healthcare setting. It is an added component of a medical visit where the patient fills out the sexual and reproductive health (SRH) and MH questionnaires, receives care regarding the results, and/or receives a referral. TT includes an adolescent health assessment, immediate care, and referrals based on identified needs. TT aims to enhance adolescents’ and young adults access to and experience with behavioral screening and services, including sexual health and MH. The program leverages preventative visits at settings where adolescents and young adults seek care to screen for comprehensive SRH and MH needs. Using the WHO’s essential youth-centered care framework, the screenings and protocols were endorsed by a youth advisory group and were youth-friendly. TT is implemented through organizational policies to ensure all adolescents receive high-quality, confidential healthcare tailored to their developmental needs. This approach eliminates ambiguity and establishes universal expectations. The program aligns with the World Health Organization’s 20 framework, is billable, and is time efficient, making it attractive to organizational stakeholders.
TT is also developed using manuals comprising organizational policy, practice guidance, and clinical workflow modifications tailored to each healthcare setting. Providers addressed risk behaviors and offered services for SRH and/or MH through a micro visit (see Table A2 in the Appendix for descriptions) when assessment scores indicated moderate or higher risk, using a tailored clinical workflow (see Figure 1). A micro visit is a time-based, separate procedure or intervention performed during a comprehensive preventative or other outpatient visit. A detailed narrative of the TT workflow and additional information is reported in the Appendix. This study reports findings from a pilot test to understand whether TT achieved its intended outcomes. The research questions include:
How does participating in the TT program impact adolescents’ and young adults’ access to SRH services and referrals in primary care settings?
How does participating in the TT program impact adolescents’ and young adult’s access to mental health services and referrals in primary care settings?
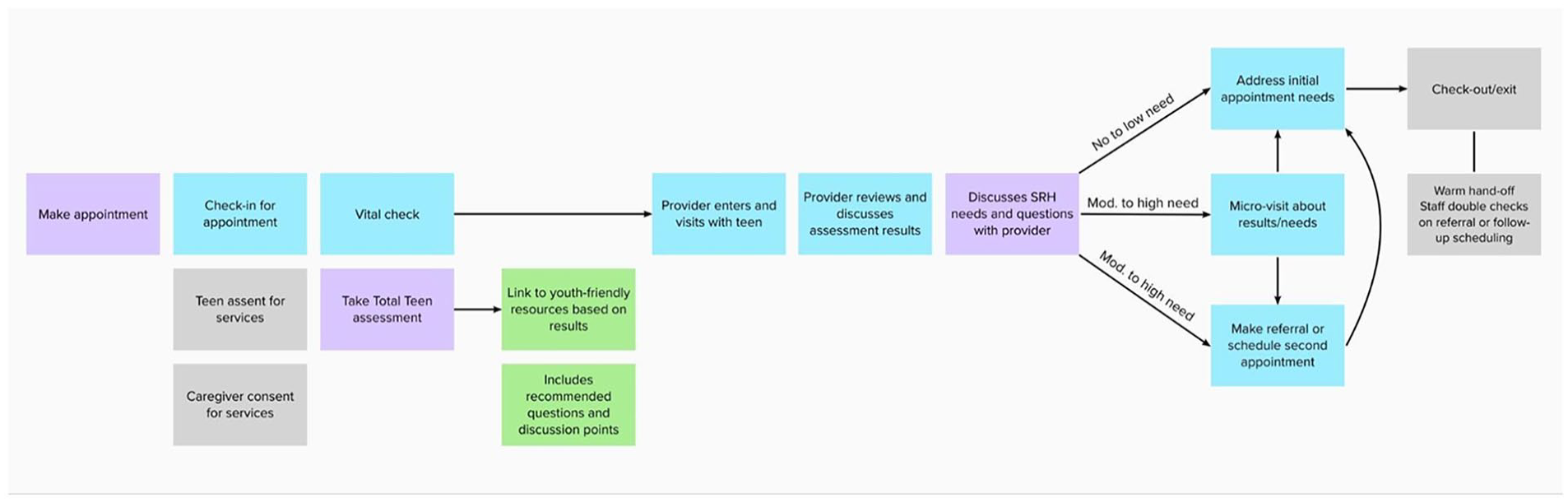
Total teen clinical workflow.
This study’s results establish TT’s significance and contribute to establishing evidence-based practices for adolescent healthcare.
Methods
Study Design
To understand the impact on access (defined as receiving a micro visit and/or referral if at risk), the CHAI team conducted a pilot test across three distinct healthcare settings where youth typically receive care—1 school-based health clinic (SBHC), a federally qualified health center, and an adolescent health clinic in communities in the midwestern, western, and southern regions of the US. These sites, all part of the CHAI network, were selected based on their setting type, diversity, geographic location, and administrative and clinical capacity to implement all aspects of the TT program. The program was implemented at all sites over twelve weeks, from October 2022 to March 2023. Patients were enrolled continually into the program throughout the twelve weeks, participated in one visit, and were not offered any follow-up services. Before the twelve-week implementation phase, the TT researcher conducted rigorous pre-implementation activities for approximately 6 months to gain partner trust, optimize program workflow and clinic setup, and develop program materials and training protocols. Feedback gathered was then used to refine the program.
Participants Characteristics
The study participants were adolescents and young adults aged 12 to 25 who sought care other than emergency services at their respective clinic sites during the study period. These adolescents received standard care as part of routine treatment but were given the option to opt out of participating in the TT program. Participants were recruited through convenience sampling, and depending on site policies, caregivers gave consent while the patients gave assent to participate in the program during a healthcare visit. After consenting to participate in the program, patients underwent the TT clinical flow, as highlighted in Figure 1.
Measures
Researchers collected sociodemographic information, including age (measured as a continuous variable), race/ethnicity (white vs. non-white—Asian, Pacific Islander, and Latino), and gender (female, male, and others).
Mental Health: Mental health measures included assessments for depression and anxiety. The Patient Health Questionnaire (PHQ)-9 is a brief, nine-item assessment using a four-point Likert scale to measure depressive symptoms. Item scores range from 0 (not at all) to 3 (nearly every day). We categorized depression severity as follows: 0-4 (minimal), 5-9 (mild), 10-14 (moderate), 15-19 (moderately severe), and >20 (severe). 24 We created a dichotomous (Yes vs. No) depression score based on responses with a PHQ-9 score of 10+. The Generalized Anxiety Disorder (GAD)-2 is a concise, two-question tool used to assess generalized anxiety disorder. Item scores range from 0 (not at all) to 3 (nearly every day). Scores are summed, with 0-2 indicating no or minimal anxiety disorder and 3-6 suggesting the presence of anxiety disorder. We categorized anxiety as 0-2 (no) and 3-6 (yes). 25
Sexual and Reproductive Health: Sexual and reproductive health measures assessed various risk factors for sexual behaviors, STIs, HPV vaccine, and healthy relationships. The assessment used the Centers for Disease Control and Prevention (CDC) Guide to Taking a Sexual History to evaluate sexual health risk. 26 This tool assesses STI prevention, STI history, and pregnancy intention. Additional questions, informed by current evidence, were incorporated to provide a comprehensive view of sexual health.
Access: Four outcome measures were collected to understand access. Providers completed a database recording whether adolescents (1) received SRH micro visits (yes vs. no – reference), (2) received MH micro visits (yes vs. no – reference), (3) were referred for MH services (yes vs. no – reference), and (4) were referred for SRH services (yes vs. no – reference).
Data Collection
All data were recorded in the clinics’ electronic health record (EHR) and/or study database. During the twelve-week study period, all sites used Microsoft Excel to record and share de-identified data with researchers every 2 weeks. Additionally, sites exported their respective TT survey data from Qualtrics, ensuring all identifying and protected health information was removed before transmission. Before data transmission, data use agreements and protocols were completed.
Data Analysis
Descriptive statistics, including median with interquartile range for continuous variables and frequency with percentage for categorical variables, were calculated for each of the 3 study settings for all participants combined. Pearson Chi-square and Kruskal–Wallis tests were employed to compare the three sites. Logistic regression models were used to analyze all outcomes, incorporating covariates such as age, gender, race, and site. Since this study involved continual enrollment of participants without follow-up visits, there were no concerns for missingness. In the Appendix, we report the PHQ-9 scores and sexual behavior scores by sociodemographic characteristics to provide further insights into the investigation. Analysis was conducted using SPSS.
Results
As shown in Table 3, 451 adolescents aged 12 to 25 participated in the TT program across the 3 sites. The TT participants had a mean age of approximately 16 (SD = 2.02). Of these participants, female and 58% identified their gender as female.
Study Characteristics
Most participants (N = 313, 69%) were from the school-based health center (SBHC). Significance differences were observed within-group across several variables: age (<.0001), race (<.0001), PHQ-9 (.09), MH micro visit (<.0001), and SRH micro visit (<.0001), and referral (<.0001) (Table 1).
Study Characteristics by Sites, N = 451.
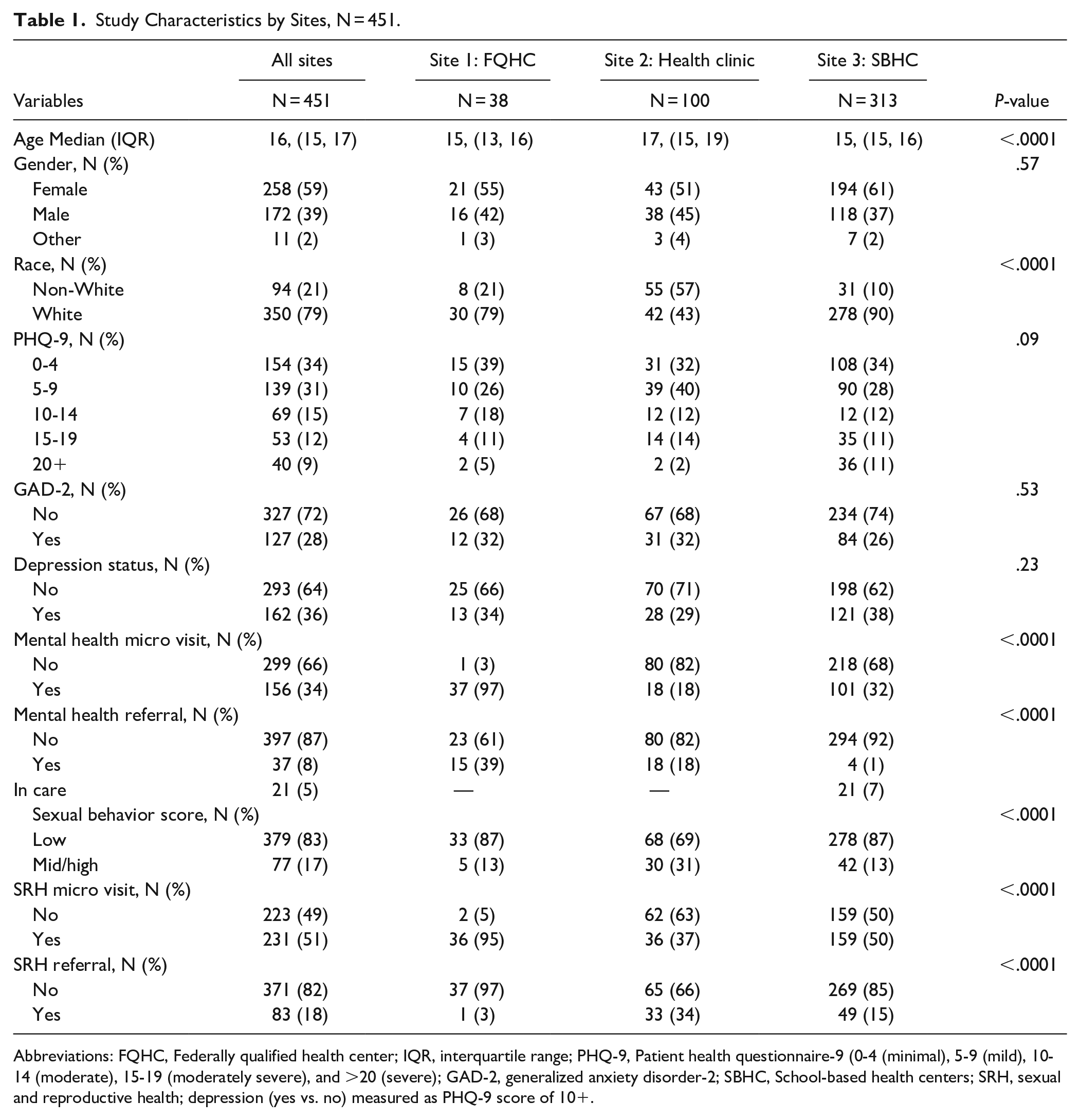
Abbreviations: FQHC, Federally qualified health center; IQR, interquartile range; PHQ-9, Patient health questionnaire-9 (0-4 (minimal), 5-9 (mild), 10-14 (moderate), 15-19 (moderately severe), and >20 (severe); GAD-2, generalized anxiety disorder-2; SBHC, School-based health centers; SRH, sexual and reproductive health; depression (yes vs. no) measured as PHQ-9 score of 10+.
Mental Health Screening
Table 2 presents regression models for MH screenings, including depression status and GAD-2 scores, analyzed by age, gender, race, and site. Being male was positively correlated with lower depression levels and generalized GAD-2 scores (OR = 0.438, 95% CI: 0.280-0.685) and (OR = 0.537, 95% CI: 0.334-0.861). Additionally, older age was significantly associated with higher GAD-2 (OR = 1.145, 95% CI: 1.008-1.301).
Mental Health (Depression Status and GAD-2) by Age, Gender, Race, and Sites. N = 451.
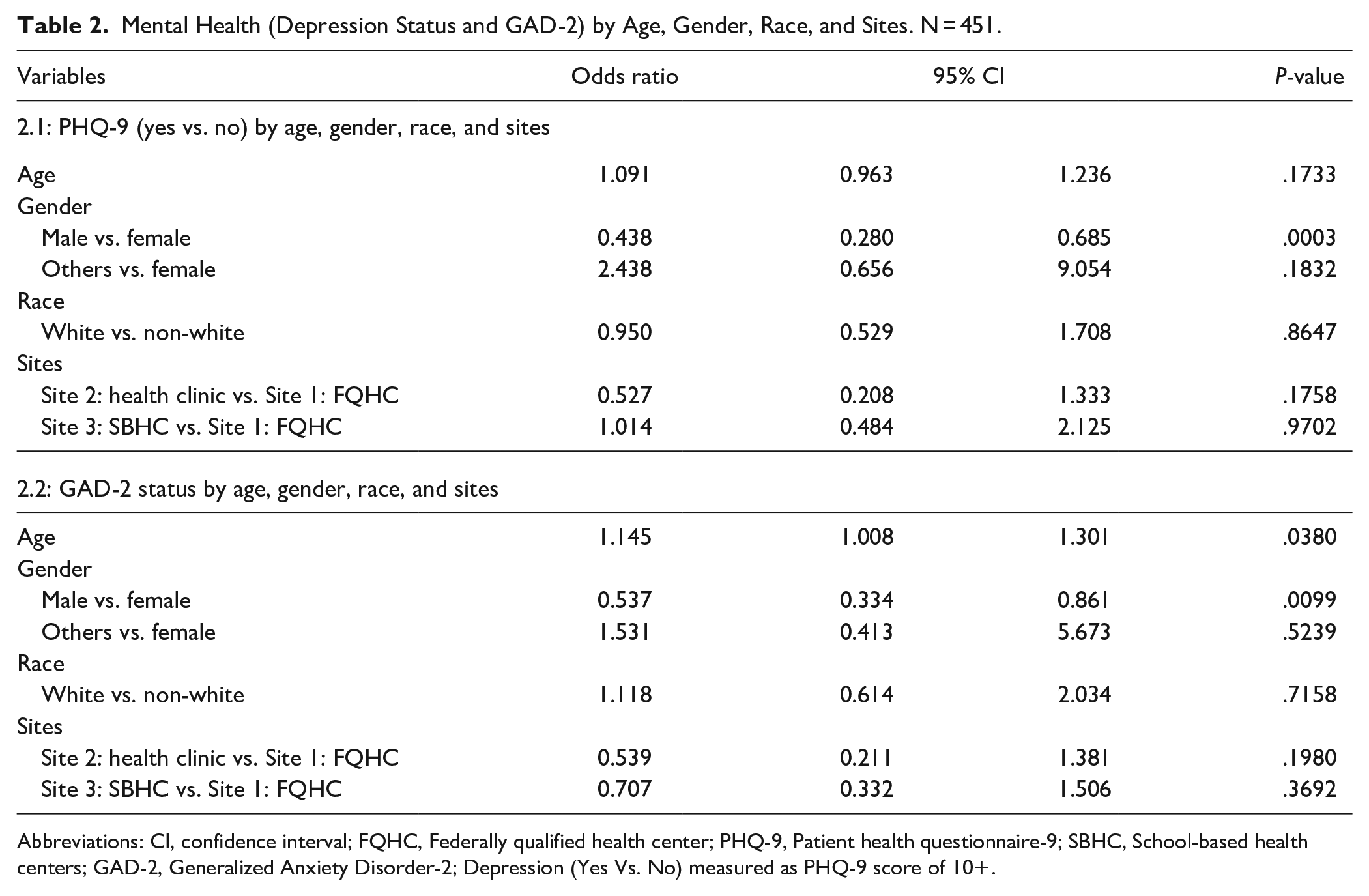
Abbreviations: CI, confidence interval; FQHC, Federally qualified health center; PHQ-9, Patient health questionnaire-9; SBHC, School-based health centers; GAD-2, Generalized Anxiety Disorder-2; Depression (Yes Vs. No) measured as PHQ-9 score of 10+.
Mental Health Micro Visit and Referral
Table 3 reports the results of MH micro visits and referrals by age, gender, race, PHQ-9, GAD-2, and site. Regarding MH micro visits, male gender was negatively associated with receiving micro visits, controlling for age, gender, race, and settings (OR = 0.518; 95% CI: 0.298-0.901). Higher PHQ-9 scores were associated with a higher chance of receiving MH micro visits: mild vs. minimal (OR = 2.878; 95% CI: 1.407-5.887); moderate versus minimal (OR = 3.962; 95% CI: 1.695-9.260); moderately severe versus minimal (OR = 6.206, 95% CI: 2.372-16.237), and severe versus minimal (OR = 17.938, 95% CI: 5.719-56.265). Additionally, there were statistically significant differences in MH micro visits receipt across the settings. In the MH referral model, adolescents with higher PHQ-9 scores had a lower probability of seeking MH referrals than those with lower PHQ-9 scores: mild vs. minimal (OR = 0.275, 95% CI: 0.101-0.750); moderate versus minimal (OR = 0.186, 95% CI: 0.060-0.577); moderately severe versus minimal (OR = 0.089, 95% CI: 0.026-0.302); and severe versus minimal (OR = 0.141, 95% CI: 0.033-0.599). Additionally, receipt of services in the health clinic and SBHC was associated with MH referral services.
Mental Health Micro Visits and Referral by Age, Gender, Race, PHQ-9, GAD-2, and Site. N = 451.

Abbreviations: CI, confidence Interval; GAD-2=Generalized Anxiety Disorder-2; FQHC, Federally qualified health center; PHQ-9, Patient health questionnaire-9 (0-4 (minimal), 5-9 (mild), 10-14 (moderate), 15-19 (moderately severe), and >20 (severe); SBHC, School-based health centers.
Sexual and Reproductive Health Micro Visit and Referral
In the analysis of the SRH micro visits, regression models revealed that older age (OR = 1.183, 95% CI: 1.018-1.374) and higher sexual behavior scores (OR = 21.358, 95% CI: 8.334-54.738) were significantly correlated with utilizing SRH micro visits. Additionally, there was a significantly positive correlation between offering micro visits at the health clinic (OR = 0.005, 95% CI: <0.001-0.030) and SBHC (OR = 0.039, 95% CI: 0.0090-0.170). Regarding SRH referrals, regression analysis showed that being male predicted lower odds of receiving SRH referrals (OR = 0.361, 95% CI: 0.183-0.712). Higher sexual behavior scores were positively associated with SRH referrals (OR = 15.743; 95% CI: 8.000-30.977). Lastly, there was a positive correlation between the receipt of SRH referrals in the health clinic (OR = 17.168, 96% CI: 1.921-153.456) and SBHC (OR = 9.628, 95% CI: 1.136-81.638) and SRH referrals (Table 4).
Sexual Health Micro Visit and Referral by Age, Gender, Race, Sexual Behavior Score, and Sites N = 451.

Abbreviations: CI, confidence interval; FQHC, Federally qualified health center; SBHC, School-based health centers.
Discussion
The results of this study indicate that the Total Teen program increases access to SRH and MH services and referrals for at-risk adolescents they otherwise would not have access to, particularly during routine preventative assessment. We observed that at-risk youth were spotted from TT’s screening (in addition to the standard practice) and, as a result, received corresponding services and referrals.TT is designed to be youth-friendly, incorporating structured intervention processes to ensure that adolescents are screened for all developmentally appropriate risks. By integrating SRH and MH micro visits into existing clinical workflows, findings support the literature on the benefits of comprehensive preventative screenings during routine generalized assessments. Furthermore, these results align with Healthy People 2030 objectives to enhance adolescent preventive healthcare visits. 27
Our study demonstrated that the TT program provided adolescents with access to SRH and MH services through micro visits but only increased referrals for SRH. Comprehensive preventive care, which includes a range of services such as sexual health and MH screening, is crucial for addressing adolescent health needs. 8 Although TT did not increase referrals for MH services, this finding is consistent with the observation that higher PHQ-9 scores were inversely related to referrals. This is likely because adolescents with higher PHQ-9 scores received immediate micro visits, during which providers could address critical issues, explore signs of crisis, and de-escalate situations. Anecdotal feedback from the implementation process indicated that many adolescents scoring high on the PHQ-9 were already receiving professional help, reducing the need for additional referrals. The literature supports the narrative 28 suggesting increased odds of receiving MH referrals and treatment among youths with MH conditions.
Consistent with existing literature, 17 increasing age was associated with a higher likelihood of having higher SRH risk scores and receiving SRH micro visits. Similarly, older age predicted higher MH risk scores, suggesting that older adolescents are at greater risk for adverse SRH outcomes and poor MH. This may be due to increased exposure to risky sexual behaviors and conditions that contribute to poor MH health in adolescents age. 3 The findings are plausible given that as adolescents mature, they begin to spend more time with peers, assert their independence, and engage in activities without parental or guardian supervision.1,29 Additionally, compared to their younger counterparts, older adolescents are more likely to discuss health-related issues with their PCPs,13,15,17 which may lead to greater utilization of preventive services, as evidenced by the higher likelihood of receiving SRH micro visits in our study. Thus, age is critical in understanding the onset of risky behaviors and their varying impacts throughout adolescence. These findings highlight a valuable opportunity for researchers and clinicians to develop age-specific, developmentally tailored interventions.
Our findings corroborate previous studies, indicating that males are less likely to report higher PHQ-9 scores than females. 30 Consequently, males had a lower chance of receiving an MH micro visit or referral. Research suggests females may be at increased risk for adverse MH conditions due to a combination of social, environmental, hormonal, and behavioral factors that differ from those affecting males. 31 While it is important not to overlook the MH health needs of males, this study underscores the importance of understanding and addressing the sex-and gender-specific effects on adolescent MH.
Healthcare settings are crucial in designing and delivering services to adolescents. The analysis revealed differences in access to and referral for SRH and MH micro visits across the participating sites. The health clinic and SBHC had lower chances of providing MH micro visits or referrals. On the other hand, participants in this study sought SRH services in the FQHC. FQHCs, as safety-net providers, offer primary care and a range of non-clinical services regardless of insurance status or financial means. Despite their successes in bridging access gaps, research indicates that FQHCs need help to enhance patient experiences. 32 Consequently, our results underscore the need for continued improvements in FQHC service delivery, particularly for adolescents.
Public Health and Policy Implications
Results from this twelve-week pilot test evaluating the impact of the TT program on SRH and MH access and referrals for adolescent patients highlight the value of integrating comprehensive screening into routine physical assessments. 33 Although complementary, these findings support the benefits of TT over other evidence-based programs, such as integrated behavioral health models, 34 which typically offer singular screenings. The design of TT aligns well with integrated behavioral health service models, such as the Primary Care Behavioral Health (PCBH) Model, 35 as the screening can facilitate the referral of patients into PCBH care.
This study highlights the essential roles of health systems and clinicians in addressing adolescent health. By incorporating the TT program into existing clinical workflows, providers could offer micro visits and make referrals without disrupting their work schedules. This approach underscores the importance of adopting a systems-based perspective rather than focusing solely on individual behavior changes to effectively meet adolescents’ healthcare needs.
As demonstrated in this study, increasing adolescents’ access to care can be achieved across various settings where they receive medical services. However, our findings suggest that FQHCs may face challenges in delivering quality, adolescent-centered care. Given that FQHCs are indispensable healthcare access points for low-income and underserved populations, including adolescents and young adults who seek care at these centers, it is paramount for policymakers to address the barriers faced by FQHCs. 32 Continued efforts to overcome these obstacles are vital to improving the quality of care for this vulnerable population.
Adolescent-centered care requires that health services be both accessible and appropriate to reduce disease burden and promote optimal health. Health professionals and clinicians must develop age-appropriate and gender-responsive health promotion and education strategies that are youth-friendly and in understandable formats to facilitate comprehension.
Strengths and Weaknesses
This study has several strengths and limitations that should be considered. First, we show that comprehensive preventative visits could be harnessed to provide age and developmentally appropriate services, including referral services that young people may not limited access to. Second, we used a systems approach to design an innovative adolescent-centered service implemented across 3 diverse settings with broad patient demographics. However, these settings are only exhaustive of some environments where adolescents receive care, which may limit the generalizability of the findings. Third, this study employed rigorous evaluation methods to increase adolescent access during primary care visits. This is substantial considering the need barriers adolescents encounter when seeking confidential care and general health services. Concerning the limitation, conducting the study within 12 weeks constrained the number of participants and potentially affected the robustness of the results. Long-term outcome research and evaluations across a wider range of settings are needed to assess the effectiveness of the Total Teen (TT) program more comprehensively.
Furthermore, we need not include follow-up visits, which would have provided longitudinal insights into the program. Since results from this pilot study are promising, continuing to build on this research (e.g., randomized controlled trials) would be instrumental in expanding the program and establishing effectiveness. Even though the sample size was sufficient to provide robust results, we relied on convenience sampling, which may have led to selection bias for the sites included. We also needed varied sample sizes across the sites. Specifically, the FQHC had a substantially lower sample size than other sites, which may have skewed our findings on MH and SRH referrals and micro visits. Thus, these results must be interpreted with caution.
Additionally, due to site preferences, sexual orientation was not universally assessed, and only gender was recorded, which restricts the data available for understanding the needs of sexual minority youth. Future research should engage community members and organizations that provide social services, such as sexual health promotion and activities, to encourage positive, modifiable behaviors, address access gaps, and meet adolescents where they are.
Conclusions
Innovative health interventions and programs are essential for delivering comprehensive developmental care to adolescents. This study demonstrates that integrating SRH and MH services into routine adolescent care can provide timely preventive interventions, improving health outcomes. Importantly, the findings highlight the necessity of involving health organizations and providers as key stakeholders, rather than external entities, in enhancing adolescents’ access to and utilization of preventive healthcare services.
Footnotes
Appendix
Acknowledgements
The authors acknowledge and appreciate the adolescents who participated as youth advisory members and health professionals who provided invaluable insights into developing the Total Teen program. The authors also thank all participating sites where Total Teen was implemented.
Authors’ Contribution
All authors contributed to the study’s conception and design. Material preparation, data collection and analysis were performed by (Whitney Garney), (Gan Han), (Christ Esquivel), (Kristen Garcia), and (Kelly Wilson). The first draft of the manuscript was written by (Kobi V. Ajayi) and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Office of Population Affairs in 2020 under grant agreement number TP2AH000074-01-00.
Ethics Approval
All study recruitment and measurement procedures were approved by the Texas A&M University Institution’s Review Board and by the respective clinic sites before implementation when required.
Informed Consent
Active parental consent and youth assent were obtained from all participants.