
Abstract
Dermatofibrosarcoma protuberans (DFSP) is a rare slow-growing skin cancer with a great capacity for local destruction. DFSP can manifest in a myriad of ways. This case report aims to contribute to the literature by increasing awareness of this condition, along with common diagnostic practices and treatment regimens. We present a 52-year-old Filipino woman who was evaluated for dyspnea with an incidental finding of an indeterminate nodule on imaging. A comprehensive diagnostic workup confirmed dermatofibrosarcoma protuberans (DFSP), which was ultimately treated with surgical resection. Clinically, about 52% of patients are misdiagnosed, leading to poor outcomes. Therefore, awareness, early detection, multidisciplinary treatment, and lifelong screening are essential for optimal outcomes.
Introduction
Dermatofibrosarcoma protuberans (DFSP) is a locally aggressive cutaneous soft tissue sarcoma. While its occurrence is rare, occurring at a rate of 0.8 to 4.5 cases per million, its propensity for recurrence is high. 1 Therefore, vigilant monitoring is warranted. DFSP is typically centered in the dermis or subcutaneous tissue and presents as an asymptomatic indurated lesion that slowly enlarges over time. While these indurated lesions are mostly located in the trunk (50%-60% of cases) and upper extremities (25%), involvement of the head and neck account for 10% to 15% of cases. 2 Given its slow growth pattern in the early stages, diagnosis is often delayed for months to years. DFSP predominantly affects individuals aged 20 to 50 years, with a notable increased incidence in African Americans. 3
The pathogenesis of DFSP lies in the chromosomal translocation, specifically translocation of t(17; 22) (q22; q13) that generates a fusion gene of COL1A1-PDGFB, which ultimately drives oncogenesis by mitogen activation. 2 Diagnosis requires a high degree of suspicion and may be suspected through physical examination. 1 DFSP can extend beyond visible structures; therefore, confirmatory biopsy with staining is needed to make the diagnosis. DFSP typically stains positive for CD34 in 80% to 100% of cases. Classically, the role of imaging in diagnosing DFSP is to determine the extent of disease. Treatment involves wide local excision with negative margins as the primary approach. Mohs surgery using CD34 staining is recommended for lesions in cosmetically sensitive areas, and radiation therapy is considered for positive margins after surgical resection.
Metastasis is extremely rare, occurring in approximately 5% of cases. However, tumor recurrence has an increased risk of transforming into a more malignant form of DFSP known as the DFSP-fibrosarcomatous variant (DFSP-FS), in which the lungs are a common metastasis site. 1 Current literature has cited recurrence rates approaching 50%; therefore, long-term follow- up is needed. 2 If recurrence or metastasis occurs, targeted molecular therapy toward the PDGF receptor by the agent imatinib (Gleevec) has been shown to potentiate clinical remission. 4
Case Presentation
A 52-year-old Filipino woman with a history of type 2 diabetes, hypertension, congestive heart failure (CHF), and hyperlipidemia presented to the hospital with acute dyspnea on exertion.
Physical examination revealed normal breath sounds with bilateral lower extremity edema. Initial laboratory tests were notable for a mild leukocytosis of 10.3, with the remaining CBC, BMP, and NT-proBNP unremarkable. None of these findings explained her dyspnea, therefore, a CT Angiogram (CTA) was performed to rule out pulmonary embolism; it incidentally revealed likely reactive lymphadenopathy in the celiac axis lymph nodes. The finding prompted further investigation with a CT scan of the abdomen/pelvis without contrast, which identified an indeterminate 2.2 cm nodule in the subcutaneous fat of the right lateral gluteal area (Figure 1).

Dermatofibrosarcoma protuberans presentation as an asymptomatic indeterminate 2.2 cm nodule on CT abdominal pelvis without IV contrast.
Given these findings, a biopsy was recommended for further evaluation. Visually, the lesion presented as a pigmented macule (Figure 2).

Superficial appearance of skin on patient’s right lateral gluteal area, prior to biopsy.
Ultrasound-guided fine needle aspiration of the area in question was strongly positive for CD34 while negative for desmin, actin, and SOX10, highly suggestive of dermatofibrosarcoma protuberans (Figure 3).
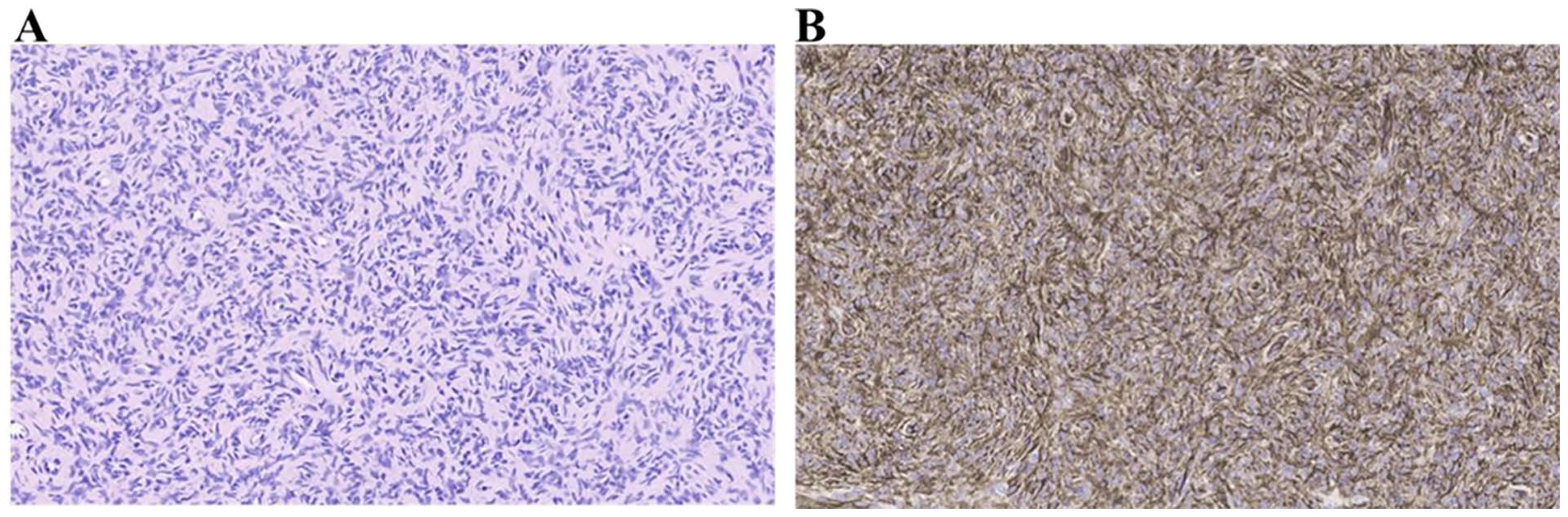
(A) Deeply infiltrative proliferation of uniform spindle-shaped cells arranged in a storiform distribution (hematoxylin & eosin; ×20) (B) Diffuse and strong positivity for CD34 (IHC; ×20).
Following the biopsy, the patient had an appointment with Orthopedic Surgery, who performed seed localization to precisely locate the tumor and successfully achieved negative margins during its resection. Final pathology confirmed DFSP, with the final tumor dimensions recorded as 2.8 cm × 2.6 cm × 2.5 cm. A follow-up CT of the abdomen/pelvis in 4 months was scheduled as part of her initial surveillance.
Of note, further investigation determined her dyspnea was related to her known CHF diagnosis.
Discussion
This case demonstrates the importance of incidental findings. The patient presented with an unrelated symptom, and subsequent imaging led to the diagnosis of DFSP. DFSP typically presents superficially, allowing clinicians to suspect tumor extent and lymph node involvement through physical examination. 1 Imaging may be helpful for larger or recurrent tumors where metastasis is suspected, but is not the standard diagnostic tool for DFSP. However, as evident in this case, DFSP may manifest in bodily folds, which can often be challenging to detect. Whether detected incidentally or reported by a patient, appropriate follow-ups are necessary for successful management.
Annual and thorough skin examinations play an important role in early detection. The patient may describe a slowly growing lump that might have started as a pimple or rough skin patch. While the epidemiology profile of DFSP is highest among women and African Americans, DFSP can manifest across many demographics. 5 Physical examination may reveal either a benign or gnarly lesion; so, the clinical differential may initially be broad and include conditions such as neurofibroma, leiomyoma, malignant melanoma, keloid, desmoid tumors, dermatofibroma, and sarcoidosis. 6 A core needle or incisional biopsy with strong CD34 staining is the gold standard for definitive diagnosis of DFSP. 1 Imaging may help determine the extent of the disease; in particular, MRI is preferred for visualizing DFSP, while CT scans are helpful when bone involvement or lung metastases are suspected.
Once diagnosed and before treatment, patients should understand that surgical excision, whether through Mohs micrographic surgery or wide local excision remains the preferred treatment.
However, postoperative radiotherapy may be considered as adjuvant treatment when there are high risk factors such as positive surgical margins, close surgical margins and recurrent or metastatic tumors when surgical excision is not feasible. In patients with advanced or metastatic disease, treatment with tyrosine kinase inhibitors show promise and highlighting the evolving landscape of DFSP treatment. 7 Once shared decision-making is achieved, treatment of DFSP should be approached within the framework of a multidisciplinary evaluation involving primary care physicians, dermatologic, orthopedic, and plastic surgeons, and potentially surgical oncologists. 6 Clear and concise communication among the treatment team is crucial for successful care coordination and patient-centered care.
Following surgical management, post-treatment surveillance is vital for preventing recurrence. Rates of recurrence2,8 can range from 13% to 50% and the risk of conversion to malignant DFSP-FS increases. 1 Risk factors for recurrence include late recognition due to initial misdiagnosis, tumors located in the head/neck or perineum, tumors larger than 3 cm, DFSP-FS on initial presentation, and a history of recurrence. Current screening recommendations include regular self-examination (particularly of the primary site) every 6 months for 3 to 5 years, followed by lifelong annual skin checks, as planned for our patient. The development of a skin-colored to brownish-red plaque that progresses to become multiple raised nodules may be the first clue of recurrent disease.
Radiographic surveillance is necessary for those with recurrent DFSP or DFSP-FS. While the prognosis for DFSP is favorable, with a 10-year survival rate of 99.1%, once metastatic, mortality occurs approximately 2 years post-diagnosis. Therefore, proper diagnosis and treatment can drastically improve one’s quality of life.
In conclusion, although DFSP is an uncommon sarcoma that typically presents with findings of a cutaneous noduloplaques, rarely lesions may be deeper in presentation necessitating the use of imaging techniques for detection. Additionally, biopsies for histopathologic evaluation are required for diagnostic confirmation. Treatment strategy should involve combination of surgical excision, radiation therapy or pharmacotherapy, depending on disease extent. Close monitoring for local recurrence posttreatment is essential. To enhance patient-centered care, outcomes, and safety related to DFSP, an effective multidisciplinary approach is required.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images in this article.