
Abstract
Introduction:
Homeless service workers play a key role in addressing the social and health needs of people experiencing homelessness, yet little is known about their own health status and behaviors.
Methods:
A nationwide survey of Hungarian homeless service workers (n = 548) was conducted using a short version of the European Health Interview Survey. The results were compared with age- and sex-adjusted data from the general Hungarian population.
Results:
Despite reporting good health, one-third of homeless service workers had long-standing health problems, with one-fourth experiencing activity limitations. Mild (29.1% vs 17.2%) and moderate (8.5% vs 4.7%) depressive symptoms were nearly twice as prevalent among service workers. They also reported lower daily consumption of fruits and vegetables (41.4% and 26.3% vs 57.0% and 45.4%) and a higher rate of daily smoking (35.4% vs 26.4%). Additionally, 59.3% were classified as overweight or obese. Participation in organized cancer screenings was higher among homeless service workers but stayed below 50% in both groups.
Conclusions:
These findings can serve as a foundation for developing strategies to improve the health status of homeless service workers. Ultimately, this benefits both the workforce and the quality of services provided.
Introduction
Although the rate of people who are at risk of poverty and social exclusion has been relatively stable in Europe for decades, homelessness, the most extreme manifestation of these situations, is increasing rapidly. 1 In 2023, the estimated number of people sleeping rough or in emergency housing was almost 900 000, representing a more than 70% increase over the past decade. 2 Hungarian homelessness surveys mirror this trend, with rising numbers of citizens using homeless care services annually. 3 In February 2022, Hungary estimated 6944 people were homeless, with one-fourth sleeping rough and three-fourths in emergency accommodations or hostels. 4 Asylum seekers, refugees, and migrants, recorded by a separate system, may also be present in significant numbers.
People experiencing homelessness (PEH) are among the most deprived and vulnerable in society, often facing complex health issues due to harsh and chaotic living conditions and lifestyles, poorly managed diseases, addictions, and mental health problems.5 -8 They are also excluded from mainstream society, worsening their situation in multiple aspects.
Homeless service workers, who operate various support services to PEH, have to deal with several factors that make them susceptible to physical and mental health disorders. Frontline professionals face long working hours, heavy workloads, and high demand. 9 They are expected to be “problem-solvers,” “crisis managers,” and “case managers.” Studies, including those conducted in Europe and overseas, highlight that these workers experience high levels of stress, even secondary traumatic stress, frustration, exhaustion, and burnout, with factors such as role conflicts and a strong sense of responsibility contributing to their difficulties.10 -14 Environmental health conditions in shelters, like poor ventilation and overcrowding, also negatively affect the health of both PEH and service workers. 15 Finally, these job characteristics are often associated with high smoking rates and alcohol consumption. 16
While research on the mental health challenges of homeless service workers is extensive, less is known about their overall health, health behaviors, and healthcare use. 11 Our study aimed to fill this gap by conducting a national survey to evaluate the health status, health determinants, and preventive service use of frontline workers in homeless services. We compared our findings to the European Health Interview Survey (EHIS) data on the general Hungarian population, hypothesizing that homeless service workers would exhibit less healthy behaviors, lower preventive service use, and consequently worse health outcomes.
Methods
Design and Sample
The Homeless Service Health Survey (HSHS) was a cross-sectional study to assess the health status, health behaviors, and preventive service use among Hungarian homeless service workers. The survey was conducted nationwide in 77 cities, targeting frontline workers employed in various settings, including night shelters, day centers, temporary accommodations, health centers, and street services. Data collection occurred between February 3 and 20, 2018. All full-time employees were eligible and invited to participate through their workplace. Participation was voluntary and subject to informed consent.
For comparative analysis, secondary data from the last round of the European Health Interview Survey (EHIS) in Hungary was utilized. 17 The EHIS provides nationally representative, cross-sectional data on the same indicators in every 5 years using a standardized questionnaire supervised by Eurostat. 18 In Hungary, stratified 2-step probability sampling was applied to provide precise estimates of health status indicators for the Hungarian population those aged 15 years and older, living in private households. 17
Measures
The HSHS questionnaire consisted of 43 items, 31 of which were derived from the Hungarian version of the EHIS 2014. 19 These items addressed various domains: sociodemographic background (3 items), health status (4 items), mental health (8 items), health determinants (9 items), use of outpatient services (1 item), and preventive health services (6 items). Mental health was measured via the Patient Health Questionnaire-8 (PHQ-8), a validated 8-item diagnostic and severity measure for depressive disorders. 20 Additional questions were developed for the study to capture the unique aspects of the homeless service workers’ experience. These included questions about reasons for not feeling healthy, tuberculosis screening in the past 12 months (this examination is legally required for frontline homeless service workers on an annual basis in Hungary 21 ), opinions on how much homeless service workers can do for their own health, structured dietary routines, frequency of cooked food consumption, and views on the health of homeless people and possible ways to improve it. Further questions focused on employment details: the type of homeless service as a workplace (ie, homeless accommodation/street service for homeless people/other), and the years spent in the homeless service (ie, 0-5 years, 6-15 years, and more than 15 years). Finally, the questionnaire captured the geographical location of the workplace to assess regional differences. Questionnaires were self-administered.
Statistical Analysis
HSHS data was compared with the nationally representative data of the EHIS 2014 in Hungary, along with the variables on health status, mental health, use of health care, and health determinants. In order to avoid bias due to the demographic composition of the homeless service workers’ sample, the EHIS 2014 data was weighted according to the internal demographic composition of the HSHS sample along the following dimensions: gender (2 categories) and age (6 categories).
Pearson’s Chi-square test was used for hypothesis testing with a significance level of 5% for comparison of categorical variables. The maximum margin of error (half of the width of the 95% confidence interval) of the prevalence estimates was determined by the following formula 22 :

Where n is the sample size. In our case, the maximum margin of error for estimates for the homeless caregiver population was ±4.14%, for the general population ±1.30%.
Responses with missing values were removed listwise.
To assess the use of preventive services, we included only those who were eligible for the organized screening programs based on the national recommendations 23 : ages 45 to 65 years for breast cancer screening, 25 to 65 years for cervical cancer screening, and 50 to 70 years for colorectal cancer screening. Data on tuberculosis screening was not available for the general population, as this indicator is not included in the EHIS survey.
The chi-square test was used to examine differences or independence between categorical variables. In the study, we evaluated whether the observed frequencies in the sample of homeless service workers deviate significantly from the frequencies in the sample of the general population in Hungary. We applied a 95% confidence level (P < .05) to determine statistical significance, marking results as significant based on this threshold.
Results
A total of 548 participants aged 21 to 70 years (43.4 ± 10.2) from 51 cities responded to the survey. The sample was 61.7% female, and one-third worked in the capital (35.6%). Demographic characteristics are summarized in Table 1. The results were compared with the age and sex-adjusted data of the EHIS (N = 5621). Figure 1 presents the difference between the unweighted and the weighted EHIS sample composition.
Demographic Characteristics of the Hungarian Homeless Service Workers’ Sample.

People worked in medical institutions, offices, public kitchens, or day centers.
People with multiple positions in different workplaces of the homeless service.

Sample composition of the unweighted (N = 5622) and the weighted (N = 5621) national European Health Interview Survey sample.
Health Status
The self-perceived general health ratings differed significantly (P = .002) between the general population and homeless service workers (Table 2). Among the latter group, 71.1% perceived their health as good or very good, compared to 68.2% of the general population. The primary reason reported by homeless service workers for not feeling completely healthy was a lack of time to address their own health, with half of them citing this issue (50.9%). Additionally, 29.1% attributed their poor health to insufficient financial resources, while 21.4% identified a chronic disorder as the main factor. The least frequently mentioned reasons were lack of interest in their own health (4.7%) and insufficient knowledge on how to improve it (6.5%).
Health Status and Mental Health of Hungarian Homeless Service Workers Compared to the General Population.
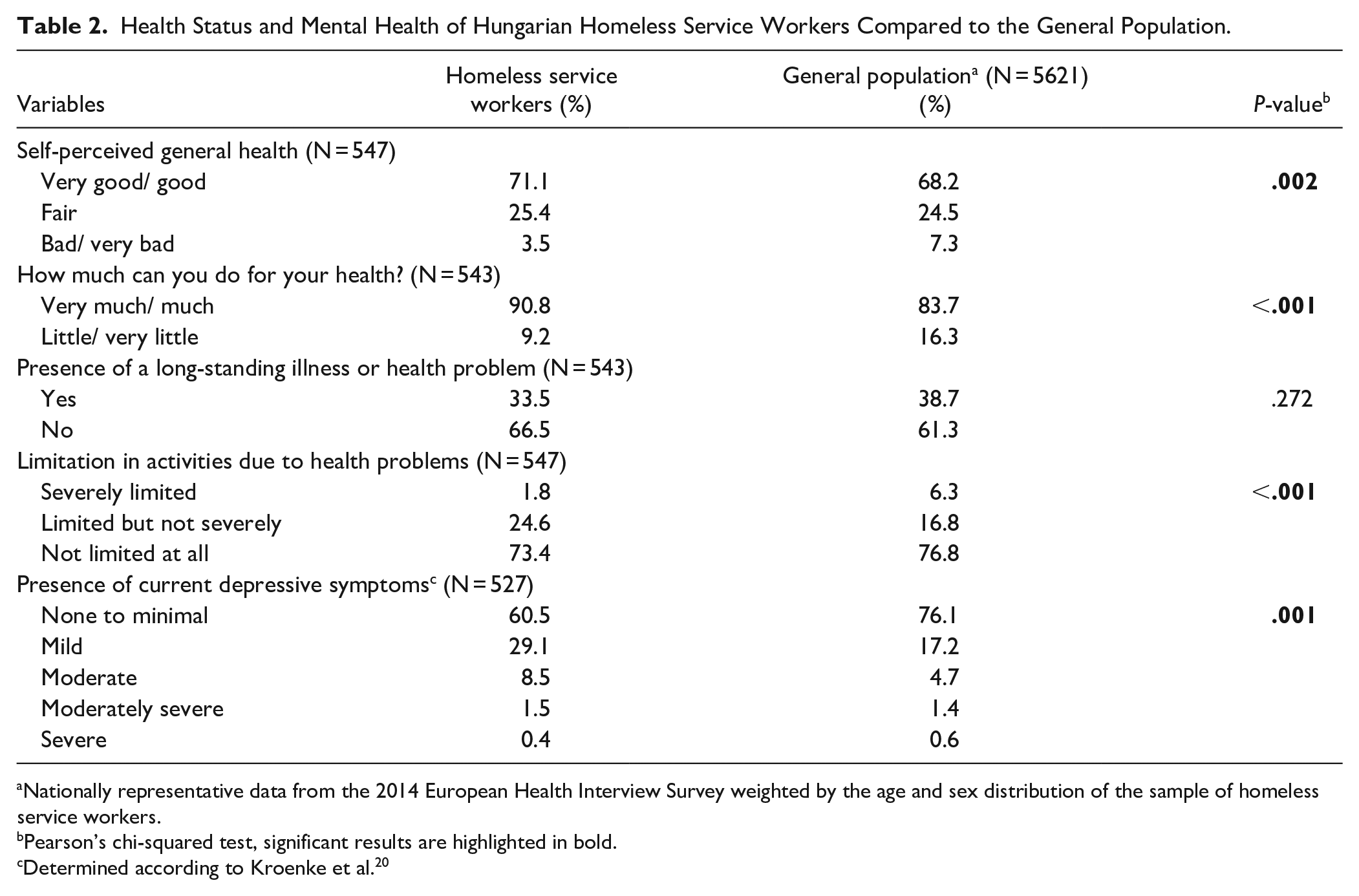
Nationally representative data from the 2014 European Health Interview Survey weighted by the age and sex distribution of the sample of homeless service workers.
Pearson’s chi-squared test, significant results are highlighted in bold.
Determined according to Kroenke et al. 20
Perceptions of the ability to influence one’s health also differed significantly (P < .001), with a higher proportion of service workers believing they could do very much or much to improve their health compared to the general population. Although the prevalence of long-standing health problems tended to be slightly lower among caregivers than in the general population, they experienced a higher prevalence of activity limitations due to health issues (26.4% vs 23.1%, P < .001). Nonetheless, one-third of homeless service workers reported having a long-standing illness or health problem, and for one-fourth, this resulted in some form of limitation in activities.
Mental Health
The PHQ-8 questionnaire results revealed a significant difference in the mental health status of frontline service workers compared to the general population (P = .001; Table 2). The prevalence of mild and moderate depressive symptoms was approximately twice as high among homeless service workers as in the general population. However, rates of moderately severe and severe symptoms were similar between the 2 groups.
Health Determinants
Based on self-reported weight and height data, there was no significant difference in the nutritional status of the 2 groups. However, the proportion of individuals with normal nutritional status tended to be lower among service workers compared to the general population (38.9% vs 45.3%) with a higher prevalence of obesity in frontline workers (26.9% vs 21.1%; Table 3). Nearly two-thirds of the caregivers (59.3%) were classified as overweight or obese. Similarly to the general population, 24 we observed a discrepancy between the perceived and calculated nutritional status among service workers, with many individuals who were living with overweight or obesity perceiving themselves as having the right weight. Thus, the rates of those who perceived themselves as overweight or obese were only 33.5% and 9.7%, respectively.
Health Determinants Among Homeless Service Workers in Comparison With the General Population in Hungary.

Nationally representative data from the 2014 European Health Interview Survey is weighted by the age and sex distribution of the sample of homeless service workers.
Pearson’s chi-squared test, significant results highlighted with bold.
Based on BMI calculated from self-reported weight and height data and categorized using standard ranges (WHO).
The frequency of fruit and vegetable consumption among homeless service workers differed significantly from that of the general population (P = .008 and .001, respectively; Table 3). The proportion of individuals who consumed fruits daily was considerably higher in the general population (57.0% vs 41.4%). Additionally, 10.5% of homeless service workers reported consuming fruits less than weekly or never. The prevalence of daily vegetable consumption was only 26.3% among homeless service workers, compared to 45.4% in the general population. Moreover, 16.4% of homeless caregivers consumed vegetables less than weekly.
The frequency of alcohol consumption also differed significantly between the 2 groups (P < .001), with a somewhat more favorable pattern observed among the service workers (Table 3). Less than 1% of service workers reported consuming alcohol daily, compared to 4.7% of the general adult population. Conversely, the proportion of those who reported drinking alcohol on a monthly basis was higher among frontline workers (35.8% vs 23.6%). Notably, slightly more than one-fifth of homeless service workers (21.1%) reported either not consuming alcohol at all during the 12 months prior to the survey or having never consumed alcohol.
A significant difference was observed between the two groups in the frequency of smoking (P = .003), though no significant difference was found in the overall current smoking status (P = .203; Table 3). The prevalence of current smokers tended to be higher among the caregivers than in the general population (36.9% vs 31.9%), with more caregivers smoking daily compared to the Hungarian adult population (35.4% vs 26.4%). Among daily smokers in the service worker group, the average cigarette consumption was 14 cigarettes per day (14.3 ± 6.2 cigarettes/day). Additionally, 30.2% of daily smokers were classified as heavy smokers, consuming at least 20 cigarettes per day.
Use of Health Care Services
The majority of individuals in both groups had visited their general practitioner (GP) during the year prior to the survey (Table 4), with no significant difference between the groups. However, the proportion of homeless service workers who had never visited their GP was more than 3 times higher than in the general population (1.8% vs 0.5%). Significant differences were observed in the participation in preventive services, particularly for blood pressure measurements and colorectal and cervical cancer screening (P < .001, P < .001, and P = .002, respectively). Among annual blood pressure, cholesterol, and glucose measurements, the participation rate for blood pressure measurement was notably higher in both groups compared to the other 2 tests. Despite this, only 85.8% of frontline workers reported participating in tuberculosis screening within the past 12 months. For all 3 organized cancer screenings, the participation rates among homeless service workers were higher compared to the general population, with cervical cancer screening having the highest participation rate in both groups. Still, the participation rates stayed below 50% for all screenings in both groups.
Use of Ambulatory and Preventive Care Services Among Homeless Service Workers in Comparison With the General Population in Hungary.
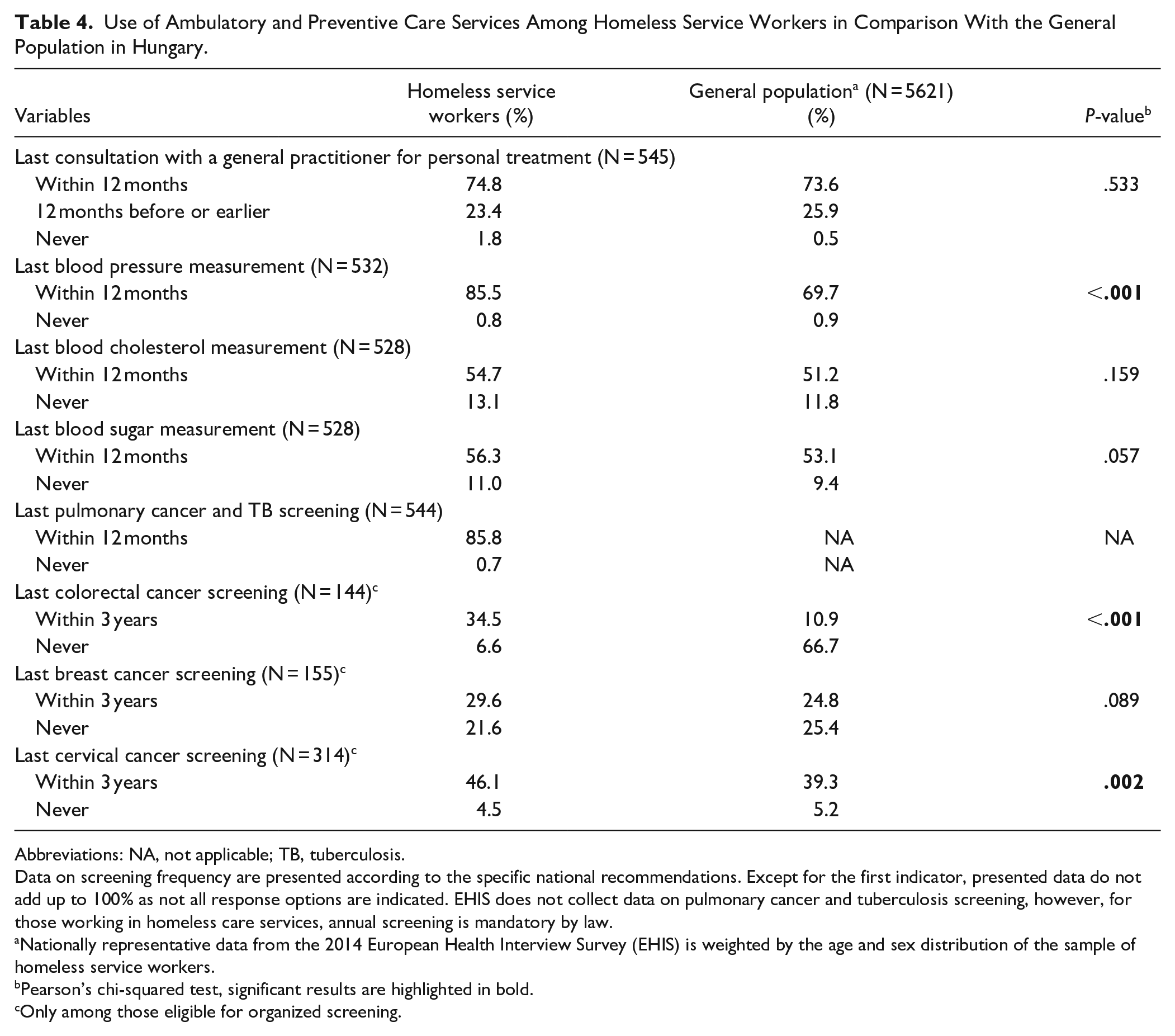
Abbreviations: NA, not applicable; TB, tuberculosis.
Data on screening frequency are presented according to the specific national recommendations. Except for the first indicator, presented data do not add up to 100% as not all response options are indicated. EHIS does not collect data on pulmonary cancer and tuberculosis screening, however, for those working in homeless care services, annual screening is mandatory by law.
Nationally representative data from the 2014 European Health Interview Survey (EHIS) is weighted by the age and sex distribution of the sample of homeless service workers.
Pearson’s chi-squared test, significant results are highlighted in bold.
Only among those eligible for organized screening.
Discussion
Health surveys targeting homeless service workers are scarce. 25 The current study provides new insights into the health status, health behaviors, and use of preventive services among frontline workers in homeless services, highlighting both challenges and opportunities for improving their health. Despite the demanding nature of their work, nearly 3-quarters of participants rated their health as good or very good. However, one-third reported having a long-standing illness or health problem, and one-fourth experienced limitations in daily activities due to health issues. These findings align with previous research suggesting that individuals’ self-assessments of health extend beyond their physical condition, encompassing a broader perception of well-being. 26 Qualitative studies have shown that health perceptions often include factors such as fitness and overall well-being. In our study, 99% of those who rated their health as “very good” had no depressive symptoms or only mild ones. This stable mental health appeared to outweigh the fact that 9.5% of those in “very good” health reported activity limitations and 8.4% had a chronic illness or health condition.
The high prevalence of limitations in performing activities of daily living among homeless service workers is concerning particularly if we consider that 71.3% of our sample were below the age of 50 years. This may be attributed to the physically demanding nature of work, the environmental conditions in which they operate, and the limited access to resources to address chronic conditions. Taking a closer look at the reasons for poor health reveals significant barriers, including limited time and financial resources, which prevent these workers from adequately addressing their health needs. These barriers underscore the complexity of maintaining health in a highly demanding work environment and reflect the broader systemic issues that could be addressed through policy interventions aimed at improving working conditions and better-supported access to healthcare services.
Our data confirmed known results that highlight elevated levels of psychological distress, including depression, among homeless service workers. 11 One of the most striking findings of the present study is the elevated prevalence of depressive symptoms among frontline workers, particularly mild and moderate depression, which was twice as high compared to the general population. The absence of a significant difference in more severe forms of depression may reflect either resilience in this workforce or self-reporting bias and underreporting due to the stigma associated with mental illness.27,28 These findings underscore the importance of implementing mental health support programs for homeless service workers, including counseling services and mental health screenings.
Our study also identified significant differences in health determinants, particularly regarding nutritional status and smoking habits. The higher prevalence of obesity among homeless service workers is notable, as obesity is a well-known risk factor for numerous chronic diseases. 29 Moreover, the low rates of daily fruit and vegetable consumption, coupled with higher rates of daily smoking, further exacerbate the risk of poor health outcomes in this population. The high rate of smokers suggests a potential coping mechanism for stress, which has been documented in other high-stress professions.30,31 These findings point to the need for targeted health promotion initiatives aimed at improving diet and reducing smoking rates among homeless service workers. Interestingly, our findings revealed a more favourable pattern of alcohol consumption among homeless service workers compared to the general population. Less than 1% of service workers reported daily alcohol use, markedly lower than in the general population. Additionally, over one-fifth of service workers reported either abstaining from alcohol entirely in the previous year or never consuming it at all. This lower rate of daily alcohol use suggests that, unlike smoking, alcohol may not be as prevalent a coping mechanism among this workforce, despite the high levels of occupational stress they face. These findings provide a positive note, indicating a potentially protective behaviour that contrasts with trends seen in the broader population and among other high-stress occupations.
Interestingly, while the use of preventive services was higher among homeless service workers for certain screenings, such as colorectal and cervical cancer, the overall participation rates remained low, particularly for organized screenings where participation should be higher given the high-risk nature of their work. The relatively low participation in tuberculosis screening is particularly concerning, as this screening is legally mandated for workers in homeless services. 21 Barriers to preventive care, such as limited time, may explain these discrepancies. Additionally, the finding that a small but significant proportion of workers had never visited their GP suggests potential gaps in access to primary healthcare, despite universal health coverage in Hungary. This gap could be addressed through workplace health initiatives that offer convenient, on-site health screenings and encourage regular check-ups.
This study has some limitations. First, the self-reported nature of the data, particularly for health behaviors such as smoking and alcohol consumption, may be subject to response bias. Additionally, the socio-demographic characteristics of the sample were quite specific. There was a high proportion of women and of those with a high level of education. Both gender and education are social determinants of health that may have influenced our results. They may also limit the generalizability of the study findings. However, the high rate of females and highly educated persons among social workers is a known phenomenon from previous studies.11,25 Also, we have weighted the EHIS data according to gender. However, the percentage of those who had high level of education was 3-times higher in our sample than in the EHIS survey. 32 Considering that there are 4 years between the 2 surveys, this may account for some of the observed differences in health status and health behaviors between the general population and the workers in homeless services. However, since changes in population health status and health behaviors typically occur to only a minor extent over a 4-year period, in the absence of major health reforms or health issues such as a pandemic, this limitation has minimal effects on the results and does not substantively impact the conclusions. Finally, our study did not assess physical activity levels among participants. Physical activity is a well-documented factor that not only influences nutritional status but also acts as a protective factor for mental health. 33 The inclusion of physical activity data could have provided a clearer understanding of the interventions needed to improve these aspects of health within this population. Although population-level data may indicate similar trends, direct assessment within our sample could have enhanced the precision of our findings.
Conclusions
The results of this study suggest that much is yet to be learned about the health status and behaviors of homeless service workers. Our study revealed a complex picture of resilience and vulnerability. While many workers perceived their health positively, significant barriers, including limited time and resources, hindered their ability to maintain optimal health. Elevated rates of obesity, smoking, and depressive symptoms suggest that targeted interventions, particularly in the areas of mental health and lifestyle modification, are urgently needed. The low participation in preventive services, especially in mandatory screenings, further highlights the need for improved access to healthcare for this population. Policymakers and local service managers should consider tailored workplace health programs that address both physical and mental health needs, as well as systemic changes to promote the health of homeless service workers.
Footnotes
Acknowledgements
The authors are incredibly grateful to the busy homeless service workers who took the time to complete the questionnaire. We also thank Zoltán Gurály for his assistance. Finally, we would like to thank Ildikó Tokaji,who is responsible for the EHIS survey at the Central Statistical Office in Hungary, for her continuous support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by University of Pécs.
Ethical Approval
This study was approved by the National Scientific and Ethical Committee (TUKEB) of the Medical Research Council of Hungary (registration number: 5547-2/2018/EKU).
Consent to Participate
Participants provided written informed consent expressing their willingness to participate in the study.
Consent for Publication
Not applicable.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.