
Abstract
El Paso Health Education and Awareness Team (EP-HEAT®) is a bilingual program focused on increasing health awareness and dispelling health-related misinformation in the U.S.-Mexico border region. EP-HEAT® consists of students, faculty, staff, and Promotoras. The primary objective of EP-HEAT® is to empower the community with healthcare resources in a culturally acceptable way. EP-HEAT® established the bilingual “In the Hot Seat with EP-HEAT®: Dispelling Myths in Healthcare” series commonly referred to as Myth Busters events. Community members were surveyed following the events. Our results showed the majority of EP-HEAT® event attendees identified as Hispanic and were older than 46 years of age. Following EP-HEAT® events, attendees felt comfortable teaching the information they learned to friends and family. Dispelling myths is instrumental for communities with limited access or knowledge of healthcare and diseases. EP-HEAT® events serve as a platform for evaluating the sources of community’s current health information, prevalence of healthcare myths, understanding the community’s health information needs, and disseminating accurate health information while dispelling myths in a culturally competent manner. Medical students need to become proficient in serving as educators, particularly in underserved areas. The skills developed by participating in EP-HEAT® myth-buster events provide information to the community while simultaneously providing opportunities for medical students to organize these events and allowing them to act as community-facing educators that may promote their professional identity development.
Keywords
Introduction
The digital age has made health information widely accessible via search engines, the media, and online social networks. However, with unprecedented exposure to information of varying quality, it has become increasingly critical to appraise information for accuracy correctly. In healthcare, the capacity for information to spread rapidly is a double-edged sword as it can mitigate the spread of disease through disseminating public health guidelines. On the other hand, the speed with information can be disseminated can also hinder these efforts if information is false or inaccurate. The COVID-19 pandemic and the corresponding “infodemic” are recent examples of the speed with which information can be disseminated, particularly surrounding the use of face masks, vaccination, or even the pandemic’s origins can be generated and spread.1,2
Multiple factors impact the endurance of misinformation and individual susceptibility to belief in false claims, including (1) the credibility of the message source; (2) the consistency of the message with prior beliefs; (3) emotionality; (4) deliberation time and “intuitive” thinking; (5) prior exposure to the false information; (6) health literacy; and (7) similarity to—or in-group affiliation with—the message source.3 -5 Additionally, well-intentioned efforts to correct misinformation can be ineffective or counterproductive.2,6,7 These challenges augment the damaging effect of misinformation as it can continue to exert influence over behavior, even after attempts to correct or debunk it. 4
Racial and ethnic minority groups have historically been plagued by health inequities, which make these populations additionally vulnerable to the consequences of misinformation— including disparities in health outcomes. For example, language barriers, poverty, lack of medical insurance, and limited access to preventative healthcare and chronic disease management have contributed to the Hispanic population being disproportionately affected by diabetes, obesity, and certain cancers.8,9 These factors, along with widespread misinformation, crowded living, and predominant fields of employment, also set the stage for the higher burden of COVID-19 infection, severe disease, and mortality that was experienced by minority populations during the COVID-19 pandemic.10,11
The Hispanic-majority border community, has borne the burden of these health disparities, which were further exacerbated during the COVID-19 pandemic and associated “infodemic.”3,12 According to the United States Census Bureau, 13 81.6% of the population in border cities is Hispanic or Latino, and the Texas Department of State Health Services 14 reports that 37.6% of the population is obese, 29.5% have hypertension, and 11% have been diagnosed with diabetes, conditions that predispose to worse health outcomes.
In response to the need for culturally competent and accurate health information, the El Paso Health Education and Awareness Team (EP-HEAT®), comprised of medical students and faculty, was established in 2020 with the mission of disseminating bilingual (English/Spanish) health education material to the border community. While initially an online platform during the COVID-19 pandemic, the success of the program in increasing knowledge of COVID-19 prevention, detection, and treatment, led to further expansion of the community outreach team to also include Community Health Workers or Promotoras de Salud,15 -17 herein after referred to as Promotoras. Promotoras are residents in the community which they serve, are fluent in the culture and language of the community, and have valuable social capital which, along with their health education and communication training, facilitate the delivery of culturally competent care and improve trust in the health care team.18,19 This unique role of liaison between the healthcare system and the community is additionally well-suited to disseminating accurate health information and dispelling myths. The literature supports the premise that efforts to correct misinformation may be more effective when delivered by a “trusted messenger” or peer with ties to credible sources, and that process of persuasion is enhanced by group affiliation with the source of the correction.4,19,20
Here we report on an expansion of EP-HEAT’s community outreach efforts into the realm of countering medical misconceptions and misinformation surrounding health topics such as immunizations, diabetes, heart disease, cancer, and digital literacy via the bilingual program “In the Hot Seat with EP-HEAT®: Dispelling Myths in Healthcare,” otherwise known as Myth Busters. 15 The goal of this project was to create a collaborative environment for community members, students, Promotoras, and healthcare experts to identify and dispel myths in healthcare while connecting the community to healthcare resources.
Methods
The pilot program consisted of interactive workshops, informational materials, and digital resources tailored to the linguistic and cultural needs of the community. By utilizing bilingual approaches, including both English and Spanish languages, the program aimed to reach a broader audience and enhance comprehension among diverse populations. Furthermore, culturally sensitive content was integrated to ensure relevance and resonance with the community’s values and beliefs. Guided by participatory action research (PAR) principles, community members were actively involved in shaping the program content, fostering a collaborative approach that strengthened its accessibility, relevance, and overall impact.
EP-HEAT® Member Composition
EP-HEAT® consisted of a multi-disciplinary, multi-institutional team. Specifically, members of EP-HEAT® included clinical and basic science faculty, Promotoras, and biomedical graduate and medical students. The students and Promotoras worked collaboratively to serve as the primary organizers of EP-HEAT® activities and liaisons between healthcare professionals and the community, while the faculty provided guidance and feedback. Students who participated in supporting the community events were awarded volunteer hours for their contributions.
Identifying Topics for Events
Healthcare topics were identified by Promotoras and students by direct contact with community members. Direct contact included door-to-door communication, outreach at local health fairs, and by speaking to attendees at other events. Commonly requested topics from community members included diabetes, hypertension, and viral infections (COVID-19 and influenza). Topics for the events can be found in Table 1.
Topics for the Events.

Planning and Advertising Events
Once a topic had been selected by community members, students identified and reached out to a healthcare expert who presented to the community. Healthcare experts were selected based on their specialty, availability, and willingness to serve as an unpaid presenter for the event. The community also requested Saturday mornings for the events as many work during the week and Sunday was reserved for religious purposes. The Promotoras served as the liaisons between the healthcare experts and community members, pinpointing questions and myths related to the identified topic. During the preparation for the event, students, together with the designated expert and Promotoras, constructed a presentation that focused primarily on the questions and/or myths related to the healthcare topic.
Additionally, students addressed technological requirements such as preparing microphones and projectors to present a PowerPoint to facilitate discussion. The Promotoras took the lead in inviting the community members to attend the event using bilingual (English/Spanish format) flyers designed by the students. These flyers were distributed to other Promotoras during conferences, to homes in the surrounding area, community health clinics, and amongst the student population. An overview of the event structure can be found in Figure 1.

Schematic of health education event planning and implementation. Once the healthcare topic and myths were identified by the community, students contacted a healthcare expert to present. As the event was planned, the Promotoras invited community members to attend. The event was set-up as a “pseudo talk show” with students addressing the healthcare topic myths, allowing the community members to openly ask questions. Since the event was held in English and Spanish, the Promotoras and/or students served as translators.
Overview of Bilingual Health Educational Events
To accommodate the working schedule of our community members, the events occurred Saturday mornings. The event was presented in a pseudo-talk-show manner, where students and Promotoras served as the hosts, interviewing the expert in the field in a bilingual (English/Spanish format) with the audience primarily being composed of the community members, along with students. At the end of each event, EP-HEAT® students distributed the paper surveys, ensuring the community members received English or Spanish versions, depending on community preference and answering any questions. Students also asked community members for ideas on topics for future events.
Surveying Community Members Attending Myth Busters Events
The community members who attended the events received a paper survey at the end of Myth Busters Events to obtain demographic data, mastery of topics, identify the motivation behind attendance, and evaluate the benefits and effectiveness of the event. These surveys were available in both English and Spanish (Supplemental File 1) to accommodate the community members.
Ethical Statement
The study was considered exempt (protocol number E22051) under Category 2: Research that only includes interaction involving the use of educational tests (cognitive, diagnostic, aptitude, and achievement), survey procedures, interview procedures or observation of public behavior (including visual or auditory recording) if at least one of the following is met: (i) Information obtained is recorded by the investigator in such a manner that the identity of human subjects cannot be readily ascertained, directly or through identifiers linked to the subjects. Children may only be included in research under this exemption when involving educational tests or observation of public behavior if the investigator(s) do not participate in the activities being observed and the information obtained is recorded by the investigator in such a manner that the identity of the human subjects cannot be readily ascertained directly, or through identifiers linked to the subjects; or (ii) Any disclosure of the human subjects’ responses outside of the research would not reasonably place the subjects at risk of criminal or civil liability or be damaging to the subjects’ financial standing, employability, educational advancement, or reputation. Children may only be included in research under this exemption when involving educational tests or observation of public behavior if the investigator(s) do not participate in the activities being observed and the information obtained is recorded by the investigator in such a manner that the identity of the human subjects cannot be readily ascertained directly, or through identifiers linked to the subjects; or (iii) The information obtained is recorded by the investigator in such a manner that the identity of the human subjects can be readily ascertained, directly or through identifiers linked to the subjects, and an IRB conducts a limited IRB review to make the determination required by 45 CFR 46.111(a)(7). Children may not be included in this section.
Results
The evaluation of the program included both qualitative and quantitative measures to identify the demographics of attendees and assess the program’s impact on knowledge acquisition, mastery of topics, attitudes toward health topics, and possible behavioral changes. Feedback from participants and stakeholders informed iterative improvements to the program, ensuring its relevance and sustainability in the community.
Demographic Data
The data was collected throughout events held between November 2021 and September 2023. Demographic data of event attendees is found in Table 2. The majority of participants were aged 46 years and older, representing 59.9% of the sample (118 out of 197 participants). The 40 to 45 years age group made up the second-largest segment, at 16.2% (32 participants). Participants aged 25 to 29 years accounted for 9.1%, while those aged 18 to 24 years made up 8.1%. The smallest groups were those aged 30 to 34 years (3.6%) and 35 to 39 years (3.0%).
Self-Reported Participant Demographics.

Most participants identified as Hispanic, comprising 87.4% of the total sample (187 out of 214 respondents). Caucasian participants made up 6.5% (14 respondents), and Asian participants accounted for 5.6% (12 respondents). There were no respondents identifying as African American or Native American, while 1 participant (0.5%) identified as “Other.” Some participants selected more than 1 racial identity, contributing to a total count above 214 responses.
In terms of educational background, 16.3% of respondents had no diploma, while 23.6% had a high school diploma or GED. Those with an associate’s degree represented the largest segment, at 25.0% (52 out of 208 respondents). Participants with a bachelor’s degree comprised 22.1% of the sample, and 5.3% had a master’s degree, while doctoral-level degree holders accounted for 7.7%.
Identification of Trusted Healthcare Sources
Participants were asked to select sources from which they obtained their medical information. Figure 2 illustrates the sources from which community members obtain their medical information and which sources they consider trustworthy. The most frequently cited source of medical information was physicians or nurse practitioners, with 67.9% of participants selecting this option. This source was also rated as the most trustworthy, with 84.7% of participants identifying it as a trusted source.
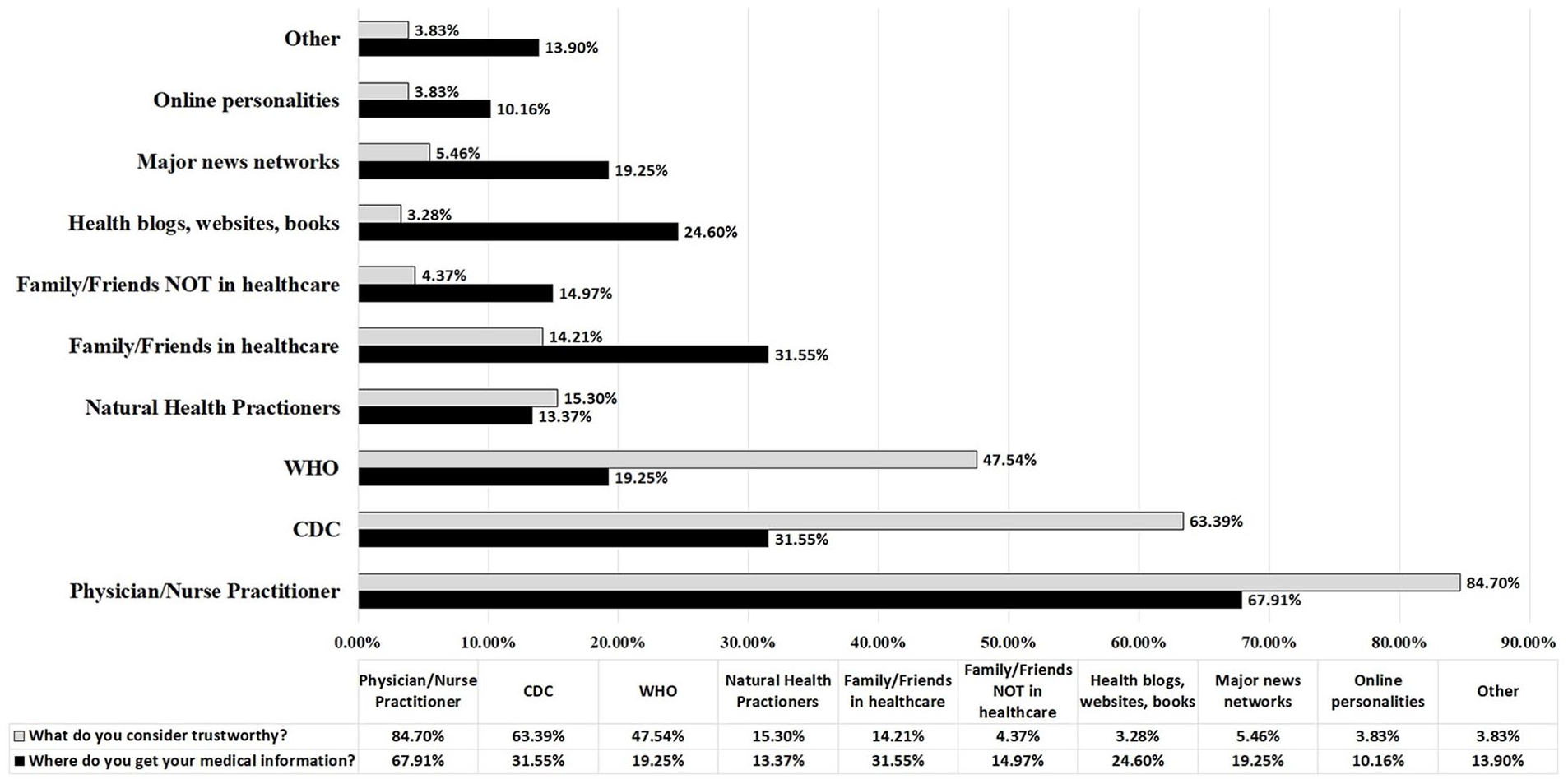
Community member sources and trustworthiness of medical information. Community members who attended the Myth Busters event selected various sources for medical information, including physicians/nurse practitioners (69%), CDC (31%), WHO (19%), and health blogs/websites/books (24%). When evaluating the validity of claims, 77% seek supporting evidence, 47% consult perceived experts, 24% look for explanatory videos, 16% find evidence weakening the claim, and 15% refer to debunking articles.
The Centers for Disease Control and Prevention (CDC) was the second-most trusted source, with 63.4% of participants considering it reliable, while 31.6% reported it as a source of medical information. The World Health Organization (WHO) followed, being viewed as trustworthy by 47.5% of respondents, though only 19.3% reported using it as a source.
Other sources included natural health practitioners (13.4% use; 15.3% trust), family or friends in healthcare (31.6% use; 14.2% trust), and family or friends not in healthcare (15.0% use; 4.4% trust). Additional sources like health blogs, websites, and books (24.6% use; 3.3% trust), major news networks (19.3% use; 5.5% trust), online personalities (10.2% use; 3.8% trust), and other sources (13.9% use; 3.8% trust) had lower levels of trustworthiness reported.
Overall, the data highlights a strong preference and trust in professional medical sources, particularly physicians, nurse practitioners, and reputable health organizations, over informal or non-professional sources. This trend suggests that community members value authoritative sources for medical information, although a notable percentage still relies on less traditional sources.
Attendee Motivation, Perceived Impact, Knowledge Gain, and Teaching Comfort From Health Education Events
Figure 3 summarizes attendee motivations for participating in health education events, as well as their perceptions of the events’ impact on knowledge and comfort with teaching the topics discussed. As demonstrated in figure 3a, the primary reason for attendance was interest in the topic, as reported by 75 attendees. This was followed by a desire to gain more information in general (54 attendees) and encouragement from friends or family (46 attendees). Fewer attendees cited dispelling misinformation (15 attendees) or other reasons (13 attendees) as their primary motivation for attending.

Community member impact of attending events. (a) Participants attended Myth Buster events because they found the subjects interesting (50%), wanted more information (35%), were brought by a family member or friend (29%), or wanted to address misinformation (9%), (b) Approximately 69% strongly agreed that these events helped dispel myths, (c) Additionally, 74% strongly agreed that the presentations increased their knowledge, and (d) 57% of attendees felt comfortable teaching the topic back to someone else.
When asked if the event helped attendees identify and dispel healthcare myths, a majority (69%) agreed, while 26% strongly agreed. A small percentage (5%) were neutral, indicating that most participants felt the event was effective in clarifying misconceptions (Figure 3b). When asked if attendees would attend more events, 73% strongly agreed that they would attend future Myth Buster events (data not shown), and 80% of surveyed participants strongly agreed that they would recommend the Myth Buster presentations to a friend or family member (data not shown).
Nearly all attendees reported an increase in knowledge as a result of the event (Figure 3c). Out of 152 attendees who answered the survey question, 114 attendees strongly agreed that the event enhanced their understanding, and 35 attendees agreed (Figure 3c). Only 3 attendees were neutral, and no attendees disagreed or strongly disagreed, demonstrating a strong consensus on the educational benefit of the event (Figure 3c). When considering mastery of the expected learning outcomes for presentations, 92% of participants agreed or strongly agreed that mastery was obtained (data not shown).
Attendees also reported their comfort level in teaching the topic to others. As demonstrated in Figure 3d, the majority (57%) felt very comfortable, while 30% felt comfortable. About 11% were neutral, and a small minority (2%) reported feeling not comfortable with teaching the material, suggesting that most attendees left the event feeling confident in their grasp of the topic.
Discussion
In border communities, access to accurate healthcare information is critical, yet often hindered by linguistic and cultural barriers, leading to widespread misinformation and disparities in healthcare outcomes. This study presents the development of a bilingual health education program aimed at addressing misinformation prevalent in a border community context. Grounded in community engagement and participatory action research principles, the program was designed collaboratively with local stakeholders, including healthcare professionals, community leaders, and residents.
With a majority of Hispanic population, a city can easily become the target of health misinformation. Health misinformation can contribute to increased health disparities and decreased health outcomes. It was the focus and aim of this program to tackle health misinformation by working with community members, Promotoras, and providing a forum where the general population could learn accurate and trustworthy information. When assessing the success of the events, it was shown that a majority of those who participated strongly agreed that attending helped them to dispel inaccurate health information. It is important to understand what caused this shift in perspectives in order to potentially recreate similar results in future studies.
Our study employed persuasive methods similar to those often used in the spread of misinformation, such as using relatable narratives, using the appropriate language (bilingual platform) and leveraging trusted community voices, to effectively disseminate accurate and reliable medical information. By framing messages in ways that resonated with the community’s beliefs and values, utilizing engaging storytelling techniques, and ensuring that information came from respected local figures, we aimed to enhance trust, encourage retention of information, and inspire positive behavioral change. This approach helped make scientific and medical content more accessible, memorable, and impactful for the audience.
In addition, this program strived to emphasize the importance of utilizing reliable sources and fostering a trusting relationship with healthcare providers. According to survey results, a majority of participants rely on their medical providers for healthcare information. This may be, in part, because of the way healthcare professionals are viewed. In a 2018 Gallup study, Americans rated Nurses, Medical doctors, and pharmacists as having high ethical standards. To enhance the credibility of our presentations, we carefully selected local physicians and faculty, who are well-versed in their respective fields. Additionally, the collaborative efforts alongside Promotoras proved to be instrumental in fostering community involvement, acting as an “in-group” link between the medical professionals and students, and effectively bridging the gap.
Juxtaposed to these findings is the apparent mismatch between the sources from which people gather their medical information and those they find trustworthy. Only 14% of respondents view information from family and friends as reliable, yet 32% rely on these sources for their medical information. About 3% of respondents view information from Health blogs and websites as trustworthy, yet 25% use these sources for their medical information. This discrepancy raises the question of why people turn to authorities that they do not consider trustworthy for their medical information. This is a potential inquiry for future research.
It is crucial to acknowledge the potential limitations of our survey, especially concerning the size of the surveyed population. We must note that certain races, such as African Americans and Native Americans, were not adequately represented in the data collected. Also, the positive feedback could have unintentionally influenced participants to return to future events and retake the survey, leading to a response bias. This emphasizes the importance of considering participant bias.
Ultimately, this bilingual health education program represents a proactive approach to identifying and addressing misinformation in healthcare within border communities. By fostering collaboration, cultural relevance, and empowerment, the program aims to mitigate disparities and improve health outcomes among underserved populations. Future research will explore scalability and long-term impacts, with the ultimate goal of promoting health equity in border regions and beyond.
This study and program serve as a valuable blueprint for institutions or organizations looking to establish a comprehensive multi-disciplinary team that collaborates with local communities to ensure accurate healthcare information is accessible to underserved populations.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241311145 – Supplemental material for Developing a Bilingual Health Education Program to Identify and Address Healthcare Misinformation in a Border Community
Supplemental material, sj-docx-1-jpc-10.1177_21501319241311145 for Developing a Bilingual Health Education Program to Identify and Address Healthcare Misinformation in a Border Community by Sara Mansour, Nathan Holland, Sergio Saucedo, Amadeus Ramirez, Mariela Lane, Joshua Salisbury, Komal Marwaha, Lorena Fernandez, Jesse Allen, Veeravenkata Garikiparthy, Patricia Rodriguez, Laura Renovato, Maria Land, Ricardo Belmares and Jessica Chacon in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We want to thank our community members for participating in the research study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the Myth Busters events was provided by AstraZeneca, AT&T, ADP, and Wells Fargo, and Underserved Communities Foundation; This pilot project served as JC’s Harvard Macy “Program for Educators in Health Professions” 2022 to 2023 Project. We thank the community members who attended the events.
Ethical Approval and Informed Consent
This study was considered IRB exempt (IRB# E22051).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.