
Abstract
Introduction:
Drug-resistant Neisseria gonorrhoeae is an urgent threat to public health. Novel prevention and treatment strategies are emerging, including immunizations, pharmacologic post-exposure prophylaxis, rapid molecular resistance assays, and novel antibiotics. However, where and how such strategies are optimally implemented remains unclear.
Methods:
We conducted a retrospective interrupted time series analysis of gonorrhea cases reported to the Massachusetts Department of Public Health. We collected names of treating providers from 2011 (n = 100) and 2022 (n = 108), and cross-referenced provider names with publicly available records from the Massachusetts Boards of Registration in Medicine and Nursing to identify provider type, specialty, year of terminal degree or licensure, and clinic type.
Results:
Of 208 providers, 111 (53.4%) were advanced care practitioners. Providers treated cases predominantly in community health centers (n = 65, 31.3%) and emergency departments or urgent care centers (n = 60, 28.8%). Only 11 (12.4%) of 89 physicians were trained in either adult or pediatric infectious diseases.
Conclusion:
Our results indicate that the majority of gonorrhea cases in the Massachusetts are treated in non-specialty settings. The time is now to plan for implementation of the emerging strategies to avoid underutilization and assure uptake of interventions in settings positioned to reach persons diagnosed with gonorrhea who will benefit most.
Keywords
Introduction
Drug-resistant Neisseria gonorrhoeae is 1 of the top 5 urgent antimicrobial resistance threats to public health. 1 Strains harboring high-level ceftriaxone resistance (minimum inhibitory concentrations [MIC] ≥ 1 µg/mL) have achieved sustained international transmission, including to the United States, 2 and the incidence of gonorrhea has climbed to levels not seen since the 1980s. 3 Therefore, clinicians are increasingly likely to encounter cases failing treatment, and will need novel strategies for gonorrhea control.
Fortunately, novel prevention and treatment strategies are emerging. Use of already licensed meningococcal B vaccines may partially cross-protect against Neisseria gonorrhoeae acquisition. 4 Doxycycline post-exposure prophylaxis (doxy-PEP) prevents infection from susceptible strains, although its efficacy in preventing Neisseria gonorrhoeae infection appears to be less than for Chlamydia trachomatis or Treponema pallidum infection.5 -7 Rapid detection of genetic resistance markers permits use of existing alternative antibiotics (also known as resistance-guided therapy). 8 Sexually transmitted diseases treatment guidelines from the United States, the United Kingdom, and Australia permit use of resistance-guided therapy for the treatment of N. gonorrhoeae infection when molecular resistance assays are available.9 -11 Commercial resistance assays are available in Europe and Australia; however, no Food and Drug Administration approved assay is yet available in the United States. Finally, novel antibiotics are in late-stage development, 12 which might provide diversified therapeutic options if approved for the treatment of gonorrhea. One novel antibiotic, zoliflodacin, recently demonstrated non-inferiority to ceftriaxone in a phase III clinical trial. 13
Implementation of those emerging strategies requires careful consideration in order to ensure sufficient uptake to effectively combat both the emergence of antimicrobial resistance and the spread of infection. For example, a recent modeling study demonstrated that resistance-guided therapy has the potential to extend the lifetime of other antibiotics (including ceftriaxone), when uptake is above 50%. 14 However, antimicrobial resistance can easily be viewed as under the purview of specialty providers, resulting in under-deployment of essential mitigation strategies. Understanding of which provider types treat cases of gonorrhea, and their practice locations can facilitate targeted interventions such as education and systems-level planning to optimize uptake.
Methods
To identify where implementation of novel prevention and treatment strategies would have the greatest impact, we conducted a retrospective interrupted time series analysis. We reviewed cases of gonorrhea reported to the Massachusetts Department of Public Health during 2 time periods. We collected names of treating providers in 2011 (n = 100 sampled consecutively) and 2022 (n = 108 sampled randomly). We permitted repeat providers as that was felt to represent the proportion of cases presenting to their practice.
We then cross-referenced provider names with publicly available records from the Massachusetts Boards of Registration in Medicine and Nursing. We extracted data on provider type, which included medical doctor, doctor of osteopathy, registered nurse, or other advanced care practitioner (nurse practitioner, family nurse practitioner, advanced registered nurse practitioner, certified nurse practitioner, or physician assistant). We also collected data on provider specialty, year of terminal degree or licensure, and clinic type. We categorized clinic type into the following domains: emergency department or urgent care center, hospital-based clinics, community health center, specialty clinics (sexually transmitted diseases (STD), HIV, or family planning clinics), private practice (which also included group practices or health maintenance organizations), school clinics, or military/job corps clinics.
We report relative frequencies of the providers who treated cases of gonorrhea among each covariate of interest, aggregated, and split by analysis time periods. We also report chi-square and fisher exact tests of significance for between time-period comparisons. We conducted all data analyses in STATA version 17.0 (StataCorp LLC., Texas, United States).
Results
Overall, of the 208 providers across both time periods (Table 1), 111 (53.4%) were advanced care practitioners. Providers treated cases predominantly in community health centers (n = 65, 31.3%) and emergency departments or urgent care centers (n = 60, 28.8%); only 30 (14.4%) providers treated cases in specialty settings (eg, sexually transmitted diseases (STD), HIV, or family planning clinics). Eleven (12.4%) of 89 physicians were trained in either adult or pediatric infectious diseases.
Characteristics of Providers Treating Individuals Diagnosed with Gonorrhea in Massachusetts: 2011 and 2022.
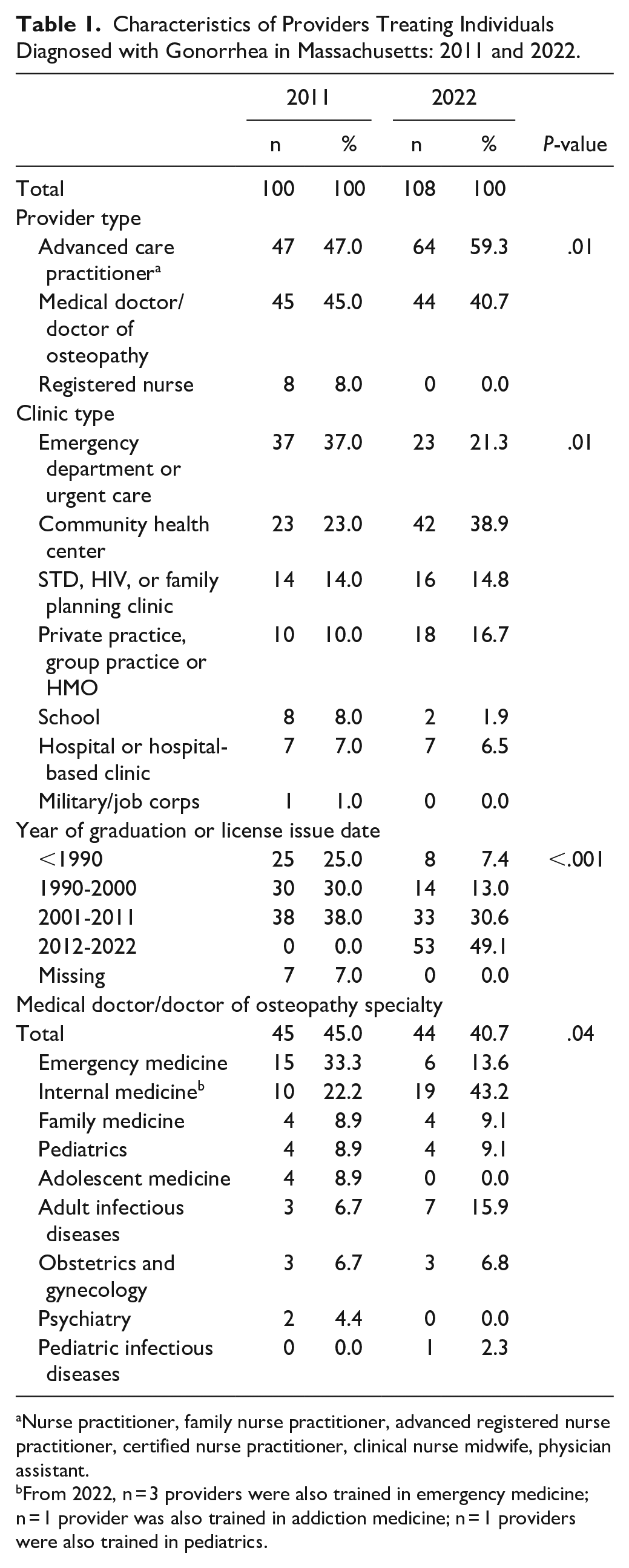
Nurse practitioner, family nurse practitioner, advanced registered nurse practitioner, certified nurse practitioner, clinical nurse midwife, physician assistant.
From 2022, n = 3 providers were also trained in emergency medicine; n = 1 provider was also trained in addiction medicine; n = 1 providers were also trained in pediatrics.
In 2022, more providers treating cases of gonorrhea practiced in community health centers (38.9%) than in 2011 (23.0%); conversely, more providers in 2011 practiced in emergency departments or urgent care centers (37.0%) than in 2022 (21.3%). More providers in 2022 who treated cases of gonorrhoeae were advanced care practitioners (59.3%) compared to 2011 (47.0%). Fewer providers in 2022 (7.4%) compared with 2011 (25.0%) graduated or were issued licenses before 1990 when gonorrhea incidence was higher.
Discussion
We retrospectively evaluated the type of providers who treated cases of gonorrhea in Massachusetts, and in what settings such treatments occurred in Massachusetts. Our results indicate that the majority of gonorrhea cases in Massachusetts were treated in non-specialty clinic settings, which is consistent with limited national data. 15 As such, it is essential to ensure that gonorrhea prevention and drug-resistant gonorrhea treatment are not viewed as the purview of specialists.
A similar “purview paradox” arose with pre-exposure prophylaxis (PrEP) for HIV. PrEP was viewed by primary care providers as the purview of HIV specialists experienced in antiretroviral prescribing, and by specialists as the purview of primary care providers who saw more individuals who were HIV negative but at high risk for HIV exposure; that paradox led to underutilization of HIV PrEP and missed opportunities to prevent new HIV infections. 16 Forthcoming strategies for combating gonorrhea will have limited effect if nuanced care of infection is restricted to specialists.
Lessons learned in overcoming the PrEP purview paradox emphasized the need for task shifting from specialist to primary care providers. 17 Such task shifting included the use of “PrEP navigators” to help patients understand and access the services they required. 18 There was also recognition of (a) the need for further training among primary care providers,17,19 and (b) the challenges imposed by geographical barriers, whereby the distance between service user and provider directly limited a patient’s ability to access PrEP. 20 Finally, PrEP implementation interventions emphasized the need to design services based on needs to patients. 21
Similar approaches can be used for the emerging interventions to prevent gonorrhea and worsening rates of antimicrobial resistance. Fortunately, the principles behind such tools are not new to emergency and primary care, nor unique to gonorrhea. Preventive vaccinations are more commonly delivered in primary care (eg, vaccination against human papilloma virus or hepatitis B). The same is now true for HIV pre-exposure prophylaxis after substantial efforts to increase provision in primary care. 22 In emergency departments and urgent care, post-exposure immunizations, such as tetanus toxoid-containing vaccine, are routinely given in the setting of contaminated wounds. 23 During the SARS-CoV-2 pandemic, strategies were developed to leverage emergency departments to increase the anti-SARS-CoV-2 vaccine coverage. 24 Emergency departments also are key sites for delivery of pharmacologic post-exposure prophylaxis, such as for HIV. 25 Antimicrobial stewardship is becoming standard of care in the outpatient setting. 26 Even resistance-guided therapy is being practiced in certain contexts (such as for predicting methicillin-resistant Staphylococcus aureus carriage or guiding treatment of Helicobacter pylori infection). Thus, the settings that most commonly treat patients with gonorrhea are already familiar with the principles behind emerging tools that will be essential for its control.
Doxy-PEP is the first of the above interventions to become widely available and recommended. 27 The guidelines from the Centers for Disease Control and Prevention avoid limiting implementation to any single setting. However, identification of best practices to implement doxy-PEP in emergency departments or urgent care centers remains unclear, particularly as individuals eligible for doxy-PEP require follow-up as well as a host of comprehensive sexual health care interventions that may be challenging to complete in a single acute-care visit. Resistance guided therapy using ciprofloxacin is permitted under the 2021 Centers for Disease Control and Prevention treatment guidelines among asymptomatic patients; 9 however, as no commercial assays are available, uptake has been slow. There are potentially only a handful of centers in the United States currently offering the molecular test for ciprofloxacin resistance. 28
To facilitate appropriate use of the tools currently available, and to ensure the next iteration of interventions reach patients who will benefit in as timely a manner as possible, development and dissemination of guidance, tailored specifically to busy emergency departments, urgent care centers, and primary care providers who have many competing clinical priorities is needed. In that context, it is notable that the first strain of Neisseria gonorrhoeae showing resistance to extended-spectrum cephalosporins and azithromycin in the United States was identified in primary care at a community health center. 2 While that health center is embedded within a unique network of community health centers in Massachusetts that may be better positioned to identify resistant strains as they emerge, it still serves to emphasize the point that antimicrobial resistance in N. gonorrhoeae will likely impact all clinic types in which cases of gonorrhea are treated.
Electronic decision support tools can augment antimicrobial stewardship when new therapeutic options are on the market. 29 Further, once available, universal access to the above prevention and treatment methods must be assured to mitigate health inequities. Data from Massachusetts between 2018 and 2022 consistently report that more than 70% of gonorrhea cases are among individuals with moderate to high social vulnerability. 30 Establishing standards for health insurance coverage of those strategies will be essential to promote early and equitable uptake.
Our study has several limitations. First, the study was retrospective in nature, using a relatively small sample size, thus limiting the precision of our findings. Second, this study was conducted within a single state, potentially limiting generalizability. Further, using date of licensure as a surrogate for experience is inherently flawed, and should be interpreted with caution. However, given that our findings were congruent with what limited national data exist, we feel those limitations do not negate the validity of our results.
Understanding where and by whom gonorrhea is being treated can inform training and capacity building efforts in a community-centric model, leveraging the lessons learned from the HIV PrEP purview paradox. Preemptive planning when novel prevention and treatment tools are becoming available may support optimization of uptake and avoid the mistakes of the past. Thus, the time is now to plan for the implementation of strategies that hold the promise of preventing the continued rise of untreatable gonorrhea.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Allergy and Infectious Diseases Award Number K23AI182453 to LAB. This work was also supported by CDC RFA PS20-2004, National Network of STD Clinical Prevention Training Centers. The authors would also like to acknowledge Laura Smock and Heather Elder for their support in data acquisition and analysis, as well as Janine Dyer for project coordination.
Ethical Approval
As all data used were obtained from either public health disease surveillance or public records, the Massachusetts Department of Public Health Institutional Review Board determined the study did not constitute human subjects’ research.