
Abstract
Background:
Angiosarcomas are rare tumors that can be difficult to diagnose due to subtle changes in the vascular endothelium. When there is evidence to suggest malignancy, such as a pathologic fracture, further investigation is needed, and a high suspicion for angiosarcoma needs to be present so that appropriate immunohistochemical stains are utilized on biopsied tissue. In situations where such suspicion is high and prior biopsies have been negative, performance of splenectomy, can be both diagnostic and therapeutic when splenomegaly is present.
Case Report:
This is a case of a 52-year-old woman with splenomegaly, initially attributed to infection, in the setting of upper respiratory symptoms and thrombocytopenia. Three months later, however, she presented with back pain. Imaging showed lytic bone lesions with pathologic vertebral fracture and numerous liver lesions that were too small to characterize further. Initial biopsies of the liver and bone did not reveal a pathologic process. Several months later, still without a unifying diagnosis, she presented to our institution. MRI of the brain was done for neurologic concerns and showed pathologic enhancement in the calvarium. A PET scan showed diffuse avidity of the skeleton and spleen. After discussing the case with a hematologist, splenectomy was performed for both diagnostic and therapeutic purposes. Angiosarcoma was identified in the spleen and in a PET-directed bone biopsy. With a definitive diagnosis, she returned home and subsequently elected to pursue hospice care.
Conclusion:
When there is a high clinical suspicion for malignant angiosarcoma, a multidisciplinary approach is necessary to direct both tissue acquisition and necessary histochemical staining.
Introduction
Angiosarcomas are a group of malignant vascular sarcomas with an incidence of approximately 1 in 1 million (NCI data: Angiosarcoma—NCI (cancer.gov)). They originate within many different organs, have different behaviors, and have a poor prognosis with limited treatment options. Due to their microscopic subtlety and infiltrative nature, they can be challenging to diagnose. Delays in diagnosis can lead to widespread disease that is not amenable to surgical resection.
To diagnose angiosarcoma, a high index of suspicion needs to be present. Additionally, in a patient with suspected malignancy and splenomegaly, splenectomy may be both diagnostic and therapeutic and should be considered. Here we present a unique case of widely metastatic angiosarcoma where the diagnosis was not evident until splenectomy was performed.
Case Report
We present a case of a 52-year-old Caucasian woman who presented to our institution’s Undiagnosed Mass Clinic (UMC) several months after a pathologic fracture which defied diagnosis. The UMC uses the expertise of specialty general internists at our tertiary care medical center to help patients to obtain a definitive diagnosis when the possibility of malignancy exists based on the imaging and clinical picture. This patient requested an appointment in our institution and was triaged to the UMC for evaluation.
In her initial evaluation, a thorough history was taken, with particular attention to risk factors for malignancy, and a physical examination was performed. She had a history of papillary thyroid carcinoma but had no history of, nor concern for, recurrence. She was in her usual state of health before waking with a sore throat and cough 4 months prior to presenting to our clinic. With the start of her symptoms, she also noted swelling in her abdomen. She went to her primary care provider who identified thrombocytopenia and splenomegaly on the evaluation. A computed tomography (CT) scan of the abdomen and pelvis was performed locally, which showed splenomegaly with attenuations too numerous to count, consistent with and infiltrative process, such as lymphoma or malignancy. No biopsies were done at that time.
Approximately 3 months later, she went to an emergency department with severe back pain and the inability to walk. She was admitted to the hospital with a pathologic fracture of the thoracic spine. Imaging performed at that time included an MRI of the thoracic and lumbar spine. This showed a pathologic fracture at T11 and widespread bony and numerous liver lesions, consistent with metastatic disease. During admission, she underwent a biopsy of the thoracic spine and of the liver. Both biopsies showed benign tissue with no specific diagnosis rendered. This was followed by a bone marrow biopsy that did not demonstrate malignancy, nor any other diagnosis.
Approximately 4 months from her initial presentation, she was seen in the UMC. We reviewed the above history. In addition, she reported a recent onset of new weakness and presented in a wheelchair. On physical exam, the spleen was palpable and there was diffuse abdominal tenderness. Right lower extremity patellar deep tendon reflex was not able to be elicited. No lymphadenopathy was noted. Given the new onset of weakness, a brain MRI was performed. While there were not any abnormalities of the brain, the calvarium and other visible bones showed lesions consistent with metastases.
Next, we performed a positron emission tomography (PET) scan (Figure 1) which showed diffuse involvement of multiple organ systems, with an infiltrative process that involved the spleen, liver, lymph nodes, and axial skeleton. The differential diagnosis included sarcoma or lymphoma. Complete blood count (CBC) at the time showed a hemoglobin of 7.0 g/dL, platelet count of 117 000 and elevated white blood cell count at 11.7 × 109/L. Although the CBC was consistent with hypersplenism (low platelet count), the peripheral smear showed hyposplenism, suggesting poor splenic function. Based on the PET scan, a biopsy was performed of the iliac crest bone was performed as this was the most avid and available site. Fine needle aspiration samples were immediately reviewed and deemed nondiagnostic. Tissue core samples were also obtained for review.

Representive image from the PET scan showing avidity in the thoracic spine (circled) and spleen with a focal liver lesion.
While the bone biopsy was still pending, splenectomy was performed for symptomatic relief and for diagnostic purposes, based on a recommendation from a hematologist. Intraoperatively, the spleen was remarkably abnormal and intraoperative photos were taken (Figure 2). Gross examination of the spleen showed a 29 cm × 18 cm × 14 cm spleen. On cross sectioning, the spleen appeared diffusely mottled and heterogeneous with a nodular, hemorrhagic and yellow cut surface (Figure 3). Microscopically, the sections of the spleen showed spindle cells with abnormal nuclei and prominent nucleoli (Figures 4 and 5). The preliminary diagnosis on frozen section was a spindle cell neoplasm, favor malignant. Immunohistochemical staining of the sections showed the tumor cells to be positive for CD31 and ERG (Figure 6) and negative for desmin, CD21, CD35, S100, and keratin AE1/AE3. In situ hybridization for EBV was also negative. This was confirmed on the bone biopsy that had still been pending at the time of surgery (Figure 7).
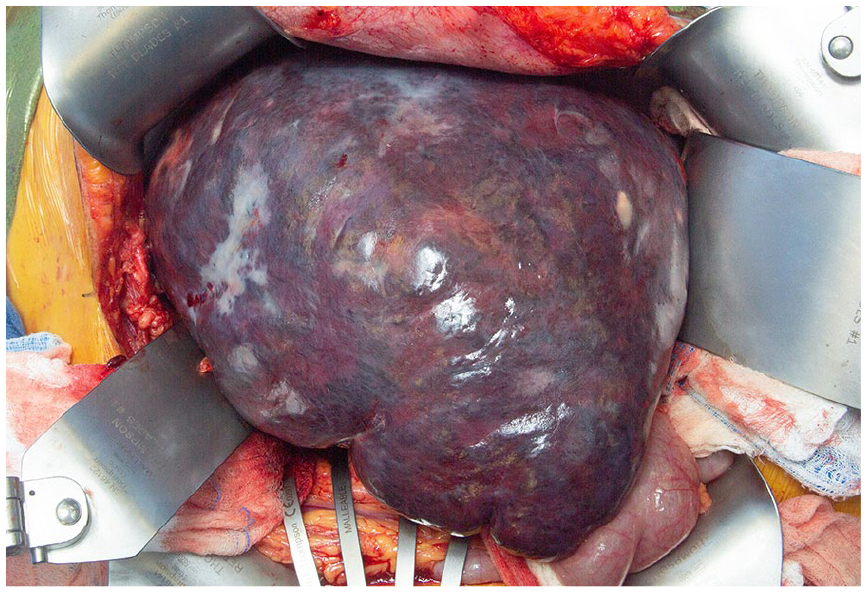
Intraoperative photo of the enlarged, abnormal spleen.

Image from a cross-section of the spleen at the time of gross examination. Circled are lesions noted at the time of sectioning.
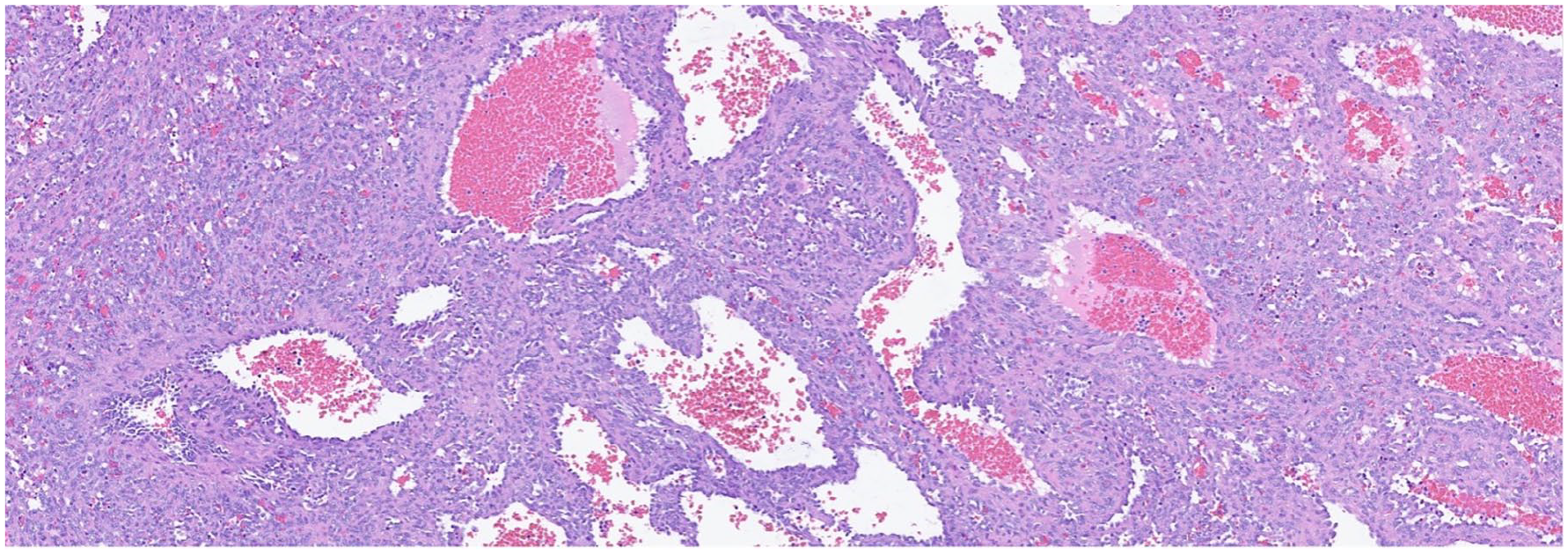
Medium power (20×) microscopic images of the spleen showing a cellular vasoformative proliferation with luminal blood.

Higher magnification (40×) views disclose nuclear atypia (circled).

Low magnification (10×) views of the Erythroblast transformation specific related gene (ERG) immunostain highlighting endothelial differentiation thus helping establish a diagnosis of angiosarcoma.

Medium power (20×) views of CD31 also highlighting vascular differentiation of malignant cells.
Three days after hospital discharge from splenectomy, the patient was able to get formal oncology opinion. Afterwards, she was able to return home for ongoing care with her local care team. Her local oncologist found her ineligible for clinical trials. She was referred to hospice and died 5 months following her diagnosis of angiosarcoma.
Discussion
This is a case of angiosarcoma that presented with distant metastases. Angiosarcoma can be challenging to diagnose and, as with many sarcomas, definitive diagnosis is often delayed. Once diagnosed, the prognosis of angiosarcoma is poor. Median survival for patients with metastatic disease is 12 months. 1 The treatments are not well-established, but usually involve systemic chemotherapy for metastatic disease, while localized disease may have a curative approach with surgery followed by radiation therapy. 2 Given the origin of angiosarcoma in the blood vessels, containment can be difficult as hematogenous spread is common.
In this case, the patient had symptoms of pathologic fracture and symptomatic splenomegaly for months prior to the diagnosis. Prior to her presentation at our institution, she had multiple biopsies which did not reveal the diagnosis. At our tertiary care medical center, PET-guided iliac crest bone biopsy was, further, preliminarily nondiagnostic prior to the splenectomy. As the bone biopsy tissue review was still pending at the time of surgery, the benefit of review of both specimens was had. Therefore, splenectomy, performed for both therapeutic and diagnostic purposes, was led to a diagnosis. Splenic angiosarcomas are rare, and, although splenic angiosarcomas present with splenomegaly, we are unable to say that our patient’s metastatic disease originated in the spleen. There is sparse literature on primary splenic angiosarcoma. It is predominantly in the form of case reports. 3
We were able to secure a diagnosis for this patient through our newly created Undiagnosed Mass Clinic that is led by general internists with expertise in diagnostic dilemmas and complex medical care. This clinic exists in the context of a large, integrated, multispecialty group practice with advanced diagnostic capabilities. This integrated model allowed us to use multispecialty expertise in internal medicine, diagnostic radiology, hematology, and pathology to determine this patient’s diagnosis of angiosarcoma. With the benefit of multiple integrated specialty teams, including general internal medicine, hematology, surgery, and oncology, collaboration offered a diagnostic pathway. In this case, curbside consultation with a hematologist regarding the splenomegaly and cytopenias led to a diagnostic and therapeutic splenectomy.
Generally, angiosarcomas have a poor prognosis. In a retrospective study looking at different primary sites of angiosarcoma, those with metastatic disease at the time of diagnosis had a 5-year survival rate of 0.1. 1 A review of over 4500 cases of angiosarcoma using the Surveillance, Epidemiology, and End Results (SEER) database showed the median age at diagnosis to be 69 years. The median survival of patients with angiosarcoma is just over 82 months. For those with stage IV disease, survival is only 29.2% at 1 year. 2
Very little is written about the best diagnostic pathway for angiosarcomas. In this case, the clinical picture of splenomegaly led to the diagnostic splenectomy. It is unclear if the bone biopsy alone would have been sufficient for diagnosis as that was not yet finalized prior to surgery for the splenomegaly.
In a recent review of primary splenic angiosarcomas published, only 205 were identified from 1968 through 2005. 3 Splenomegaly and abnormal blood counts were the most common presenting signs and symptoms for these primary angiosarcomas of the spleen. More than 85% of the patients in this review had metastases at the time of diagnosis. The rarity of this disease and the associated poor prognosis show the need to keep angiosarcoma in the differential diagnosis of patients presenting with splenomegaly and cytopenias, along with other evidence of metastatic malignancy, such as the pathologic fracture in this patient. In the evaluation of patients, for whom there is a suspicion of malignancy, a tissue diagnosis can be elusive. Having a multidisciplinary team involved is helpful and may be necessary for achieving a diagnosis. When splenomegaly is present, a splenectomy offers the opportunity to be both diagnostic and therapeutic.
Conclusion
A multidisciplinary approach is an ideal way to approach a diagnostic dilemma in which malignancy is suspected but yet unconfirmed. In this case, consultation with multiple specialists initiated by a general internist led to a diagnosis of angiosarcoma in a patient with widespread disease and splenomegaly.
Footnotes
Acknowledgements
The study team would like to thank the entire Mayo Clinic Undiagnosed Mass Clinic study team toward making this Clinic the success that it is today.
Author Contributions
All the authors participated in the data collection, interpreting the results, aiding in writing, and editing the manuscript. In addition, they have all seen and approved the final version of the manuscript. Each author will take public responsibility for the entire work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the Helen and Paul Baszucki Fund.
Ethical Approval and Consent to Participate
Minnesota state law gives patients the right to deny access to their Minnesota medical records for research purposes. This patient provided Minnesota authorization to allow use of her Minnesota medical record information. In addition, this patient was part of a larger study (under the Undiagnosed Mass Clinic Umbrella) in which she did give IRB consent which included a review of her electronic medical record.
Ethical Approval
All authors assert that all procedures contributing to this work comply with the ethical standards of the Mayo Clinic.