
Abstract
Objectives:
We aimed to evaluate the feasibility and effectiveness of a brief community-based intervention to promote physical activity (PA) and the mental well-being of adults in Hong Kong.
Methods:
A pilot cluster randomized controlled trial was conducted in 15 family service centers. The intervention group (N = 162, 8 centers) received two 2-h interventions uniquely combining “Sharing, Mind and Enjoyment (SME),” Zero-time Exercises (ZTEx), positive psychology, and simple family games. “Sharing” involved promoting PA among families and peers, “Mind” captured positive emotions during PA, and “Enjoyment” assessed engagement of PA. ZTEx are simple PAs to reduce sedentary behaviors and enhancing PA and fitness and require minimal time and no cost or equipment. The control group (N = 152, 7 centers) received interventions unrelated to SME. Primary outcomes were PA-related SME at a 3-month follow-up after completing the baseline questionnaire. Secondary outcomes included subjective happiness, well-being, and family-related outcomes. Participants reported self-perceived changes at 1- and 3-month. Nine focus group discussions with the participants and 4 individual in-depth interviews with community service providers were conducted.
Results:
The retention rate at1 month was 90.1% for the intervention group and 95.4% for the control group, while at 3 months, it was 83.3% and 92.8%, respectively. The intervention group showed significantly greater positive changes in PA-related outcomes than the control group at 3-month follow-up (Cohen’s d = 0.33-0.42, all P < .05). Most secondary outcomes were non-significantly different between the 2 groups. However, more than 90% of participants in the intervention group reported self-perceived positive changes at 1- and 3-month follow-ups. The qualitative data showed that ZTEx was popular with families due to its simplicity.
Conclusions:
Our trial showed the feasibility of implementing the brief interventions and the potential benefits for promoting physical activity in community adults.
ClinicalTrials.gov identifier:
NCT03332810 (date of registration: November 6, 2017).
Introduction
The prevalence of major depressive episodes (MDE) among young people in Hong Kong was high during the time periods before, during, and after the COVID-19 pandemic from 2019 to 2022. 1 The prevalence of MDE increased from 13.2% during May 2019 and June 2020 to 18.1% during July 2020 to December 2020. 1 However, the prevalence returned to pre-pandemic level by 2022 (13.2% during July 2021-June 2022). 1 Another survey conducted during the COVID-19 pandemic in Hong Kong showed that 41.8% of adults had mild to moderate depressive symptoms, and 14% had anxiety disorders. 2 Globally, age-standardized disability-adjusted life-years (DALY) rates increased most substantially for anxiety disorders (16.7%, 14.0-19.8), depressive disorders (16.4%, 11.9-21.3) among the 25 leading Level 3 causes between 2010 and 2021. 3 Practical or simple universal or population-based approaches to prevent mental disorders at population levels had been advocated before and since the COVID-19 pandemic.4 -7 Population-based approaches have a greater emphasis on prevention and early intervention and look for modifiable lifestyle factors for preventive measures. 4 However, most interventions remain using complex components for individuals. 8
Around 7% Hong Kong Chinese aged 16 to 75 years were reported to have mixed anxiety and depressive disorder (MADD) in 2010 to 2013. 9 The demand for psychiatric services in Hong Kong has been rising, with the number of patients with mental illness under the care of the Hospital Authority increasing from about 187 000 in 2011 to 2012 to over 220 000 in 2015 to 2016. 10 A territory-wide and population-based mental health promotion campaign named “Joyful@HK” was launched by the Hong Kong Department of Health in January 2016, under 3 main themes: Sharing, Mind, and Enjoyment (SME). 11 Sharing connects families and friends and supports those in need. Mind entails keeping an open mind and being optimistic. Enjoyment is about engaging in enjoyable activities to maximize one’s potential and achieve satisfaction. 11 These themes align with the principles of positive psychology and Seligman’s PERMA model (Positive emotions, Engagement, Positive relationships, Meaning, and Accomplishment).12,13 Positive psychology-based interventions have shown effectiveness in enhancing well-being and reducing symptoms of mental disorders.14 -18 Given the importance of family in Chinese culture 19 and the family’s role in mental illness prevention, 20 this trial adopted a positive psychology-based intervention model to promote SME and mental well-being of adults through involving families and collaborating with community service partners to ensure a culturally sensitive intervention.
Regular physical activity (PA), especially jogging and walking, is associated with lower depressive symptoms and greater emotional well-being.21 -23 However, only 57% of Hong Kong adults aged 18 to 64 years had engaged in at least 10 min of moderate PA in a week, and even fewer (45%) had been involved in vigorous PA. 24 Lack of time, resources, skills, weather, or inconvenience are common barriers. 25 Furthermore, community service providers such as social workers often find intensive PA difficult to handle and deliver to people of different ages or with physical disabilities. Therefore, we proposed a Zero-time Exercise (ZTEx), which requires zero extra time, zero cost, and zero equipment.26,27 Physical exercise usually take extra time, but will take zero extra time if people integrate PA into their daily activities, such as waiting for transportation or during the time of watching TV. Our previous pilot randomized controlled trials (RCTs) showed that ZTEx reduced sedentary behaviors and enhanced PA and fitness, with small to large effects (effect size = 0.27-1.05).28,29 ZTEx is easy for community service providers to learn and can potentially be adopted as a part of mental health promotion interventions. In addition, ZTEx can facilitate interventionists in engaging the participants promptly. Prompt practice is critical to the success of behavior change. 30 ZTEx employs a gradual initiation strategy (foot-in-the-door approach), beginning with manageable exercises and progressively fostering confidence in physical activity. 29
The present pilot cluster RCT evaluated the feasibility and effectiveness of brief SME-based ZTEx interventions in promoting PA and mental well-being in adults. Brief interventions were designed to engage participants through prompt practice and encourage participants to act immediately after the interventions.
Methods
Participants
The trial (registry number: NCT03332810) was conducted in 2017 to 2018 in partnership with the Hong Kong Council of Social Service (HKCSS). The HKCSS approached 15 local community service centers with 3 District Healthy City Committees. People aged 18 to 59 years who can read and communicate in Chinese and willing to participate were enroled. Ethical approval was obtained from the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (reference: UW 17-334). All participants provided written informed consent.
Recruitment
Participants were recruited through collaboration with non-governmental organizations (NGOs). We sought the assistance of these NGOs to reach out to their existing clients or individuals who were interested in participation. The NGOs approached their clients and invited them to take part in the study. Only those who were interested in participation were invited for screening.
Procedures
To avoid contamination caused by interactions among participants within the same community, and to better simulate the real-world implementation of the intervention, a cluster randomized controlled trials (cRCT) design was used. Each of the 15 centers served as a distinct cluster, located in the Central & Western District (6 centers), Tsuen Wan District (6 centers), and Sham Shui Po District (3 centers). Stratified randomization by district was conducted. Eight centers were randomized to the intervention group, and the other 7 were randomized to the control group. One person not involved in the randomization process allocated the group using serially labeled, sealed, and opaque envelopes concealed from the cluster representatives. However, blinding was impossible as the intervention was evident to researchers and participants. The data analyst was not blinded to group allocation because of logistic constraints and the nature of the intervention. To mitigate potential bias, all data were collected by the same research team using standardized procedures and consistent explanations across both intervention and control groups.
SME Intervention Group
One or 2 social workers from each center attended a 1-day train-the-trainer workshop. The workshop, comprising interactive talks, group-based games, and small group discussions, was led by 3 experienced instructors (social worker, clinical psychologist, and nurse). The training focused on the concepts of SME and ZTEx-based PA, principles of positive psychology, symptoms of mixed anxiety and depressive disorder, and the design of mental well-being activities in community settings. After the training, social workers from each center designed and conducted 2 sessions of mental well-being interventions for their service users according to the needs of their districts. Each session lasted for 2 h.
The first session briefly covered the symptoms of mixed anxiety and depressive disorder, help-seeking for emotional disturbances, the concept of SME, and the benefits of doing ZTEx. The social workers used simple family games (eg, dancing and competitions) to engage the participants in understanding SME, provided feedback after each game, and encouraged them to do PA daily. Examples of ZTEx 31 included shrugging shoulders, tilting the head up and down, lifting the legs off the ground, and cycling in the air, most of which can be done while standing, sitting, walking, lying down, watching TV, or waiting for transportation. In small groups, the participants had prompt practice to create and share their own movements with others. The session ended with a reminder to do more PA, preferably with family members, and to encourage family members to do ZTEx together.
The second session was held after about 1 month to reinforce the effect indoors or outdoors. For indoors, more family games were used to enhance the understanding of SME and to encourage more PA after class. Outdoor activities included mindful running, walking tours, family soccer balls, and competitive games.
Control Group (Attention Control)
Given practical implementation and ethical considerations, the community service centers also held activities for control group participants after completing all intervention sessions. The activities included lunch/tea gatherings (2 centers), table games (1 center), diet tips (1 center), environment protection tips (1 center), movie watching (1 center), and a farm tour (1 center). The activities were not related to SME or PA. The duration was similar to that of the intervention group.
Outcome Measurements
Baseline and outcome data were collected by the research team using paper-based questionnaires. Participants completed the questionnaires at scheduled intervals, and the data collection was supervised by the research team to ensure consistency and accuracy. The questionnaires were self-administered by the participants, with the research team available to provide clarification if needed.
We measured all outcomes at baseline (before the first session of intervention), 1 (before the second session), and 3 months after baseline. The primary outcomes were 10 self-developed PA-related SME items. 11 Each item measured the days in the past 7 days when the activity occurred (range 0-7). These items were divided into Sharing (3 items: “encourage family members to do PA,” “encourage family members to do ZTEx,” “do PA with family members,” range 0-21; congeneric reliability .84); Mind (3 items: “have the motivation to do PA,” “do PA with a goal,” “do PA with confidence,” range 0-21; congeneric reliability .92); and Enjoyment (4 items: “do at least 30 min of vigorous PA,” “do at least 30 min of moderate PA,” “do ZTEx,” “enjoy PA,” range 0-28; congeneric reliability .67). Higher scores indicated more SMEs. We reported similar measurements in our previous papers.32,33 As the control group did not learn ZTEx, we put a note together with the question to explain what is ZTEx (ZTEx refers to simple exercises that can be integrated into daily routines, such as moving different parts of the body while sitting, standing, or walking) to avoid the bias in outcome assessment.
Details of the scales measuring the secondary outcomes had also been reported previously. 33 Secondary outcomes included Subjective happiness measured by the 4-item Subjective Happiness Scale (SHS; ranged from 1 to 7, test-retest reliability ranged from .55 to .90), 34 Wellbeing measured by the 7-item Short Warwick-Edinburgh Mental Well-being Scale (SWEMWBS; ranged from 7 to 35, the congeneric reliability and the test-retest reliability of the scale was .85 and .70, respectively).35,36 Personal health and happiness measured by 2 single-item questions (how healthy/happy do you think you are, range 0 [not at all healthy/happy] to 10 [very healthy/happy]), Family health, happiness and harmony measured by single-item questions (how harmonious/happy/healthy do you think your family is,” range 0 [not at all harmonious/happy/healthy] to 10 [very harmonious/happy/healthy]), 37 and Family relationships measured by 3 questions about family understanding, intimacy, and communication with family members (sum of the 3, total range 0-30).33,38
Subjective Changes and Process Evaluation
Subjective changes were measured at 1- and 3-month follow-up among participants in the intervention group. These changes included aspects such as enjoyment of physical activity, perceived health improvements, and overall happiness, with questions rated on a 5-point Likert scale from 1 “much less” to 5 “much more.” The specific subjective changes assessed are detailed in Supplemental Table 1. Process evaluation on the satisfaction of the activity, whether participants can learn SME from the activity, and whether participants can acquire mental health knowledge, was conducted at 1- and 3-month. Specific questions included, for example, “How satisfied are you with the first activity?” and “How confident are you that you can learn SME from the activity?” The questions were rated on a 0 to 10 scale from 0 “very unsatisfied” to 10 “very satisfied.” Participants were asked whether they would like to share the activity with others (yes/no).
Focus Group Discussions and In-Depth Interviews
Nine focus group discussions with 88 intervention group participants and 4 individual semi-structured in-depth interviews with 3 community service partners were conducted to explore participants’ satisfaction with the interventions, subjective changes, and suggestions. The interview guides were shown in Supplemental Materials. The focus groups and in-depth interviews were led by either the research assistant with a psychological education background or the project officer who have a public health education background. Each interview included a moderator who primarily asked questions and a note taker to record the necessary background information. The interviews were audiotaped and field notes were taken during the sessions. The name list and demographic data were provided by the community collaborators before the interview. Written consent were collected before the interviews.
Fidelity
One to 3 persons per center (government research officers, university research staff, and social workers) independently completed a fidelity assessment for each intervention session to evaluate the extent to that the activities and delivered SME messages adhered to the proposed rundown.
Statistical Analysis
Quantitative data were analysed using STATA 13.0. We calculated between-group mean differences (BMD, intervention vs. control) in the outcome changes using multilevel mixed-effects linear regression models (command xtmixed), adjusting for clustering effect, and significantly different demographics and outcome variables at baseline. An intention-to-treat (ITT) analysis was adopted by including all randomized subjects. The missing observations from loss to follow-up or not completing follow-up questionnaires were imputed using chained equations. 39 An effect size (ES, Cohen’s d) of 0.2 was considered small, 0.5 medium, and 0.8 large. All significance tests were 2-sided, with P < .05 indicating statistical significance. Within-group differences were conducted using paired t-tests. Qualitative data were analysed using thematic content analysis. 40 One researcher transcribed the interviews verbatim, read the transcripts thoroughly, and collated the data into potential themes. The themes were checked and refined until clear definitions and names were created for each theme. Another researcher double-checked the codes and themes. Some representative examples were extracted. 40
Results
Figure 1 shows the CONSORT flowchart. Fifteen community service centers (314 eligible participants) were recruited during November 2017 to January 2018, with 162 participants in the intervention group and 152 participants in the control group. The retention rate at 1 month was 90.1% for the intervention group and 95.4% for the control group, while at 3 months, it was 83.3% and 92.8%, respectively. Table 1 shows that most participants (88.9% in the intervention group and 82.9% in the control group, P = .13) were female. The average age was 41.2 (SD = 7.96; intervention group 41.4 (8.51) vs control group 41.0 (7.35), P = .60). None of the baseline characteristics were significantly different between groups.

CONSORT flowchart.
Baseline Characteristics of the Intervention and Control Group (n = 314).

1 US$ = 7.8 HK$.
Primary and Secondary Outcomes
Table 2 shows significantly greater positive changes in the intervention versus control group in Sharing (1-month BMD = 1.78, 95% CI = 0.11-3.45, Cohen’s d = 0.32; 3-month BMD = 2.22, 95% CI = 1.03-3.40, d = 0.42), Mind (1-month BMD = 1.86, 95% CI = 0.39-3.34, d = 0.34; 3-month BMD = 1.88, 0.64-3.13, d = 0.33), and Enjoyment (1-month BMD = 2.82, 95% CI = 1.38-4.27, d = 0.45; 3-month BMD = 2.49, 95% CI = 1.16-3.82, d = 0.41).
Outcome Comparison Between SME Intervention Group and Control Group at 1- and 3-Month.
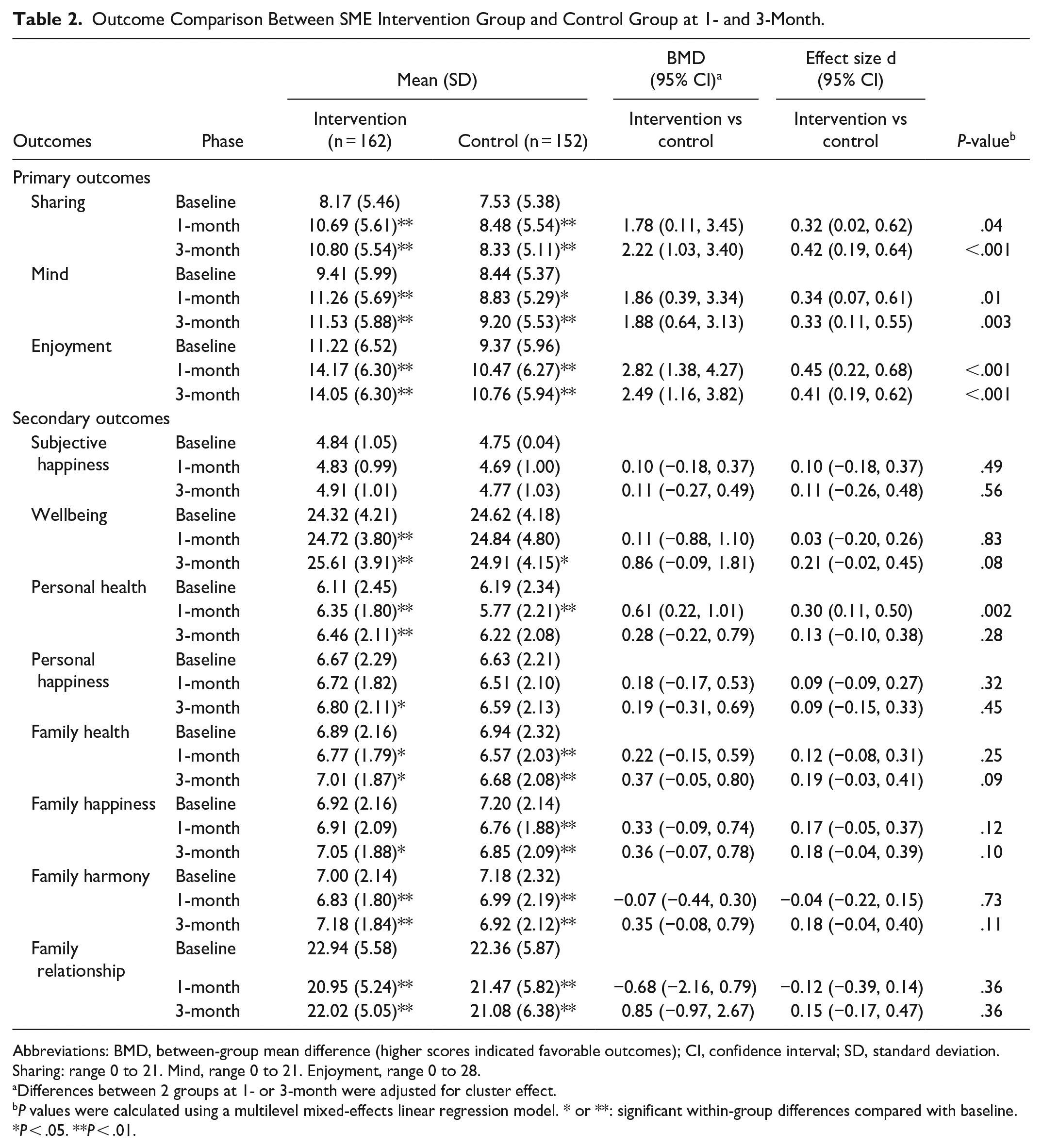
Abbreviations: BMD, between-group mean difference (higher scores indicated favorable outcomes); CI, confidence interval; SD, standard deviation.
Sharing: range 0 to 21. Mind, range 0 to 21. Enjoyment, range 0 to 28.
Differences between 2 groups at 1- or 3-month were adjusted for cluster effect.
P values were calculated using a multilevel mixed-effects linear regression model. * or **: significant within-group differences compared with baseline. *P < .05. **P < .01.
At-1-month, compared to the control group, 7 of 8 secondary outcomes in the intervention group did not show significantly different changes except for the significantly greater positive change in personal health (BMD = 0.61, CI = 0.22-1.01, Cohen’s d = 0.30). At 3 months, all 8 outcomes in the intervention group showed non-significantly different changes from the control group. No harmful effects was reported.
Table 2 shows significant within-group improvements at 3 months in sharing, mind, enjoyment, and well-being (all P < .01) in both groups. At 3 months, both groups showed no change in subjective happiness (mean difference = 0.06 in the intervention group and 0.02 in the control group). Only the intervention group showed improvements in personal health and happiness, family health, happiness, and harmony (mean difference = 0.35, 0.14, 0.13, 0.14, and 0.19, all P < .05). The intervention group showed significant deterioration in family relationships (mean difference = −0.74, P < .01), while the control group showed significant deterioration in family health, happiness, harmony, and family relationships (mean difference = −0.26, −0.36, −0.26, −1.44, all P < .01).
Subjective Changes and Process Evaluation
Supplemental Table 1 shows that regarding the subjective changes, most participants reported a little more or much more positive changes in enjoying PA (86.2%), encouraging family members to do PA or ZTEx (89.2%), and doing PA with families (89.2%) at 1 month. In comparison, the proportion at 3 months was 86.6%, 90.2%, and 82.8%, respectively.
Table 3 shows that the process evaluation scores at different time points were all above 8 out of 10 (ranging from 8.07 to 8.49) except for 1 item, “know more about mixed anxiety and depressive disorder” (7.59). Ninety-seven percent of the participants were willing to share the intervention with others.
Process Satisfaction at 1- and 3-Months Among Intervention Group Participants.

Abbreviations: MADD, mixed anxiety and depressive disorder; SD, standard deviation; SME, sharing, mind, enjoyment; ZTEx, zero-time Exercise.
Scores range from 0 to 10; higher scores indicate higher satisfaction.
Fidelity
The adherence to the proposed rundown and delivery of SME messages was 92.4% (SD = 10.57) and 90.6% (SD = 11.39; n = 25 observations) for the first session, and 92.0% (SD = 8.37), and 91.4% (SD = 8.70) for the second (n = 16 observations).
Focus Group Discussions and In-Depth Interviews
Engagement in the Activity and Improvement in Family Relationship
Some participants said they engaged in the activities and had a great time with their families doing PA, such as ZTEx and dancing. Some said these helped improve family relationships and bring positivity to their family members.
Here we could spend some time together with families. I could also arrange (such activities) by myself, but it was good to be together with other families. (Male, 44 years)
The activity was perfect for releasing stress. (Female, 38 years)
I learned ZTEx from this activity. ZTEx takes no extra time, e.g., you can do exercise when you are watching TV. (Female, 40 years)
Our favourite activity is dancing. After the activity, my son searched for that video online. Now we dance together at home when we are free. (Female, 43 years)
Improvements in Doing PA
Some participants reported doing more exercise, including ZTEx, indoors, and outdoors. They also reported better health and mental conditions after doing more exercise. In addition, some participants encouraged their family members to exercise with them.
I feel healthier and happier now. I used to have sleep problems. Now I do exercise every day, which might have improved my sleep quality. (Female, 37 years)
I did exercise at home with my daughter. She taught me how to dance. (Female, 41 years)
My mom is very old, and she watches too much TV. It is perfect to teach her some ZTEx at home. (Female, 55 years)
Suggestions for Future Interventions
Some participants said the intervention was too short and should have had more sessions. In addition, some suggested that follow-ups and reminders should continue after the program. Instead of a 1-off program, sustainable services, such as updating information online about ZTEx and SMEs, are needed to maintain the effect.
I wish to learn more about ZTEx. More examples can be provided and put on YouTube. (Female, 32 years)
[The organisers] should provide more activities. We will forget the activities over time. It would be nice to have more sessions. If it is not sustainable, the previous work could be a waste. (Female, 55 years)
Community Service Providers’ Views
The community collaborators also liked the program themes and PA-based approach. They found the program meaningful and well-suited for the community. Some suggested booster sessions or longer duration for each session. The program should be promoted to more community centers.
The SME concept is straightforward and clear; physical activity promotion is useful to facilitate interaction and communication. (Female)
The intervention is suitable for the community participants, and the messages are easy to deliver. (Female)
The interaction among participants during the activities can be enhanced. The length of the sessions could be longer. (Male)
Discussion
This is the first RCT to assess the effectiveness of a brief physical activity promotion intervention on improving PA-related SME among Hong Kong Chinese families, and highlighted several distinct features of our approach. First, the intervention uniquely combined SME with ZTEx, and simple movements that can be easily integrated into daily routines. Second, the intervention was very brief, consisting of just 2 sessions totaling 4 h, showing the potential of scalability and adaptability in population-based campaigns. Third, the interventions were delivered by social service and healthcare workers from various NGOs, who only received brief training for the present project, and they brought realistic perspectives in promoting physical activity within families. The interventions were implemented with high fidelity, suggesting the validity of the findings. The retention rates at follow-ups were above 83%. The small effect size at 1- and 3-month follow-ups was expected: PA-related SME (Cohen’s d = 0.32-0.45) and personal health (d = 0.30). More than 90% of participants reported self-perceived positive changes at 1- and 3-month. The process evaluation and qualitative data triangulated the positive effects of the interventions.
The quantitative findings of the primary outcomes of SME are consistent with those from a meta-analysis of interventions for improving PA in healthy adults, while their interventions were typically long. 41 The significant positive changes of our brief interventions might be due to the simplicity of the intervention and the prompt practice as suggested. A meta-analysis summarized the effective behavior change techniques in changing individuals’ PA. 30 It showed that the interventions, including prompt cues, practice, and rewards, had the largest effects on PA. 30 ZTEx movements can be learned and mastered quickly and are more sustainable, even for busy people and families. More than half the citizens in Hong Kong had less than 10 min of vigorous PA weekly, 24 and the lack of time or skills was a significant barrier to PA. 25 It is plausible that simple movements such as ZTEx, jogging, walking, and group-based dancing can boost participants’ confidence in doing PA compared to more demanding therapy and training. 23 We found that participants had more motivation, confidence, and engagement in doing PA at 1 and 3 months from the primary outcomes. Although the BMD differences appeared modest in absolute differences, it is important to note that an effect size greater than 0.2 is generally considered to have practical significance. 42 Therefore, even with relatively small BMD differences, the observed effect sizes suggest that the intervention had a meaningful impact on the participants. The qualitative data showed that ZTEx was popular with families due to its simplicity and fun. Some participants found the activities enjoyable and engaging and desired more examples of ZTEx and dance music after the intervention sessions. Therefore, our brief interventions should be scalable for promoting physical activities in population-level health campaigns.
We did not significantly improve the secondary outcomes, including subjective happiness, well-being, and family-related outcomes, for several reasons. First, brief and low-intensity interventions often result in small effect sizes, as research has suggested that PAs with high intensity contribute more to mental well-being.23,43 However, the long-term effect is yet to be confirmed. Second, our sample size might have been inadequate to detect small changes. For example, the effect size for improving well-being at 3 months was 0.21; the power was 0.46. Finally, improving outcome measurements is more challenging for healthy populations because they tend to achieve more favorable baseline scores. For instance, a study reported that the mean SWEMWBS score in healthy individuals was higher than in those with depression (25.0 vs 21.3). 44 This means that further improvements by simple interventions would be limited because the participants already performed quite well initially. Therefore, the interventions may have greater benefits for the patients with less favorable outcomes related to mental and physical health. In future studies, it may be useful to screen community members to identify those with poorer mental and physical health to validate this hypothesis. If effective, the interventions for these populations could be recommended to maximize public health benefits.
This trial had several limitations. First, as validated questionnaires were unavailable for all outcomes and many existing questionnaires were too long, we developed our simple outcome and impact-oriented questionnaires to ensure the participants were not too burdened. A systematic review of 187 studies found only low to moderate correlation between self-report and direct measures of physical activity, but no clear pattern was found regarding the direction of the differences. 45 Although our measurements showed good congeneric reliability in general, future studies should test the validity of these measurements. However, our results on positive subject changes in almost all participants could account for the validity of the quantitative pre- and post-intervention positive changes. Second, blinding the participants was not feasible in our trial because each cluster required a fixed timetable and activity before they started doing recruitment. We did not blind the individual analyzing the data, which potentially introduced bias and exaggerated effects. 46 Besides the effect size, subjective change was an important indicator for the improvements after the interventions. However, as these subjective changes were not assessed in the control group, it is unclear whether similar changes might have occurred in control group participants if they had been measured. Therefore, further research is needed to determine the reliability of subjective changes. Third, although brief interventions have shown potential for scalability and adaptability in population-based activities, participants, and service partners suggested that longer durations and more sessions might be required to fully meet their needs. Participants also suggested follow-up and reminders to increase the effectiveness of the intervention. Thus, the program might not fully meet the preferences or expectations of participants and service partners, which may limit its overall impact. Lastly, it is inconclusive whether group activities in the control group increase happiness and well-being; this ambiguity could lead to an underestimation of effect size. The topics were not related to SME but included some lifestyle interventions such as diet and some fun activities. As shown in the within-group difference, the well-being in the control group also improved at 3 months compared to the baseline.
Our pilot trial has also shown the feasibility of academic and community service-provided collaboration on developing, delivering, and evaluating the SME program. Such collaboration was designed for future implementation in the community, promoting SME and physical activities among many families and reflecting a community-based approach. Further research with a large sample size and longer follow-up on this simple intervention to promote the population’s well-being is warranted. Incorporating wearable devices in future studies could provide more objective measures of physical activity.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241281567 – Supplemental material for Brief Intervention to Promote Physical Activity and Mental Well-Being in Community Adults: A Pilot Cluster Randomized Controlled Trial
Supplemental material, sj-docx-1-jpc-10.1177_21501319241281567 for Brief Intervention to Promote Physical Activity and Mental Well-Being in Community Adults: A Pilot Cluster Randomized Controlled Trial by Yuying Sun, Sai Yin Ho, Christian S. Chan, Man Ping Wang, Alice N. T. Wan, Yudian Xu, Agnes Y. K. Lai and Tai Hing Lam in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We sincerely thank the Hong Kong Council of Social Service for coordinating participant recruitment and activity delivery. We also thank all participants for their active involvement, social workers for conducting the interventions, and all research assistants for helping with the project implementation.
Author Contributions
Yuying Sun: Methodology, Formal analysis, Investigation, Data Curation, Writing—Original Draft, Writing—Review & Editing. Sai Yin Ho: Conceptualization, Methodology, Resources, Data Curation, Writing—Review & Editing, Funding acquisition. Christian S. Chan: Methodology, Validation, Writing—Review & Editing. Man Ping Wang: Conceptualization, Methodology, Writing—Review & Editing, Supervision, Project administration, Funding acquisition. Alice N.T. Wan: Conceptualization, Methodology, Investigation, Project administration, Writing - Review & Editing. Yudian Xu: Writing—Review & Editing, Visualization. Agnes Y.K. Lai: Validation, Resources, Writing—Review & Editing. Tai Hing Lam: Conceptualization, Methodology, Resources, Writing—Review & Editing, Supervision, Funding acquisition.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by Health and Medical Research Fund Health Care and Promotion Scheme (Project No. CPP-HKU), Health Bureau, The Government of the Hong Kong Special Administrative Region. All authors declare no financial relationships related to the manuscript.
Ethical Approval
Ethical approval was obtained from the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (reference: UW 17-334). All participants provided written informed consent.
Trial Registration
ClinicalTrials.gov identifier: NCT03332810 (date of registration: November 6, 2017).
Data Availability
Data will be made available upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.