
Abstract
Background:
The prevalence of cardiovascular diseases (CVD) is continuously increasing. A nurse-led workplace health promotion program (NWHPP) has demonstrated potential in reducing cardiovascular risks among employees. This study aimed to evaluate the effectiveness of the NWHPP in reducing CVD risks among at-risk workers.
Methods:
Sixty workers from 2 factories in Thailand, each with an estimated 10-year cardiovascular risk of 5% or higher (determined by the WHO/ISH cardiovascular risk prediction chart), were enrolled. Participants were randomly assigned to either the intervention or control group based on their factory. The intervention group received an 8-week program comprising 3 core components: redesigning healthcare services, strengthening self-management, and obtaining organizational support. Evaluations of the estimated 10-year CVD risk, systolic blood pressure (SBP), smoking status, and body mass index (BMI) were conducted at baseline and at 1- and 3-month follow-ups.
Results:
The intervention group showed significant improvements compared to the control group in CVD risk score (F = 4.827, P = .017) and SBP (F = 12.136, P < .001). Moreover, non-smokers were significantly higher in the intervention group (75.0%) compared with the control group (46.2%) after the 3-month follow-up (OR = 3.50; 95%CI 1.11-11.07; P = .030). However, BMI differences between the groups were not statistically significant.
Conclusion:
The nurse-led workplace health promotion program effectively improved cardiovascular risk scores among at-risk workers. Developing workplace policies and environments that promote healthy behaviors is essential for reducing CVD risks among at-risk workers.
Keywords
Background
Cardiovascular diseases (CVDs) are the leading cause of death globally, 1 with three-quarters of these deaths occurring in low- and middle-income countries (LMICs). In LMICs, late detection and inadequate healthcare often lead to premature CVD deaths, particularly among the 20 to 64 and 30 to 74 age groups. 2 Thailand, a middle-income country, has seen rising CVD mortality rates: stroke deaths increased from 47.81 per 100 000 in 2017 to 55.53 in 2021, and ischemic heart disease deaths rose from 31.82 to 33.54. 3 In 2022, the mortality rate for CVDs in the 15 to 59 age group was 53.6 per 100 000. 3 Behavioral risk factors like unhealthy eating, lack of physical activity, tobacco use, and excessive alcohol consumption are prevalent among Thailand’s working-age population. 4 Addressing these risks through targeted interventions can reduce premature CVD mortality and improve health outcomes.
The working-age group is at high risk for cardiovascular diseases. The workplace, where workers spend a significant portion of their time, is an ideal setting for health promotion strategies to reduce CVD prevalence. Current healthcare delivery for workers addresses both work-related and non-work-related illnesses. The Total Worker Health approach, which integrates safety with health promotion, has proven effective in reducing chronic diseases and improving overall health.5 -7 Workplace interventions such as training, education, and counseling can significantly lower cardiovascular risks.8 -10 Employers can target high-risk groups, and nurses can engage workers in health initiatives, promoting healthier lifestyles. In workplaces, nurse-led health promotion programs have been effective in lowering cardiovascular risk. 11 However, in Thailand, nurses are mostly confined to clinical roles focused on primary care. 12 Expanding their role to lead health promotion and disease prevention programs could enhance workplace health outcomes.
The Expanded Chronic Care Model (ECCM) 13 is designed to improve healthcare organizations’ approach to disease prevention and management by enhancing strategies for health promotion and disease prevention. The ECCM includes decision support mechanisms, connects healthcare systems with community resources, offers self-management support, and manages information systems. This model can be effectively integrated into workplace health promotion programs, as it promotes population health, considers social determinants of health, and provides a comprehensive approach to disease prevention and management.
In Thailand, despite several workplace programs aimed at preventing cardiovascular diseases, the prevalence and mortality rates among the working-age population remain high and continue to rise. 3 Current workplace health promotion programs often target the general working population rather than focusing on high-risk groups. Developing workplace intervention that specifically address workers with cardiovascular risks is crucial. Intervening early with at-risk workers can prevent the onset or progression of CVD. Tailored interventions that focus on those most at risk are also more likely to produce significant health improvements compared to general population approaches. By addressing specific risk factors, these programs can lead to better health outcomes and healthier lifestyle choices. Workplace programs using the EECM can more effectively prevent CVD by promoting population health, addressing social determinants, and encouraging community involvement. Nurses play a key role in providing feedback and education on self-management within the ECCM framework. This research aims to develop and evaluate a nurse-led workplace health promotion program (NWHPP) using the ECCM to enhance workplace health services for those at risk of CVDs, while also promoting the role of nurses in health promotion and disease prevention at work.
Methods
This research follows a randomized controlled trial. The protocol was registered in the Thai Clinical Trials Registry (TCTR20210923009). In a cluster randomized controlled trial, with the factory as the unit of randomization, 60 participants from 2 factories were enrolled in each condition to compare the intervention with control condition. The intervention group received NWHPP lasted for 8 weeks. The control group was given brief advice and leaflets based on their cardiovascular risk factors. Figure 1 shows the flow diagram of the study.

The flow diagram of the study.
A study was carried out in 2 ceramic roof tile factories owned by a company locating in the central region of Thailand, each with over 200 employees in which a nurse was required by law to be available on-site. The production processes in both factories are comparable. It should be noted that no NWHPP was provided to workers during the study period.
The research participants comprise workers who are considered at-risk and currently employed in eligible factories. The sample size was calculated with G* Power 3.1.9.4 14 ; The effect size of each dependent variable in this study was calculated based on the finding of experimental research conducted with workers with cardiovascular risk. F tests-ANOVA: Repeated measures, within-between interaction. To account for potential dropouts or missing data, an additional 25% was added, a total of 60 individuals were ultimately recruited. To participate in this study, participants must be at risk for CVDs (5% or higher). Risk status was determined by the WHO/ISH cardiovascular risk prediction chart (non-laboratory-based) 15 by analyzing the results of our participants’ annual health checkups, age 20 or older, and willing to participate. Those who were pregnant and being diagnosed or treated for CVDs, chronic kidney disease, and cancer were excluded.
The NWHPP is an 8-week program designed for at-risk workers, with guidance from the Expanded Chronic Care Model. Therefore, the core components of NWHPP are in line with components of the Expanded Chronic Care Model and consist of 1) redesigning workplace healthcare service, 2) strengthening self-management, and 3) obtaining organizational support. Table 1 summarizes the core components, sub-components, and nurse activities of the NWHPP.
The Nurse-Led Workplace Health Promotion Program (NWHPP).
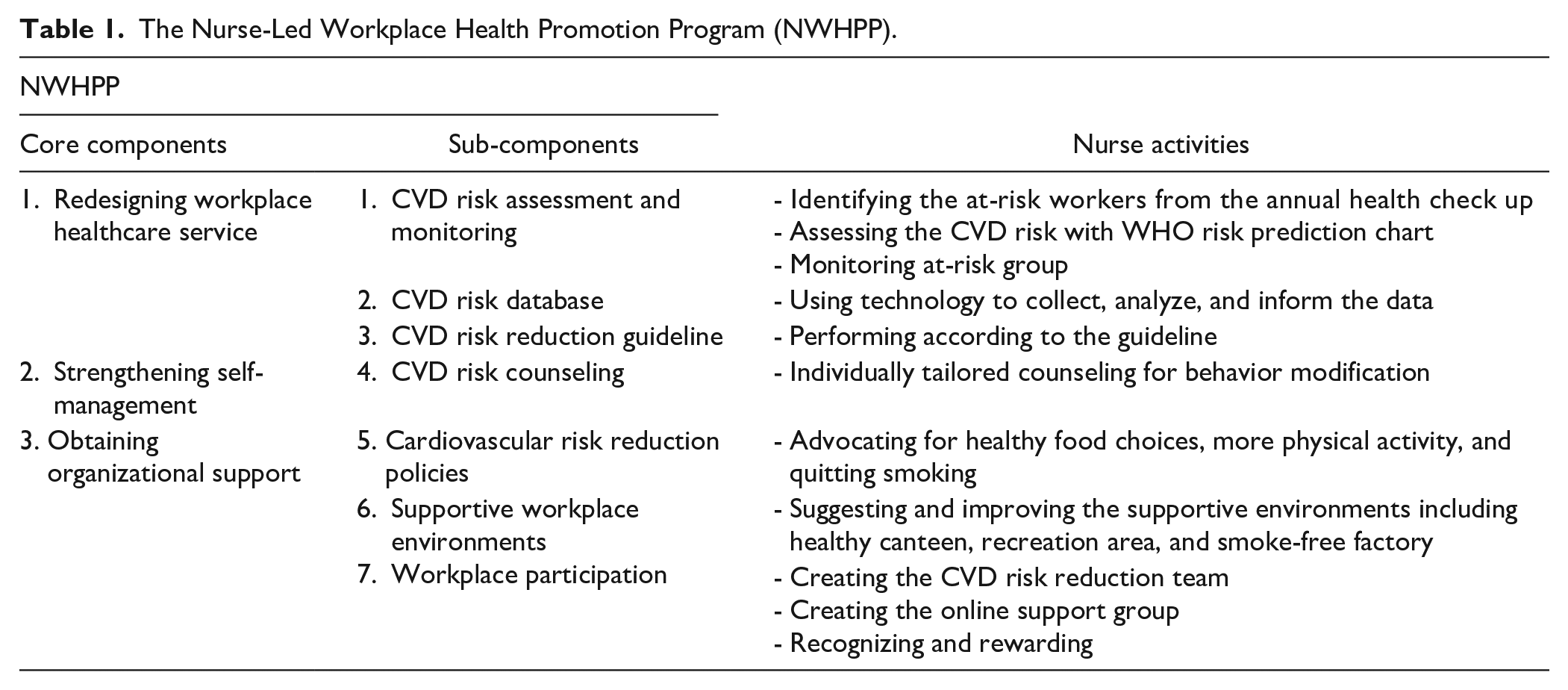
The intervention was implemented from January to February 2022. A nurse initiated an 8-week NWHPP in the first week by identifying workers at risk from the result of an annual health checkup. Their cardiovascular disease risk was assessed using the WHO/ISH cardiovascular risk prediction chart (non-laboratory-based), and the data was then collected in a CVD risk database. Afterward, in the second week, a nurse advocated for health promotion policies and collaborated with the healthcare team to create a team that reduces the risk of CVD and an online support group for at-risk workers. Moreover, the nurse suggested enhancing supportive environments.
During weeks 2 to 8, the program focused on counseling, providing support, monitoring, and rewarding. In week 2, the nurse conducted individually tailored counseling sessions aimed at behavior modification to reduce cardiovascular disease (CVD) risks. Each session lasted 30 to 45 min and followed a four-step process: 1) Understanding the participant The nurse first got to know the participants and their current life circumstances, 2) Identifying focus areas The nurse then helped participants identify and prioritize areas where change was needed, recognizing current behaviors hindering their goals. Goals could originate from the participant, the situation, or the nurse, 3) Encouraging discussion The nurse asked questions to prompt participants to discuss their reasons for wanting to change, and 4) Planning and commitment Finally, the nurse assisted participants in planning their behavior changes and encouraged their commitment to these changes.
From weeks 3 to 7, the nurse monitored participants’ health behaviors and indicators while providing supportive information on reducing CVD risk. This information was shared through online channels (such as posters on the LINE application) and onsite channels (such as billboards). If participants struggled to make behavioral changes, the nurse provided additional support by listening, identifying areas needing more effort, and helping overcome any obstacles preventing behavioral changes.
These participants were then rewarded for their efforts at the end of program (week 8). The instruments of the program include a CVD assessment tool, learning media on CVD and lifestyle modification, a personal record book for setting goals and monitoring behaviors.
Outcomes
Smoking status was assessed by asking the Yes/No question to determine current smoking status. Smoking cessation was defined as answering “No” to the question, “Have you smoked any in the last seven days?” at the last contact.
SBP was measured twice using a HEM-7320 Omron digital blood pressure monitor (Omron, Hoofddorp, The Netherlands) while seated after 10 min of rest. The digital monitor was calibrated against a traditional mercury sphygmomanometer to ensure accuracy.
BMI, weight was measured using a digital scale (TANITA HD 394), while height was measured with a wall-mounted stadiometer.
CVD risk was measured by WHO CVD risk (non-laboratory-based) chart. The estimation of 10-year cardiovascular disease risk was used to investigate the risk of cardiovascular disease. WHO CVD risk (non-laboratory-based) chart was calculated based on the 5 coronary risk factors including age, gender, systolic blood pressure, smoking habits, and body mass index. Absolute cardiovascular disease risk percentage over 10 years was classified as low risk (< 5%), intermediate risk (5-20%), and high risk (> 20%).
Data Analysis
Data was collected from November 2021 to June 2022. Statistical analyses were performed to obtain descriptive statistics and to evaluate the intervention effectiveness. Intention-to-treat analysis was used to manage missing data, where missing values in the continuous variables were impacted by means. Descriptive statistics in terms of frequency and percentage were used to describe the participants’ characteristics and study variables. Chi-squared and Fisher exact tests were used to determine sample equivalence at baseline. Repeated measures ANOVA was used to test the interaction effect (groups × time) of each continuous outcome. An independent t-test was employed to examine the differences between the groups. The criterion for statistical significance was set at P < .05 (2 tailed) for all analyses. The data were analyzed using a statistical software program: IBM SPSS Statistics version 29 (IBM Corp. Released 2022. IBM SPSS Statistics for Windows, Version 29.0. Armonk, NY: IBM Corp).
The study was approved by the Ethical Review Committee for Human Research, Faculty of Public Health (PHIRB) of Mahidol University (COA. No. MUPH 2020-107). Before the data collecting process, participants were provided with written and verbal information and completed a consent form. Participation was voluntary, and participants could withdraw from the study at any time.
Results
Two out of 4 ceramic roof tile factories located in the central of Thailand were recruited. Of 821 eligible workers, 60 (7.3%) consented to participate in the study. Thirty participants (one factory) were randomly assigned to the intervention group and 30 participants (one factory) were randomly assigned to the control group via cluster randomization. All baseline data were successfully collected. At 3-month follow-up, 2 (6.7%) and 4 (13.3%) participants dropped out from the intervention and control groups, respectively. In total, data from 54 participants (28 in the intervention group; 26 in the control group) were included in the analyses (Figure 1).
Out of the 60 at-risk workers, the majority are men (88.3%), and most (80.0%) are over 40 years old. Additionally, most (80.0%) were married and had worked at the factory for over ten years. Approximately half (58.3%) worked more than 8 h daily, and half (50%) are currently smokers. There was no significant difference in the characteristics of samples between both groups (P > .05), as shown in Table 2.
Baseline General Characteristics of the Study Population.
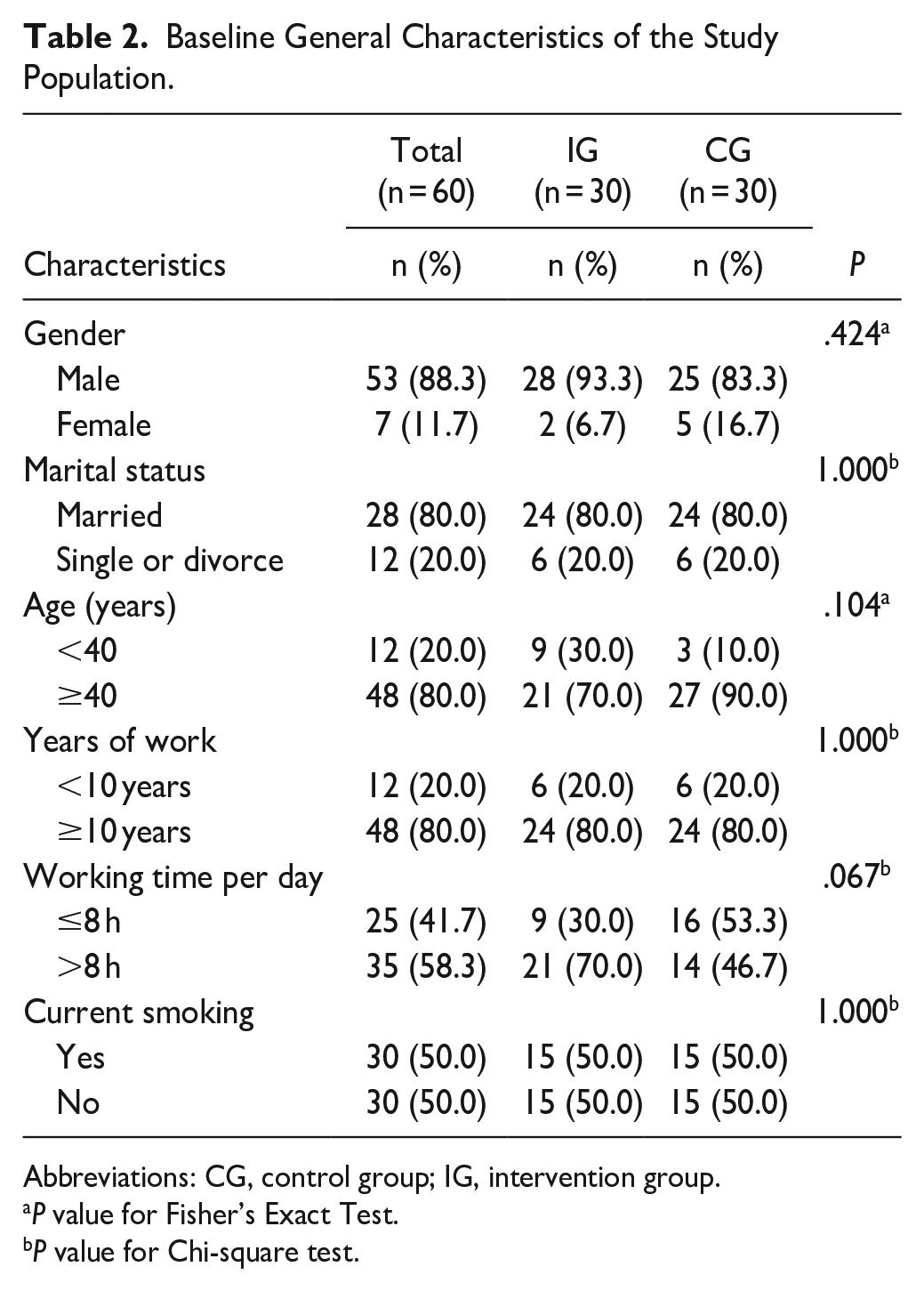
Abbreviations: CG, control group; IG, intervention group.
P value for Fisher’s Exact Test.
P value for Chi-square test.
The outcome variables (SBP, BMI, CVD risk, and smoking status) were measured 3 times at baseline (pre-intervention) and 1 month and 3 months after the end of the intervention. For systolic blood pressure (SBP), the results of a two-way repeated measures ANOVA comparing the mean SBP between the intervention and control groups revealed a significant difference (P = .016). Within-group analysis indicated that at least 1 pair of SBP measurements across time points differed significantly (F = 6.405, P = .007). Additionally, the interaction between groups and time points was significantly different (F = 12.136, P < .001) (Table 3). Figure 2 and Table 4 shows that within the intervention group, SBP was significantly different between 2 pairs of time points. Specifically, SBP decreased significantly from baseline to both the 1-month follow-up (Mdiff = 13.20, 95%CI 5.92, 20.48, P < .001) and the 3-month follow-up (Mdiff = 10.33, 95%CI 3.38, 17.28, P = .002). Comparisons of SBP mean difference between the intervention and control groups at 3 time points using a t-test showed significant differences at the 1-month follow-up (Mdiff = −10.97, 95%CI −17.22, −4.72 P < .001) and the 3-month follow-up (Mdiff = −10.67, 95%CI −16.60, −4.74, P < .001).
Repeated Measured ANOVA of SBP, BMI, and CVD Risk.

Abbreviations: BMI, body mass index; CVD risk, cardiovascular disease risk; df, degrees of freedom; MS, mean square; SBP, systolic blood pressure; SS, sum of square.
P value for Greenhouse Geisser.
P value for F-test.

Difference in mean scores for SBP, BMI, and CVD risk between intervention and control groups.
Pairwise Comparisons of the Mean Difference of SBP, BMI, and CVD Risk Between Each Pair of Time Points Within the Intervention and Control Groups.
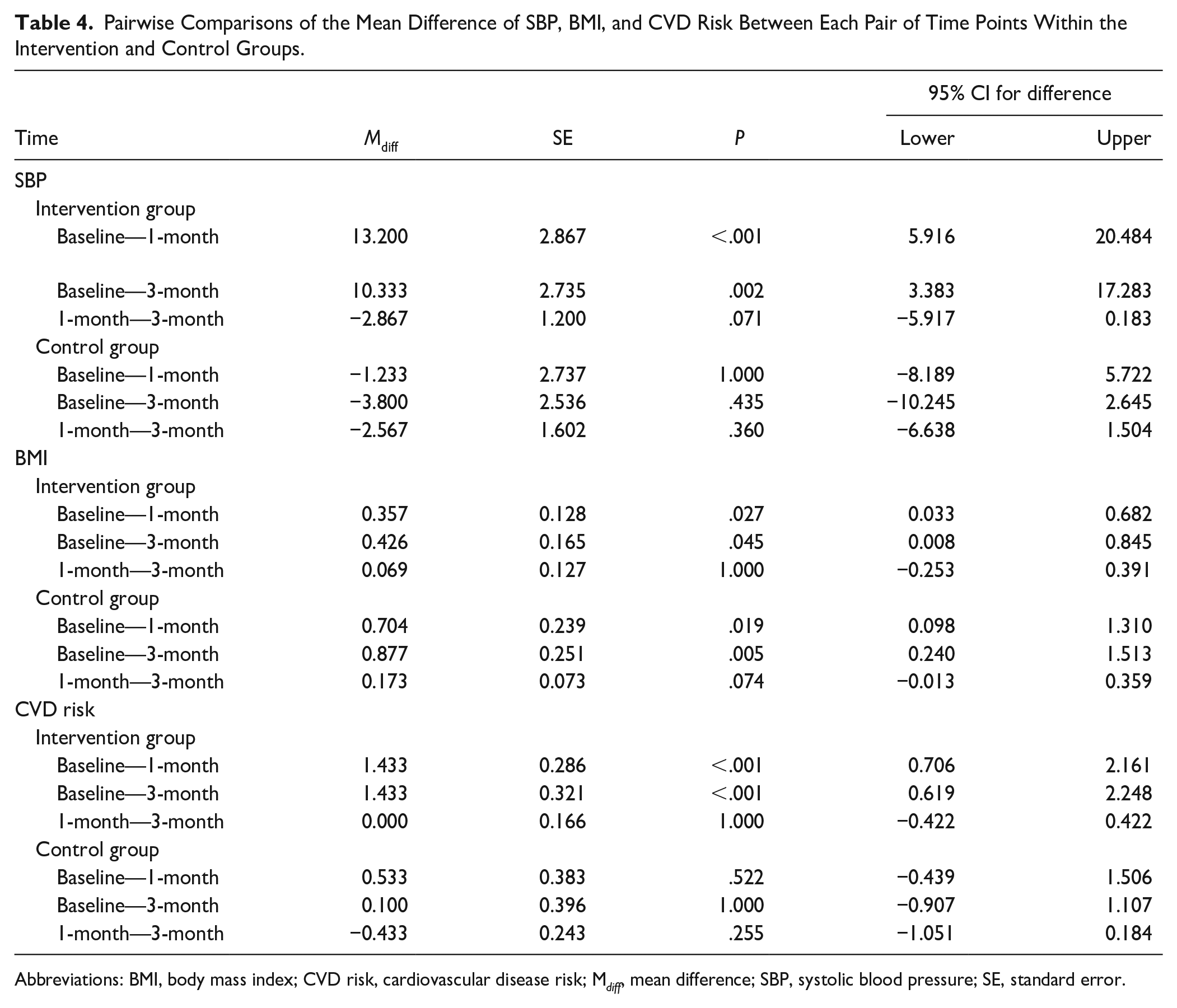
Abbreviations: BMI, body mass index; CVD risk, cardiovascular disease risk; M diff , mean difference; SBP, systolic blood pressure; SE, standard error.
Body mass index: As shown in Table 3, a two-way repeated measures ANOVA comparing the mean BMI between the intervention and the control groups showed no significant difference (P = .821). The overall within group indicated that at least 1 pair of the BMI by time interaction was different (F = 15.617, P < .001) and the interaction between groups and difference of time measure was not significantly different (F = 1.807, P = .169). In Figure 2 and Table 4, in the intervention group, the BMI compared baseline with 1- and 3-month follow-up was significantly decreased (Mdiff = 0.36, 95%CI 0.03, 0.68, P = .027; Mdiff = 0.43, 95%CI 0.01, 0.85 P = .045 respectively). Also, in the control group, the BMI compared baseline with 1- and 3-month follow-up was significantly decreased (Mdiff = 0.70, 95%CI 0.09, 1.31, P = .019; Mdiff = 0.88, 95%CI 0.24, 1.51, P = .005 respectively). The test for differences between the intervention and control groups on BMI showed no significant intervention effects.
For cardiovascular disease risk, two-way repeated measures ANOVA was performed to determine the differences of the interaction and main effects of the intervention on the CVD risk between 2 groups. The results of comparing the mean CVD risk between the intervention and the control groups showed significant difference (F = 9.854, P = .003). The overall within group indicated that at least 1 pair of the CVD risk by time interaction was different (F = 11.142, P < .001) and the interaction between groups and difference of time measure was significantly different (F = 4.827, P = .017) (Table 3). The CVD risk at three-time points of the intervention group was significantly different at 2 pairs of time points as shown in Figure 2 and Table 4. The results showed that the CVD risk compared baseline with 1- and 3-month follow-up was significantly decreased (Mdiff = 1.43, 95%CI 0.71, 2.16, P < .001; Mdiff = 1.43, 95%CI 0.62, 2.25, P < .001 respectively). The CVD risk showed significant difference between the intervention and the comparison groups at 1-month follow-up (Mdiff = −2.00, 95%CI −3.26, −0.74, P = .002) and 3-month follow-up (Mdiff = −2.43, 95%CI −3.79, −1.08, P < .001).
For smoking status (Table 5), the percentage of non-smokers was significantly higher in the intervention group (21 non-smokers, 75.0%) compared with the control group (12 non-smokers, 46.2%) after the 3-month follow-up (OR = 3.50; 95%CI 1.11-11.07; P = .030). However, at 1-month follow-up, the percentage of non-smokers was not significantly higher in the intervention group compared with the control group (OR = 1.50; 95%CI 0.54-4.17; P = .436).
Non-Smokers in the Intervention and Control Group at Pre- and Post-Intervention.

Abbreviations: CG, control group; IG, intervention group; OR, odds ratio; χ2, chi-square test.
P value for Chi-square test.
Discussion
The nurse-led workplace health promotion program (NWHPP) demonstrated significant improvements among at-risk workers particularly in SBP, smoking status, and CVD risk score. While BMI showed a positive trend in the intervention group, the difference compared to the control group was not statistically significant.
A significant reduction in SBP among at-risk workers is supported by previous research highlighting the efficacy of self-management education in improving blood pressure control. The NWHPP’s emphasis on self-management was pivotal in achieving these positive outcomes. Self-management plays a critical role by offering tailored behavioral counseling to at-risk workers. This counseling aims to assist individuals in modifying their risky behaviors to decrease the probability of encountering harmful outcomes associated with high-risk behaviors. By providing tailored behavioral counseling and increasing participants’ knowledge about blood pressure management, the NWHPP empowered individuals to make positive lifestyle changes. This approach is supported by studies such as Abdalla et al, 16 Delavar et al, 17 Gu et al, 18 and Kurnia et al 19 which highlight the importance of self-management, health education, and organizational-level interventions in improving blood pressure control.
The observed improvements in smoking cessation are consistent with previous research highlighting the efficacy of nurse-led interventions in promoting smoking cessation. Nurses’ comprehensive role in assessment, counseling, education, and support is vital for achieving these outcomes. Studies by Grech et al, 20 Ali et al, 21 and Qiu et al 22 support the notion that nurse-led programs can effectively reduce smoking behaviors. Additionally, in this study organizational support is vital for the success of workplace smoking cessation interventions. Measures such as tobacco control policies and employer support are often crucial for the effective implementation of these programs, as demonstrated by Le et al, 23 Chatdokmaiprai et al, 24 and Ayaz et al. 25
Reductions in SBP and smoking rates among participants affected a substantial decrease in their overall CVD risk score of the intervention group. Targeting these critical CVD risk factors proved effective in mitigating the risk of developing the condition. These findings align with the results of a systematic review by Abbate et al, 26 which indicated that lifestyle interventions successfully improved key CVD risk markers, including SBP. Moreover, a recent study by Lönnberg et al 27 mentioned that a lifestyle intervention offered in primary care can significantly improve cardiovascular risk factors and reduce the 10-year risk for CVD in high-risk adults. A nurse-led lifestyle intervention is vital for health promotion programs because nurses are responsible for assessing, counseling, educating, monitoring, coordinating, and advocating for individuals’ health, particularly in at-risk groups. These roles are critical in reducing the risk of CVD. Zheng et al’s 10 findings support this assertion, as they discovered that a nurse-led lifestyle intervention program successfully reduced cardiovascular risks.
While our NWHPP demonstrated significant improvements in other cardiovascular risk factors, the lack of a statistically significant difference in BMI between the intervention and control groups is noteworthy. It might be possible that the duration of the intervention (8 weeks) might have been insufficient to induce substantial weight loss. Similar findings have been reported in studies by Morgan-Bathke et al 28 and Aceves-Martins et al, 29 which found that while lifestyle interventions can influence weight loss, achieving statistically significant differences can be challenging. Although the NWHPP did not result in statistically significant BMI differences between groups, the observed trend towards BMI reduction in the intervention group is promising. Future research should focus on refining the program’s weight management components and extending the intervention duration to maximize its impact on BMI and overall health outcomes.
The NWHPP’s success in reducing CVD risk factors underscores the importance of workplace-based health promotion initiatives. By addressing modifiable risk factors and empowering employees, organizations can significantly impact the health and well-being of their workforce.
While the study provides valuable insights into the effectiveness of a nurse-led workplace health promotion program, it is essential to acknowledge its limitations. The sample size was relatively small, which may limit the generalizability of the findings to a larger population. Also, the three-month follow-up period might not be sufficient to assess the long-term impact of the intervention on CVD risk factors. The study did not assess the economic implications of the program, such as the cost-benefit ratio or return on investment. Addressing these limitations in future research can enhance the understanding of the program’s effectiveness and its applicability to broader populations.
Strengths of this study include rigorous methodology, targeted population, and multiple outcome measures, while the primary innovation of this study lies in its comprehensive approach to workplace health promotion. Focuses on redesigning healthcare services, strengthening self-management, and securing organizational support as core components of nurse-led programs distinguishes it from traditional workplace wellness initiatives. This multifaceted approach demonstrates a deeper understanding of the factors influencing employee health behaviors and the potential for sustainable change.
Conclusion
This study assessed the effectiveness of an 8-week nurse-led workplace health promotion program (NWHPP) in reducing cardiovascular disease (CVD) risks among at-risk Thai workers. Employing a randomized controlled trial design, the study measured changes in CVD risk, blood pressure, and smoking status over a three-month period. Our results show that the NWHPP significantly lowered systolic blood pressure, smoking rates, and overall CVD risk among participants. However, the reduction in BMI was not statistically significant.
These results underscore the potential of nurse-led interventions in improving cardiovascular health within workplace settings. By integrating health promotion into the organizational culture, workplaces can create environments that foster healthy behaviors and reduce the burden of CVD. Implementing comprehensive programs that include health assessments, behavior change support, and supportive workplace policies is crucial for achieving sustained improvements in employee well-being.
Footnotes
Acknowledgements
The authors wish to acknowledge the Department of Public Health Nursing, Faculty of Public Health, Mahidol University, Bangkok, Thailand, for their helpful contributions.
Author Contributions
All authors have involved in study conception and design. Arisara Ritngam and Surintorn Kalampakorn have involved in data collection. All authors have involved in data analysis and interpretation. Arisara Ritngam and Surintorn Kalampakorn have involved in drafting of the article. All authors have involved in critical revision of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Faculty of Nursing, Burapha University, Thailand.
Human Subjects Review Details
Approval date: August 31, 2020
Identification No.: COA. No. MUPH 2020-107
Name of the institution: The Ethical Review Committee for Human Research, Faculty of Public Health (PHIRB) of Mahidol University