
Abstract
Objectives:
This study aims at exploring the effects of physicians’ communication behaviors on patients’ satisfaction in primary care medical consultations in Chattogram, Bangladesh. The study used a quantitative research approach designed with a cross-sectional survey.
Methods:
Data were collected using post-consultation and facilitator administered questionnaire from the patients who visited the physician for medical consultation in different hospitals and clinics in Chattogram city. Seven hundred patients were included as the study participants. A hierarchical linear regression analysis was performed to examine the factors contributing to the outcome variables.
Results:
A statistically significant difference (P < .001) appeared regarding patients’ perception of adequate consultation, physicians’ nonverbal behavior, inhibiting behavior and patients’ participating behavior in private and public settings. However, R2 value shows that physicians’ patient-centered behaviors appeared as the stronger predictors of patient satisfaction toward medical interviews, followed by socioeconomic variables of patients and physicians and patients’ participation during the consultation. Presence of a third person with patients during consultation (β = −.05, P = .040), physicians’ private setting of consultation (β = .16, P < .001), physicians’ seniority (β = .05, P = .042), patients’ participating behavior during consultation (β = .20, P < .001), physicians’ nonverbal behavior (β = .10, P < .001), physicians’ inhibiting behavior (β = −.39, P < .001), and physicians’ facilitating behavior with patients (β = .32, P < .001) were reported as the influencing factors of patients’ satisfaction with medical consultation.
Conclusion:
This study suggests the profound impact of physicians’ patient-centered communication behaviors on patient satisfaction in primary care settings, overshadowing even socioeconomic factors and patient participation.
Keywords
Introduction
Globally, patient-physician conflict is a pervasive issue, impacting the efficacy of healthcare delivery.1 -3 However, effective communication between physicians and patients has been shown to strengthen relationships and reduce medical disputes. 4 Research consistently indicates a strong correlation between positive physician-patient communication (PPC) and improved healthcare outcomes, such as increased patient satisfaction,5,6 enhanced trust,7 -9 greater patient loyalty,10,11 and better health results. 12 Physician-patient communication encompasses the interactions and exchanges of information between two parties, forming the cornerstone of effective diagnosis, treatment, and ongoing management of health conditions.13 -15 Scholars argue that proficient communication is a critical component of healthcare, essential for fostering a deeper understanding of medical information. This understanding, in turn, promotes increased patient engagement, knowledge, and empowerment, ultimately enhancing decision-making processes in healthcare settings.2,13
The complexity of communication between physicians and patients extends beyond mere information exchange, encompassing biological, psychological, and relational dimensions of medical care. 16 Clinically, effective communication is not only crucial for providing top-quality care but also serves as a strategic element within patient care practices. This interaction includes both noticeable verbal and nonverbal behaviors.17,18 Abundant studies indicate that physicians’ nonverbal communication skills, including gestures and facial expressions, have a significant impact on patient satisfaction.19 -21 A study by Artati et al 22 found that verbal, haptic, and kinetic communications considerably affected patient satisfaction, with verbal communication being the most influential.
Moreover, the manner in which physicians interact during consultations is as critical as the content delivered. 23 Bertakis et al 24 observed that the type of questions—open-ended or closed-ended—asked during patient visits influenced satisfaction levels differently, with biomedical inquiries generally showing a negative correlation and psychosocial inquiries a positive one. They also noted that treatments focusing on psychosocial aspects positively affected patient satisfaction. Reflecting the importance of affective communication, Ben-Sira’s social interaction model 25 highlighted that a physician’s empathetic engagement, such as showing concern and dedicating sufficient time, is vital for positive patient evaluations. Further, Norton’s work26,27 on communication style emphasized how the manner of verbal interaction determines the reception and interpretation of medical information, identifying various styles like attentiveness and calmness that profoundly affect evaluations of medical care. 28 These insights suggest that enhancing communication skills in healthcare settings could significantly improve patient satisfaction and overall care outcomes.
Recent studies increasingly focused on the attitudes and behaviors of healthcare providers, illustrating their profound influence on patient satisfaction during physician-patient interactions. 29 These studies reveal that patients often assess their understanding and comfort with treatments based on social cues from physicians, such as tone of voice, personality traits, and mood. 30 This leads to an emphasis on the need for effective communication skills, empathy, and professional behavior in medical settings.4,9,15,31
Howard Giles’ Communication Accommodation Theory (CAT) posits that individuals adjust their communication styles—including speech, tone, and nonverbal behaviors—to match their conversational partners, thereby enhancing rapport and managing social differences. 32 This theory suggests that such adaptations, influenced by personal, contextual, and cultural factors, can significantly elevate patient satisfaction. 32 These adjustments not only facilitate smoother interactions but also signal social status and group identities, with social norms guiding the extent and appropriateness of communication accommodation.
Further exploring the dynamics of communication styles in healthcare, Buller and Buller 28 examined how affiliative and controlling communication styles, along with eight social characteristics of medical interviews, impact patient satisfaction. Their findings indicate that effective communication is strongly linked to positive evaluations of medical treatment, underscoring communication as a crucial aspect of medical competence. Specifically, affiliative communication styles were associated with increased patient satisfaction, whereas controlling styles tended to reduce it, highlighting the critical role of adapting communication to patient needs and preferences.
Moreover, various elements including the physician’s age, their specialty, the patient’s health status, and prior medical visits have been shown to influence how communication affects treatment evaluations. Despite these variables, psychosocial factors consistently emerge as a primary concern for patients during their initial consultations.33,34 Research across different medical conditions indicates that attention to psychosocial concerns positively affects treatment outcomes. 35
Patient satisfaction is further shaped by socio-demographic, cognitive, and contextual factors. Edelmann 36 identified key determinants affecting the physician-patient relationship, which include characteristics of both the physician (eg, gender, experience) and the patient (eg, gender, social class, age, education, information needs), along with disparities in education, social class, attitudes, beliefs, and expectations. Factors such as the patient load and the extent of interaction also play critical roles. Additionally, Adhikari et al 37 found that socio-demographic characteristics like age, gender, and ethnicity substantially affect overall patient satisfaction, with age often being the most decisive factor across different dimensions of satisfaction. Education, occupation, income level, and religion were also noted to influence various facets of patient satisfaction in studies by Akthar et al 38 and Azharuddin et al 39
This study aimed at investigating the impact of physicians’ communication behaviors on patient satisfaction across various public and private healthcare settings in Chattogram, Bangladesh. Despite previous efforts being somewhat limited in gathering patient perspectives on service satisfaction in Bangladesh, particularly concerning the specific relationship between physicians’ communication behaviors and patient satisfaction during primary care consultations, some studies have explored the quality of services in both government and private hospitals and their impact on patient satisfaction.40 -44 Nonetheless, a substantial gap persists in the scholarly examination of how physicians’ communication styles influence patient satisfaction within the Bangladeshi context, which this study aims to fill. So, the objective of this study is to investigate the impact of doctors’ communication behaviors on patient satisfaction within various government and private medical settings in Chattogram, Bangladesh and to identify factors that either enhance or hinder patient satisfaction during medical consultations.
Conceptual Framework
To conduct our analysis, we utilized a conceptual model (Figure 1) introduced by Zandbelt et al 45 to comprehend the determinants of patient satisfaction during individual medical interviews. This model was developed based on the frameworks proposed by Ong et al 46 and Mead and Bower. 47 It hypothesized that various factors influence patients’ satisfaction, adherence to prescribed medication, and overall health status across different levels. The researchers focused on background characteristics, physicians’ patient-centered communication, and patient participation-related variables as key potential factors of patient satisfaction. To explore these relationships, we employed three distinct models. Background characteristics encompassed patient traits (socio-demographic factors, health status, and information preferences), visit characteristics (familiarity, presence of a third party), and physician attributes (socio-demographic and professional aspects). Furthermore, physicians’ patient-centered communication included both facilitating and inhibiting behaviors, while patient participation referred to the extent of patients’ involvement in the conversation and their participatory behavior.
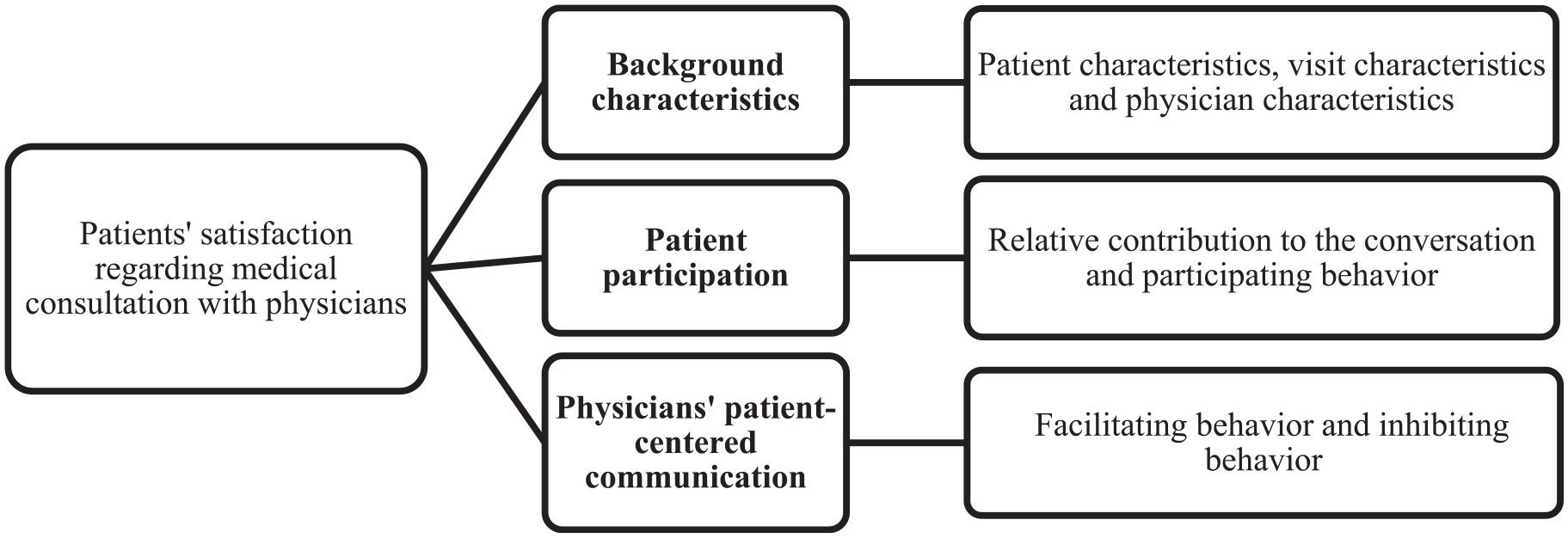
Conceptual framework to identify factors influencing patients’ satisfaction with medical consultation.
Methods
Study Design, Sampling Procedures and Sample Size
The study design employed in this research aimed to attain specific research objectives by utilizing a quantitative research methodology structured around a hospital-based cross-sectional survey. The study focused on elucidating the descriptive aspects related to patient satisfaction with physician-patient communication behaviors during primary care medical consultations within the public and private hospitals of Chattogram, Bangladesh. Ethical approval was taken from the Institutional Review Committee of the University of Chittagong, Bangladesh. All individuals seeking primary care medical consultations at various government hospitals and private health centers constituted the study population. The project utilized a hospital/clinic-based cross-sectional approach, employing purposive sampling to select the study area and convenience sampling to choose study participants. Chittagong Medical College and Hospital (CMCH) was purposively chosen for government hospital patients due to its diverse patient population, while two private clinics in Chattogram city were selected from private medical centers to provide a comparative public setting. Study participants from both government and private settings were selected through convenience sampling. The sample size was determined using the single population proportion formula under the assumptions of P = 50%, significance level of 5% (α = .05), Z = 1.96, margin of error of 5% (d = 0.05), and design effect of 2. A total of 768 patients were invited to participate in the study, with 700 individuals completing the questionnaires, resulting in a response rate of 91.15%.
Data Collection
Data collection involved using a structured questionnaire administered by graduate students. The questionnaire had five parts including consent, background characteristics, physician-patient communication, patient participation, and patient satisfaction. Facilitators had previous data collection experience and guided the survey process. Patients received information about the questionnaire before meeting the physician to reduce reporting errors. The goal and confidentiality of the study were explained to the respondents before the distribution of questionnaires. After the explanation, each participant gave their written informed consent to take part in the study. Self-reported data from patients in the study depicted various aspects of physicians’ behavior. Communicating ideas to patients before the physician’s visit helped achieve research goals by minimizing reporting errors. Data collection in Bangladesh does not involve documenting medical consultations, unlike in developed countries. Therefore, we relied on self-reported patient information through a post-visit questionnaire, with limitations in obtaining exact data. 48
Outcome Variables
Patients’ satisfaction with their medical consultations was the dependent variable in this study. It was assessed using the “Medical Interview Satisfaction Scale (MISS-21),” which consists of 21 items adapted by Meakin and Weinman. 49 We used a seven-point Likert scale from 1 (strongly disagree) to 7 (strongly agree) to measure each item related to patient satisfaction. The scale was modified from the original Medical Interview Satisfaction Scale (MISS-29) developed by Wolf and Stiles 50 that was used in different studies performed in general practices.51 -53
Independent (Explanatory) Variables
Patient characteristics-related variables were patients’ education, patients’ gender, monthly household income, area of residence, patients’ information preference, perception of self-communication skill, and perception of self-knowledge.
Visit characteristics-related variables were patients’ acquaintance with the physician, presence of a third person (family member, relative, friend) during the consultation.
Physicians’ characteristics-related variables were physicians’ gender, physicians’ age, physicians’ setting of consultation, physicians’ seniority, patients’ perception of adequate consultation, appointment length, and the necessity of diagnosis suggestion.
Physicians’ nonverbal behavior (making eye contact, nodding), physicians’ inhibiting behavior (interrupting the patient, dismissing patient concerns), physicians’ facilitating behavior (actively listening, encouraging patient questions) were used as physicians’ patient-centered communication variables.
Patients’ participating behavior, and patients’ relative contribution to the conversation were used as the variables related to patient participation.
Content Validity and Reliability
In the first stage, items of the MISS-21 were translated from English text into Bengali as the original scale was in English and the target study participants were Bengali patients. A translation of the MISS-21 into Bangla was completed by two translators (one was a psychologist, and the other was the author of this manuscript). They were native Bangla speakers and knowledgeable of assessment principles and had in-depth knowledge of native Bangla language. They evaluated the meaning of the equivalence of items. The expert panel then judged the forward translated form of the scale to determine whether there were any differences in the two versions. A back translation of the scale (ie, translating items from Bangla to the original English) was completed by two language experts (one was a linguist, and the other was a faculty member in English). The expert panel further judged the back-translated form of the scale, suggesting that the translation was an appropriate version of the original English scale. After evaluating the two translations, the expert panel finalized the MISS-21-B. Afterward, The MISS-21-B was compared with the original English scale. At first, the original MISS-21 was administered to 30 respondents who would have enough knowledge of both the Bangla and English languages. A few days later, the MISS-21-B will be administered to 30 respondents (the respondents who would not participate in the original MISS-21 study). A significant positive correlation (r = .939, P < .01) between the two versions of the scale indicated that the MISS-21-B was an appropriate translated version of the original MISS-21. The reliability of the scale was also checked, and Cronbach’s alpha (α = .96) value suggested very good internal consistency of the scale.
Statistical Analysis
The data were coded and entered into IBM SPSS version 24.0. Comparisons among multiple groups regarding the overall mean score of respondents’ MISS-21 score were made using appropriate inferential tests such as a two-tailed t-test and one-way analysis of variance (ANOVA) and Pearson correlation. To estimate the proportion of variance in MISS-21 that can be accounted for by the background characteristics, patient participation and physicians’ patient-centered communication-related factors, a hierarchical linear regression analysis was performed. As the proposed study is designed to be conducted among a large sample and the dependent variable was continuous (the range of the sum of the MISS-21 scale was between 21 and 105), the linear regression was run as the parametric test. The variables with a P < .05 in t-test and ANOVA were included in linear regression models to determine the predictors of better patient satisfaction scores.
The multicollinearity was checked by examining the tolerance value (TV) and variance inflation factor (VIF) value in collinearity statistics. In total, three models were fitted to predict the determinants of patients’ satisfaction with the medical interview. In hierarchical regression, step 1 assessed the determinants of a better MISS-21 score by background variables. Step 2 explored the effects of background variables and patient participation-related factors, while step 3 (final model) examined the respondents’ background variables, patient participation, and physicians’ patient-centered communication-related factors. In the model summary, ANOVA values (P < .001) of each step for the overall MISS-21 score report that our hierarchical regression model performed well and was a good predictor of the main outcome variables. R2 of each step was changed considerably and significantly, and F changes were also statistically significant (P < .001). Variables having a p-value < .05 in the regression analysis were taken as significant predictors.
Results
Background and Visit Characteristics of Study Participants
Table 1 shows the socio-demographic characteristics of the study participants. The mean education years of the study participants was 9.69 (±5.01). Of them, 157 (22.4%) attained up to class 5, while 273 (39.0) completed up to Secondary School Certificate (SSC) and 270 (38.6%) had an education of more than SSC. Among the study participants, 399 (57%) were female, whereas 301 (43%) were male. Among the study participants, 422 (60.3%) had monthly household income up to Bangladeshi Taka (BDT) 20 000, whereas 278 (39.7%) had an earning of BDT > 20 000. The majority of the respondents (486, 69.4%) were from urban areas. Among the study participants, 332 (47.4%) preferred detailed information from the physicians, while 368 (52.6%) preferred brief information. Of the patients, 386 (55.1%) had a perception of having good oral communication skills, while 314 (44.9) perceived being poor in verbal communication.
Background and Visit Characteristics of Study Participants (N = 700).

Abbreviations: BDT, Bangladeshi Taka (Currency); SSC, Secondary School Certificate.
Table 1 also illustrates patients’ perceived severity of disease, reporting that 363 (51.9%) perceived that they were affected by a severe problem, while 337 (48.1%) thought that they had a mild problem. Of the study participants, 216 (30.9%) were acquainted with their physician, and 484 (69.1%) were new patients. For 364 patients (52%) there was a third person (family member, relative) present during the medical consultation, whereas 336 (48%) were not accompanied by anyone.
Socio-Demographic and Work-Related Characteristics of Physicians
Table 2 indicates the gender of the physician, reporting that 420 (60%) patients consulted with a male physician, while 280 (40%) had an interview with female physicians. An equal number of patients (350, 50%) visited physicians in a public hospital versus a private clinic. Three-fourths of the patients (528, 75.4%) visited the physicians with lower seniority, while the remaining one-fourth (172, 24.6%) consulted with the physicians who held high positions in their profession. Most patients (n = 290, 41.4%) visited physicians in the Medicine department.
Physicians’ Socio-Demographic, and Work-Related Characteristics.

Physicians’ Behavior and Patient Satisfaction
Regarding the specific communication behaviors impacting patient satisfaction, Table 3 presents patients’ perception of the adequacy of consultation length with 38% rating it as “good” or “very good.” Additionally, 38% of the patients experienced physicians’ non-verbal behaviors frequently (27% frequently + 11% very frequently), while 83% of the respondents reported rarely experiencing inhibiting behaviors from physicians. Of the patients, 29% participated “much” or “a great deal” in expressing concerns, asking for information, and stating treatment preferences. Regarding patients’ satisfaction levels, 62% of the patients reported high satisfaction with their medical consultations. In public medical settings, only 43% of the patients were highly satisfied with medical consultations, while in private medical clinics, 80% of the patients had a high level of satisfaction.
Different Variables Relating to Physicians’ Behavior and Patient Satisfaction (N = 700).

Table 4 depicts that different independent variables of the study are highly correlated with each other that were statistically significant (P < .001).
Correlation Among the Independent Variables (N = 700).

P < .001.
Regression Analysis for Variables Predicting Patients’ Satisfaction
The model summary for the linear regression predicting patients’ satisfaction with medical consultation is shown in Table 5. Additionally, Table 5 also provides the analysis of variance and the β coefficients. A positive β value means that as the predictor variable increases, the dependent variable also increases. Conversely, a negative β value means that as the predictor variable increases, the dependent variable decreases. The hierarchical multiple regression reveals that in model 1, among the seven predictors of patients’ satisfaction, patients’ acquaintance with the physician (β = .10, P = .006), physicians’ private setting of consultation (β = .45, P < .001), and visiting a female physician (β = .08, P = .025) contributed significantly to the regression model (F = 30.46, df = 7, P < .001) and accounted for 24% of variation in the outcome variable.
Multiple Linear Regression Analysis With Model Summary Depicting Factors Influencing Patients’ (N = 700) Satisfaction in Medical Consultation.

Dummy variables (1 = yes, 0 = no); §Continuous variable; ANOVA = One-way analysis of variance.
Background characteristic of patients and physicians.
Patients’ participation in medical consultation.
Physicians’ behavior in medical consultation.
Adding the other two predictors in model 2 explained an additional 20% variation (∆R2 = 0.20, ∆F = 117.95, P < .001) in patients’ satisfaction above and beyond the effects of the predictors in model 1. In model 2, among the nine predictors of respondents’ patients’ satisfaction with medical consultation, presence of third person with patients during consultation (β = −.10, P = .001), physicians’ private setting of consultation (β = .27, P < .001), visiting a female physician (β = .08, P = .009), patients’ relative contribution to the conversation (β = .19, P < .001), and patients’ participating behavior (β = .41, P < .001) contributed significantly to regression model (F = 57.91, df = 9, P < .001) and accounted for 43% of variation in the outcome variable.
Introducing the other three predictors in model 3 explained an additional 25% variation (∆R2 = 0.25, ∆F = 197.27, P < .001) in patients’ satisfaction above and beyond the effects of the predictors in step 2. In model 3, among the nine predictors of patients’ satisfaction with medical consultation, presence of third person with patients during consultation (β = −.05, P = .040), physicians’ private setting of consultation (β = .16, P < .001), physicians’ seniority (β = .05, P = .042), patients’ participating behavior during consultation (β = .20, P < .001), physicians’ nonverbal behavior (β = .10, P < .001), physicians’ inhibiting behavior (β = −.39, P < .001), and physicians’ facilitating behavior with patients (β = .32, P < .001) contributed significantly to the regression model (F = 129.82, df = 12, P < .001) and accounted for 69% of variation in the outcome variable. Model 3 was employed to explain appropriately to patients’ satisfaction.
Discussion
Our study reveals that 38% of patients felt that the adequacy of consultation length with physicians was good or very good. Conversely, 63% reported satisfaction with the duration of their consultations, which they described as ranging from acceptable to very poor. Notably, a higher percentage (62%) of patients expressed greater satisfaction when consultations involved more extensive interaction with their physicians. This emphasizes the importance of longer consultation times for enabling personalized conversations that are critical for fully understanding and effectively addressing patient needs. Supporting this, a study by Wang et al 54 found that consultations lasting 10 to 20 min were associated with higher completion rates of recommended checklist items and improved diagnostic accuracy, thereby enhancing patient satisfaction and treatment outcomes. Similarly, findings by Srinivas and Salah 55 indicated that longer visits typically lead to increased patient satisfaction due to more thorough care. Tadeu et al 56 also reported that longer consultations, often exceeding 15 min, allow for more comprehensive care, which correlates with higher satisfaction levels. These findings collectively affirm the positive impact of extended consultation durations on patient satisfaction and healthcare quality.
Our study revealed that 76% of patients experienced positive non-verbal communication from their physicians, ranging from occasionally to very frequently, while 24% reported seldom or never receiving such cues. These statistics underline the significant role of non-verbal communication in enhancing patient satisfaction. This finding is supported by Mast, 57 who demonstrated that non-verbal behaviors such as eye contact and physical proximity are correlated with increased patient satisfaction. Similarly, Montague et al 58 found that social touch could enhance feelings of empathy. Furthermore, Marcinowicz et al 59 noted that patients often perceive non-verbal cues like tone of voice, eye contact, and facial expressions as critical, significantly influencing their satisfaction by improving the therapeutic relationship. Recent studies by Mohd Salim et al 60 and Zhang et al 15 also emphasize that these non-verbal interactions make patients feel valued and understood, which is crucial for their overall satisfaction.
Patient participation in expressing concerns, requesting information, and discussing treatment preferences varies significantly, influenced by numerous factors. Our findings show that while 12% of patients displayed limited interest in these activities, 8% were highly proactive, and a significant 80% were keen to engage actively with their physicians. This engagement trend is echoed in diverse healthcare contexts; for example, Sankar et al 61 observed that in India, cancer patients often actively seek information, yet typically adopt a passive role in decision-making, with considerable family participation influencing their actions.
Recent studies highlight the essential role of effective, patient-centered communication in enhancing patient satisfaction and overall healthcare outcomes.62,63 Goldstein et al 64 highlight that physicians consider diagnostic tests essential for effective patient management, yet there exists a notable discrepancy in practice: in our study 57% of patients reported their physicians recommended diagnostic tests, while 43% received no such recommendations. This inconsistency points to a critical need for consensus-based guidelines on the utilization of common laboratory tests among medical inpatients, as emphasized by Ambasta et al 65 Furthermore, patients’ perceptions of the necessity of these tests vary significantly, with some viewing them as essential and others as unnecessary, a variation that Noiseux et al 66 also observed.
Factors Associated With Patient Satisfaction Toward Medical Consultation
Through multiple linear regression analyses, this study highlights factors that augment or impede patients’ satisfaction with physicians’ medical interviews. It is noteworthy that one of our specific objectives was to explore the comparative strength of socioeconomic factors of patients and physicians, patients’ participating behavior, and physicians’ patient-centered behaviors in predicting patients’ satisfaction with medical consultation. A comparison of R2 value shows that physicians’ patient-centered behaviors appeared as the stronger predictors of patient satisfaction toward medical interviews, followed by socioeconomic variables of patients and physicians, and patients’ participation during the consultation.
Previous studies suggest that physicians’ patient-centered communication behaviors contribute to patients’ satisfaction, adherence to the medication, adaptation of healthy lifestyles, ensuring the follow-up visit and improvement of the patient’s health that lead to health promotion and development.67 -70 This hypothesis is supported by our study findings that report the physicians’ inhibiting behavior as the strongest predictors of outcome variable, followed by physicians’ facilitating behavior with patients and non-verbal behavior. 57 Letting the patient talk without interruptions also appeared as the most important factor in patient satisfaction in a previous study. 71 In addition, the findings that report physicians’ patient-centered communication behaviors as the most important factor for patient satisfaction align with numerous studies conducted in Bangladesh44,72 and other countries.68,69,73 -75 In a systematic review study, Moslehpour et al 69 found that verbal and nonverbal indirect interpersonal communication was associated with patients’ satisfaction, while physicians’ interpersonal communication skills had a significant effect on low-income patients’ satisfaction levels in Indonesia, 73 Denmark, 75 Switzerland, 72 and the USA. 74
A growing body of literature indicates that patients who play a more active role are also more pleased with the care, provide more input and guidance from physicians, are more dedicated to treatment plans, have a greater understanding of treatment choices, report more substantial health benefits and are more satisfied than more passive patients. 76 Patients often hesitate to participate if physicians do not encourage them to ask questions. Besides, patient satisfaction depends on the response behavior of the physician. Usually, the physicians who cheer the patient to ask questions are more likely to respond to the patients’ questions.4,48 We also found a positive correlation between the two items. Our finding also agrees with the literature reporting that patients with more participatory behavior were more satisfied with individual medical consultations.
Provider characteristics can also affect interaction. For example, the higher rank of physicians has attracted a lot of attention as a potential source of difference in the interpersonal aspects of medical practice, with theories that senior physicians tend to utilize more patient-centered communication and facilitate more open and equitable interchange as most of them visited patients in private settings. 77 Senior physicians participate in dialog that is analyzed based on the wider lifetime background of the circumstances of patients by discussing psychosocial problems through relevant questioning and therapy, increased use of more supportive talk, and more positive patient inputs; these elements provide a trend that can be commonly regarded as a patient-centered medical consultation.
Our study found that the presence of a third person, for example, friends and family members, during the medical encounter was associated with patients’ satisfaction. The possible explanation might be due to the fact that family members accompanying the patients often express their anxiety and express their opinion during medical consultations while patients are unable or hesitant to talk to the physician. Wong et al 76 also found that when patients’ families had enough opportunity to speak to the physician, it significantly affected patients’ satisfaction.
This study, while providing insightful observations about the impact of physician-patient communication on patient satisfaction in Bangladesh, has some limitations. First, the sample size may not fully represent the diversity of the Bangladeshi population, including rural versus urban differences in healthcare experiences. Second, the subjective nature of patient satisfaction and self-reported measures might introduce social desirability bias in the responses. Third, the study primarily focuses on verbal and non-verbal communication without deeply exploring the systemic and organizational factors that might influence these interactions, such as workload, institutional policies, or technological resources.
Nonetheless, the findings of this study carry significant implications for healthcare practice in Bangladesh. Enhancing patient-centered communication and ensuring adequate consultation time are crucial steps toward improving patient satisfaction and healthcare outcomes. Healthcare training programs should incorporate modules on effective communication strategies, emphasizing non-verbal cues and patient engagement techniques. Hospitals and clinics might consider revising their policies to allow for longer consultation times and more patient involvement in decision-making processes, potentially leading to better adherence to treatment plans and improved health outcomes.
Conclusion
Our study highlights the critical role of effective communication in enhancing patient satisfaction within healthcare settings in Bangladesh. While a majority of patients reported satisfaction with the duration of their consultations and the quality of non-verbal communication from their physicians, a significant minority indicated a need for improvement in these areas. This finding suggests that extending consultation times and enhancing the quality of both verbal and non-verbal interactions could lead to higher patient satisfaction and better healthcare outcomes. Furthermore, active patient participation, influenced by a range of factors including demographic characteristics and the presence of family members, is crucial for fostering satisfactory medical encounters. This study also highlights a gap between medical advice and patient perceptions, emphasizing the need for clearer communication and more personalized consultations to ensure patient understanding and comfort with prescribed diagnostic tests and treatments. Future healthcare practices and training should focus on enhancing patient-centered communication skills among physicians, thereby promoting more effective interactions and better overall health outcomes. Despite its limitations, such as diversity and representativeness of the sample and potential response biases, this study contributes valuable insights into the dynamics of physician-patient communication in Bangladesh, offering a foundation for future research and improvements in healthcare practice.
Footnotes
Data Availability
All of the primary data has been included in the results. Additional materials with details may be obtained from the corresponding author if required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Mid-term Evaluation of 14th Five Year Plan for National Healthcare Insurance funded by Center for Bigdata Research in Medical Insurance & Health Policy, Project of Evaluation of Chronic Disease Health Management Policies (Project No. 2023-SKY-A07054-0010) and the Research and Publication Office of the University of Chittagong, Bangladesh (Project No. 601/2020).
Informed Consent
Informed consent was obtained from participants prior to completing the survey.
Research Involving Human Participants
This research was approved by the Institutional Review Board of University of Chittagong, Bangladesh (CU-SOC-21-0007).