
Abstract
Background:
Escalating street violence and criminal homicides have an adverse impact on psychological well-being. However, these consequences have been difficult to evaluate. Using a recently validated scale, we aimed to assess the impact of fear of crime on the psychological status of middle-aged and older adults living in a rural setting afflicted by endemic violence.
Methods:
Participants were selected from Atahualpa residents included in previous studies targeting psychological distress in the population. A validated scale was used to objectively quantify fear of crime in participants. Differences in symptoms of depression and anxiety between baseline and follow-up were used as distinct dependent variables and the continuous score of the fear of crime scale was used as the independent variable. Linear regression models were fitted to assess the association between the exposure and the outcomes, after adjusting for relevant confounders.
Results:
A total of 653 participants (mean age = 53.2 ± 11.5 years; 57% women) completed the requested tests. We found a 13% increase in symptoms of depression and anxiety during the peak of violence in the village compared with previous years. Linear regression models showed a significant association between the total score on the fear of crime questionnaire and worsening symptoms of depression (β = .24; 95% CI = 0.14-0.35) and anxiety (β = .31; 95% CI = 0.24-0.37), after adjustment for relevant confounders.
Conclusions:
This study shows a significant aggravating effect of fear of crime on pre-existing symptoms of depression and anxiety and a deleterious effect of these conditions on overall well-being.
Introduction
Ecuador ended the year 2023 with its worst record of street violence in its history. A total of 7592 criminal homicides were reported across the country, which represents a rate of 43.94 cases per 100 000. This compares with 2019 when the official rate of criminal homicides was 6.84 per 100 000 inhabitants, consistent with 7-fold increase over the past 5 years. 1
Criminal violence is associated with an increased frequency of monetary extortions and kidnappings, all of which provoke fear, anxiety, and depression, as well as causing restrictions in daily activities. Living in fear and being forced to remain at home further results in a loss of economic productivity and constraints on outdoor leisure activities. Clearly, such changes have a deleterious effect on overall quality of life and are likely to result in downstream adverse effects on the psychological well-being of the affected population. 2
There is a substantial body of research on the impact of community violence, but the overwhelming majority deals specifically with the impact on children and adolescents. 3 There is limited documentation of the effect of fear of violence on older adults. That which has been done tends to address the cumulative impact of earlier traumas, or has been qualitative, rather than quantitative.4,5
Over the past 12 years, our group has conducted several epidemiologic studies on various health conditions prevalent in middle-aged and older adults living in Atahualpa, a rural village located in coastal Ecuador.6-9 This village and its neighboring communities have traditionally been considered safe and peaceful but even here, the homicide rate increased by 143% in just a few years. 10 Relying on baseline data previously established in this population, we assessed recent worsening in psychological well-being in order to ascertain the role of fear of crime in mediated these changes.
Methods
Study Population
This study was comprised of community-dwelling middle-aged (40-59 years) and older adults (≥60 years) who were actively enrolled in the Atahualpa Project cohort up to January, 2024. As detailed elsewhere, this is an open population-based cohort with original enrollment taking place from 2012 to 2019.6-9 Participants were identified by means of door-to-door surveys and followed-up by periodic home visits where interviews and complimentary exams were offered to all of them. Individuals share several characteristics that reduce the likelihood of confounding variables. The population is homogeneous regarding race/ethnicity (Amerindian ancestry), low levels of education, dietary habits, and low socio-economic status. The migration rate is low and retention in the study is high, providing an ideal setting for carrying out longitudinal prospective studies.
Study Design
Following a longitudinal population-based study design, we used data on psychological well-being collected for the Atahualpa Project cohort prior to the waves of violence and crime that later struck the village. We then compared these baseline results with updated surveys carried out in January 2024, when extortions, kidnappings and homicides were at their peak. Only individuals who agreed to sign a new comprehensive informed consent were included in the current study. The protocol was approved by the Ethics Committee of Hospital-Clínica Kennedy, Guayaquil (FWA 00030727). Aggregated data will be shared from the corresponding author upon reasonable request.
Background Data
Prior to the escalation of violence in the village, we collected data—for research purposes—on demographics and other conditions of interest (see below), as well as on symptoms of psychological distress. This information was used for comparison purposes in the present study. Psychological distress was assessed with the depression and anxiety axes of the depression-anxiety-stress 21 scale (DASS-21). 11 This is a validated scale that has been shown to have good internal reliability (Cronbach’s alpha values ranging from .84 to .91), 12 and that provides quantitative measures of symptoms of depression (dysphoria, hopelessness, devaluation of life, self-deprecation, lack of interest/involvement, anhedonia, and inertia), and anxiety (autonomic arousal, skeletal muscle effects, situational anxiety, and subjective experience of anxious affect). Responses are rated on a 4-point Likert scale ranging from 0 (not at all) to 3 (almost always) with a maximum total score of 21 for each axe. 11 Scores of ≥5 points are considered to be symptoms of depression and ≥4 points symptoms of anxiety.
Data Collected for the Present Study
The DASS-21 scale was again administered to all study participants. Follow-up interviews were performed by the same investigators who obtained the baseline data and were already acquainted with the study population, with the aim of reducing bias by minimizing elusive responses to questions about fear and insecurity. In addition, we introduced a recently validated “fear of crime” questionnaire that includes 4 key items rated on a Likert scale: (1) how fearful are you of crime in your village, ranging from 1 (not fearful at all) to 4 (very fearful); (2) how do you perceive the crime rate in your village compared to neighboring villages, ranging from 1 (very low) to 3 (about the same) to 5 (very high); (3) how dangerous or safe it is to walk in your village during the daytime, ranging from 1 (completely safe) to 4 (extremely dangerous); and (4) how dangerous or safe it is to walk in your village after dark, ranging from 1 (completely safe) to 4 (extremely dangerous). 13 This questionnaire has a minimum score of 4 points and a maximum of 17, with higher scores indicating a greater fear of crime. The instrument was translated from English to Spanish and then back-translated to English by bilingual speakers from our group, and the questions were then tested for reliability in a random sample of 50 individuals.
Covariates Evaluated
Information about age at baseline, sex, level of education (elementary school or higher), occupation (working or retired/unemployed), social risk and sleep quality were selected as relevant covariates in all models. Age, sex, level of education and occupation were collected by self-report. Social risk was assessed by the Gijon’s Social-Familial Evaluation Scale (SFES). 14 This instrument rates 5 risk situations (social determinants of health) that include family situation, economic status, housing, social relationships and support networks. Each of these components is comprised of 5 questions weighted on a 1 to 5 scale, for a maximum score of 25, with higher scores indicating greater social risk. This scale was selected due to its appropriateness to the living conditions of the study population. 15 Sleep quality was assessed by means of the Pittsburgh Sleep Quality Index (PSQI). 16 This field instrument basically discriminates between “good” and “poor” sleepers. The PSQI consists of 19 items grouped into 7 components (sleep duration, sleep disturbances, sleep latency, daytime dysfunction due to sleepiness, sleep efficiency, overall sleep quality, and medications needed to sleep). Each component is weighted on a 0 to 3 scale for a maximum score of 21 points, with >5 points indicating a poor sleep quality.
Sample Size Calculation
During the design of the study, it was hypothesized that the proportion of subjects with worsening anxiety would likely double among subjects with high fear of crime. Background proportion was hypothesized to be 10%, OR = 2.0, 80% power to detect a double-sided difference of at least twice the estimated proportion. Total sample size required of 472 subjects. A secondary objective was to expect roughly the same difference for (OR = 2.0) for worsening depression.
Statistical Analysis
Data analyses were carried out using STATA version 18 (College Station, TX, USA). In unadjusted analyses, continuous variables were compared by linear models and categorical variables by the chi-square or Fisher exact test as appropriate. Differences in the continuous scores of symptoms of depression and anxiety between baseline and follow-up were used as distinct dependent variables (outcomes) and the continuous score of the fear of crime scale (exposure) was used as the independent variable. Separate linear regression models were fitted to assess the association between the exposure and the outcomes, after adjusting for age, sex, level of education, occupation, social risk, and sleep quality. Levels of depression and anxiety at baseline were included in these models to estimate the potential impact of previous psychological status on the investigated outcomes.
Results
Recruitment Process
Of 933 individuals aged ≥40 years enrolled in the Atahualpa Project Cohort up to June 2019, 51 (5%) did not received the DASS-21 at baseline. Of the remaining 882 participants, 653 (74%) were enrolled in the present study as they completed the follow-up depression and anxiety axes of the DASS-21 as well as the questionnaire assessing fear of crime. Figure 1 depicts the reasons for excluding participants at each stage of the enrollment process. The high number of deaths during the follow-up period was mostly related to the SARS-CoV-2 pandemic, which severely struck the village starting in the first trimester of 2020. 17

Flow chart depicting the reasons for excluding potential participants at each stage of the enrollment process.
Characteristics of Participants at Baseline
The mean age (at baseline) of the 653 participants was 53.2 ± 11.5 years, 369 (57%) were women, 326 (58%) had elementary school education only, 94 (14%) were retired/unemployed, 292 (45%) had poor sleep quality, and the mean score in the SFES was 9.8 ± 2.6 points (median: 10 points). At baseline, the mean score on the depression axis of the DAAS-21 was 1.6 ± 2.1 points and that one of the anxiety axes was 1.6 ± 1.9 points, with 62 (9%) participants having symptoms of depression and 88 (13%) with anxiety. Table 1 shows differences across categories of individuals who were excluded from the study because follow-up interviews were missing versus those who participated. The former were older, less educated, more often retired/unemployed, had higher social risk scores, and more often had symptoms of depression and anxiety at baseline than those who completed the follow-up.
Baseline Characteristics of Atahualpa Residents Excluded and Included in This Study (Unadjusted Analyses).
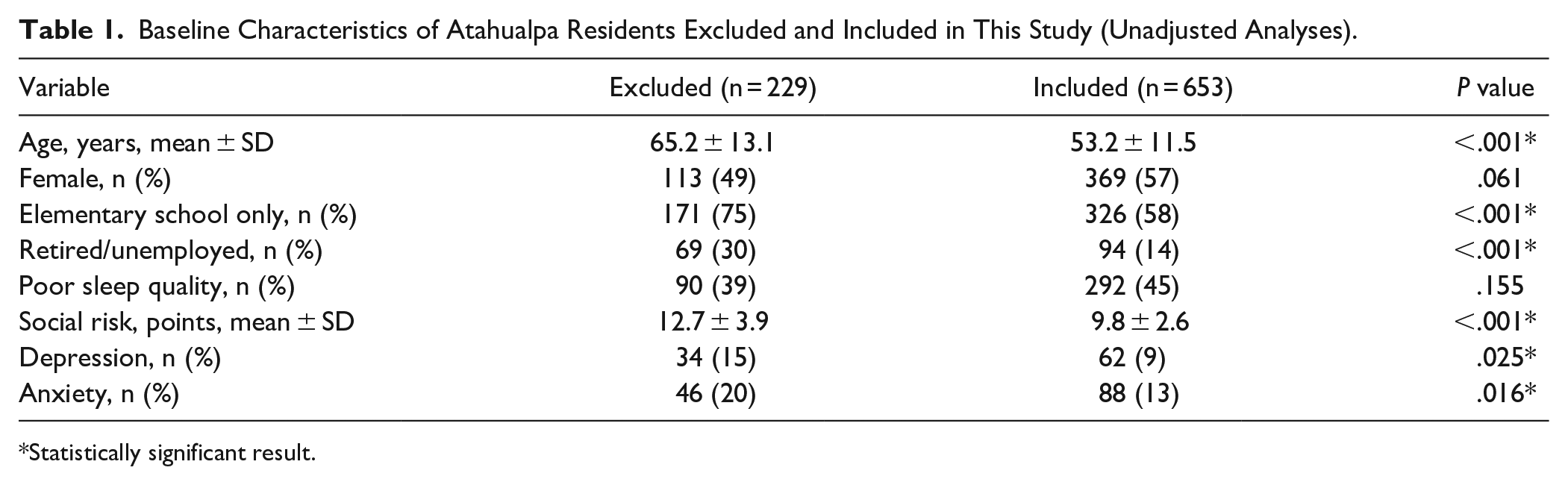
Statistically significant result.
Results of the Fear of Crime Questionnaire
The mean (±SD) total score in the fear of crime questionnaire was 7.07 ± 1.99 points in the whole series. Mean scores for the different items of this instrument were: 2.13 ± 0.97 for “how fearful are you of crime in your village?”; 1.15 ± 0.57 for “how do you perceive the crime rate in your village compared to neighboring villages?”; 1.60 ± 0.66 for “how dangerous it is to walk in your village during the daytime?”; and 2.21 ± 0.86 for “how dangerous it is to walk in your village after dark?”
Results at Follow-Up
At the time of follow-up, the mean score on the depression axis of the DAAS-21 was 2.3 ± 2.9 points and on the anxiety axis it was 1.5 ± 1.9 points. A total of 110 (17%) participants had symptoms of depression and 111 (17%) had anxiety. A worsening of symptoms of depression was noted in 84 (13%) cases and worsening of anxiety occurred in 88 (13%). Participants with worsening symptoms of depression had higher total scores on the fear of crime questionnaire compared to those who did not (7.61 ± 2.05 vs 6.99 ± 1.97; P = .008). Likewise, the fear of crime questionnaire score was higher among participants who had worsening of anxiety compared to those who did not (9.15 ± 2.20 vs 6.75 ± 1.75; P < .001).
Results of Statistical Analyses
Unadjusted linear regression models showed significant associations between the total score in the fear of crime questionnaire and worsening of symptoms of depression (β = .18; 95% CI = 0.06-0.29) and anxiety (β = .20; 95% CI = 0.12-0.29). Such associations persisted when models were adjusted for the specified covariates (Table 2). In the depression model, high social risk, poor sleep quality and levels of depression at baseline remained independently significant, while in the anxiety model only, poor sleep quality and levels of anxiety at baseline remained independently significant. Thereafter, we fitted another linear regression model where fear of crime was used as the dependent variable and both, depression and anxiety worsening, were included as independent variables. In this model, only anxiety worsening was statistically significant, while age, sex, and education remained as relevant covariates (Table 2).
Linear Regression Models Showing Significant Associations Between Fear of Crime and Worsening in Symptoms of Depression (Upper Panel) and Anxiety (Lower Panel) as Separate Dependent Variables.

Statistically significant result.
Discussion
This study exhibits the deleterious effects of fear of crime (self-reported) on measures of psychological well-being in middle-aged and older adults living in a remote rural setting of a country afflicted by escalating street violence and criminal homicides. About 13% of participants had worsening symptoms of depression and anxiety that were directly related to an increased perception of being a potential victim of crime. Multivariate models suggested that levels of depression and anxiety at baseline had an impact on the observed outcomes. In addition, poor sleep quality and higher levels of social risk may play a role in the perceived risk of victimization, a finding that was previously demonstrated in another study. 18 When both variables (depression and anxiety worsening) were used as independent variables in a model using fear of crime as the exposure, only the latter remained significantly associated with the exposure, suggesting that fear of crime is more significantly associated with anxiety than with depression worsening.
Several studies have investigated the association between fear of crime and psychological distress during periods of violence or other unfavorable circumstances.19 -21 While most studies confirm an adverse effect of fear of crime on psychological well-being, their results vary because of differing designs and variations in the study populations. 22 The impact of fear of crime on pre-existing psychological symptoms in a population that has been methodically evaluated before and during a peak of violence has not been adequately considered.
The present study opens avenues of research for the implementation of tailored interventions aimed at providing counseling to the most vulnerable individuals. Some individuals may be more prone to victimize themselves than others (between-person effect), and this behavior may result in more severe psychological (and even physical) consequences of street violence. Likewise, a premorbid predisposition may exacerbate the impact of fear of crime on psychological distress during periods of violence (within-person effects). 23 These considerations should be taken into account when tailoring interventions at the individual level.
The present study has potential limitations. One of them may be that the perception of risk of being a victim of violence may be greater than the actual risk. This exaggerated perception may be augmented by the media (and social media) with its disproportionate coverage of violent news. Another limitation is a possible self-report bias in the responses to the depression and anxiety axes of the DASS-21, and the internal inconsistency in the anxiety axis of this scale that has been noted in other studies. 12 However, our administration of the instrument by field personnel already acquainted with the study population is likely to have reduced the social desirability bias that may be responsible for inaccurate responses within sensitive topics, a finding previously demonstrated by our group. 24 In addition, there is the potential confounding impact of COVID-19 and its associated anxiety, isolation, and loss of productivity. Our group has published extensively on the morbidity of the SARS-CoV-2 pandemic in this community, but the additive effects on subsequent well-being are difficult to calibrate.25 -27 Certainly, the emotional and health effects of the pandemic may have increased the vulnerability of the population to environmental threats. Nevertheless, the trajectory of escalating violence in the community and fear of crime was already apparent well before the onset of this pandemic.
These limitations are offset by several strengths, such as the population-based design with a door-to-door identification and the subsequent unbiased enrollment of participants, the use of a validated field instrument to assess fear of crime as well as symptoms of depression and anxiety, and the homogeneity of the study population in terms of levels of education, lifestyles, income status, and living conditions. These similarities reduce the bias related to latent variables.
In summary, our study results show a significant aggravating effect of fear of crime on pre-existing symptoms of depression and anxiety in the study population and therefore overall well-being. Hopefully, recently introduced governmental policies aimed at reducing violence and crime will ameliorate the fear of crime and thereby diminish its impact on the psychological health of the population. 28
Footnotes
Author Contributions
OHD: study design, manuscript drafting; RMM: statistical analysis, significant intellectual contribution to manuscript content; DAR: study coordinator, data collection, and analysis; EEA: data collection and analysis; MJS: significant intellectual contribution to manuscript content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Universidad Espíritu Santo—Ecuador. The sponsor had no role in the design of the study, in the collection, analysis and interpretation of data, or in the decision to submit the manuscript for publication.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.