
Abstract
Academic Medical Centers (AMCs) and Federally Qualified Health Centers (FQHCs) are similarly tasked with managing the health of their local community, yet they each face unique challenges in their ability to do so. Integrating AMCs and FQHCs into novel care delivery models can leverage both organizations strengths, providing care in a comprehensive and sustainable fashion. Johns Hopkins Medicine (JHM) implemented this model with a large East Baltimore medical center, creating an AMC-FQHC collaboration focused on providing care to the East Baltimore patient population. This system provided various improvements in care delivery, including increased staffing, new wraparound services, improved access to funding dollars, and decreased out of pocket costs for patients qualifying for financial assistance. The academic missions of research and training were preserved, serving as the primary continuity clinic for several residency programs and as a community site for research. These changes resulted in more robust care for patients while improving the financial standing of the clinic. Through AMC and FQHC partnership, progress can be made toward providing holistic and financially sustainable primary care services in underserved areas while preserving the tripartite mission of academic medicine, with significant pedagogical and research opportunities.
Keywords
Highlights
Academic Medical Centers (AMCs) and Federally Qualified Health Centers (FQHCs) can collaborate to provide more comprehensive care in medically underserved areas (MUAs)
The integration of AMCs and FQHCs yields financial benefits and increases sustainability
AMC and FQHC integration is a reproducible model for delivering care in MUAs
Background
Academic Medical Centers (AMCs) and Federally Qualified Health Centers (FQHCs) both share a common goal of comprehensively managing the care of their local patient populations. Both entities often provide care in Medically Underserved Areas (MUAs) with high burdens of chronic disease and social strain. For AMCs, the needs of these populations can be significant, with reimbursement models that are often inadequate to cover the resource needs threatening sustainability of these centers. FQHCs (Table 1), by comparison, receive enhanced reimbursement from Medicaid and Medicare to provide a broader set of comprehensive primary care services which makes them a valuable strategic partner for AMCs. For FQHCs, partnership with an AMC can facilitate growth within their primary service area by building upon an existing clinic and patient base. Reducing investments typically needed for a new site and having support from a health system partner improves financial sustainability, and the unique clinic opportunity can aid in recruiting and maintaining the clinical workforce. We present in this manuscript the rationale and process for converting an AMC primary care clinic to an FQHC to address shared community care goals.
Key Features of Federally Qualified Health Centers.

Problem
In reviewing the rising primary care investment and increasing needs of the local community, JHM determined its current model to be financially unsustainable and sought opportunities to convert a primary care site into an FQHC. This collaboration had been considered previously, although it was not pursued due to concern for excessive turnover, risk to the educational training mission, and concerns about perceived abandonment of the community mission. However, as social needs grew atop mounting financial losses, a shared model of care became imperative to sustainability of the clinical site. JHM thus decided to pursue partnership with an existing FQHC.
Organizational Context
Johns Hopkins Medicine (JHM) sought to assemble an integrated AMC-FQHC model, leveraging the strengths of each organization to provide high-quality primary care services in a MUA in East Baltimore. Collaboration with an FQHC would allow JHM to enhance care for its local community through better addressing of social determinants and improvement in the financial sustainability of primary care services. While Maryland’s unique hospital all-payor rate structure helps support care in the hospital setting for underserved populations, this collaboration enhances resources and reimbursement in the non-regulated, ambulatory setting. 1 Our FQHC partner, noting the need for additional specialized medical services, was seeking opportunities to expand services in the same region. Conversion of a pre-existing JHM-owned clinical care site provided a unique opportunity to meet their community care goals and allow them to meet their patient engagement and access needs as required by the Maryland Insurance Administration and Medicaid Managed Care Organization (MCO) partners. Additionally, partnering with JHM allowed the FQHC partner to gain more MCO interest in allowing participation in value-based purchasing agreements.
AMC Site Selection
JHM began by selecting its target primary care site for conversion into an FQHC. We looked for a center located in a high-need community with poor health status indicators. We sought a freestanding location with a high patient volume and a high percentage of publicly insured patients. Additional factors accounted for were whether the site was a teaching location, its proximity to an existing FQHC, and due to the unique nature of the Maryland Total Cost of Care model, whether it was located in or outside regulated hospital facilities. 1 JHM ultimately selected East Baltimore Medical Center (EBMC), a large primary care site with approximately 40 000 patient visits per year. The EBMC site was initially a JHM primary care location, providing community services including but not limited to primary care services, OB/GYN, laboratory and dental services, pharmacy services, and community navigation resources.
FQHC Partner Selection
To select a partner FQHC, JHM released a Request for Application (RFA) to all Baltimore FQHCs outlining the key partnership goals noted in Figure 1. Financial and legal due diligence were completed for respondents to the RFA before selecting Baltimore Medical System (BMS) as the partner FQHC. BMS is the largest FQHC in Maryland, with 6 centers and 8 school-based health centers, and EBMC was located in their Health Resources and Services Administration (HRSA)-designated primary service area. They also had a longstanding care coordination relationship with JHM and share ownership of the largest Medicaid MCO in the state, which provides coverage for many of the patients.

Informing principles of AMC-FQHC collaboration.
Personnel Content
The team for this project involved leaders in 12 workstreams (Figure 2) with planning work beginning about 2 years before execution and continuing for a year after conversion of the AMC site to an FQHC. The Office of Johns Hopkins Physicians coordinated the broader structure and agreement, and Johns Hopkins Community Physicians leadership spearheaded the complex operational integration on the JHM side. FQHC leadership, led by their CEO, were fully engaged in the site conversion and brought forth matching operational leaders in all inter-entity workstreams. Full-time project management was needed from both organizations. BMS used a consulting service and JHM used existing project management team members to spearhead the complex operational integration. Weekly large operations meetings were used to review status of all major operational items throughout this transition, and there was significant investment in legal support to negotiate the 13 definitive agreements governing the collaboration as well as to execute over 40 new vendor contracts for the FQHC to maintain continuity of services at the care site. After launch, a Joint Steering Committee was formed to oversee the collaboration and a FQHC-approved JHM appointee was added to the board of directors while maintaining requisite FQHC board community majority.

Core workstreams informing AMC-FQHC collaboration.
Solution
EBMC was formally transitioned into a BMS health center. It was a HRSA-approved new service site operating under the BMS tax identification number (TIN). JHM retained employment of all providers and staff and leased them to the FQHC. Thus, while their JHCP employment and benefits were uninterrupted, they operated as BMS providers while at the site, billing under the BMS TIN and receiving FQHC reimbursement rates. The leased providers were not eligible for Federal Tort Claims Act (FTCA) coverage, and the additional malpractice cost was accounted for in determination of grant support for BMS. JHM hosted the site on the Epic platform via Epic Community Connect and provided key administrative services including scheduling and quality reporting. Quality reporting initially followed both JHM and BMS metrics although this proved to be redundant and often confusing given differing data definitions. The JHM quality team transitioned to the FQHC metrics driven by oversight needs and their value-based programs. An Epic Uniform Data System (UDS) report writer was in place to ensure adequate federal reporting capabilities. An interface was created between Epic and the BMS Electronic Medical Record (EMR) for billing purposes. A Joint Steering Committee with JHM and BMS provided oversight for the collaboration. Johns Hopkins Hospital (JHH) provided a Community Benefit Grant to BMS to support ongoing operational losses at the site.
We continued our residency training programs and program leadership defined expectations to ensure stability in staffing, panel size, and preceptor expectations. Research at the site is supported by an IRB reliance agreement with the School of Medicine and JHM helped to support creation of a BMS research review process to approve ongoing and new research projects at the site.
Exterior branding “BMS together with Johns Hopkins Medicine” reflects BMS’s ownership while demonstrating JHM’s ongoing commitment to the community. A multidisciplinary group including EBMC providers and staff members identified and prioritized incremental roles to support the clinic population based on their wish-list of resources. Eleven positions were ultimately approved including 1 physician, 2 mental health counselors, a substance use disorder counselor, 3 care managers/RNs, 2 certified diabetes educators/dietitians, and 2 community health workers. These roles were prioritized, considering their ability to be supported with FQHC reimbursements, their dependency on short-term grant funding, their cost, and their general need at the clinic.
Benefits of Collaboration
The primary benefit of the collaboration was enhanced support for the EBMC patient population and local community. There is greater community access due to the expansion of accepted Medicaid plans and EBMC adoption of the BMS sliding scale. BMS’s role as billing entity expanded access to discount drugs for attributed patients through the 340B program and increased access to care through additional partners that accept the sliding scale fees for services such as imaging, lab work, and dental care.
Additional benefits include enhanced access to grants due to the FQHC status, leading to increased HIV testing, PrEP access, linkage to care for HIV-positive patients, funding for a dedicated psychiatric nurse practitioner, and funding to support expansion of the Hopkins Community Connection Program 2 for patient navigation. This collaboration has also been beneficial during the COVID-19 pandemic, with EBMC being 1 of 8 high-risk clinics to receive targeted vaccine allocation from JHM and being the first Hopkins affiliated primary care site to offer in-clinic vaccination. BMS additionally selected JHM’s Care Transformation Organization to support its efforts in the state’s Medicare Primary Care Program.
JHH continues to provide a Community Benefit Grant to BMS to support the clinic’s financial standing, which remains improved from the escalating operating loss prior to the transition. Improved financial resources were allocated to additional navigational resources including Community Health Workers, expansion of care management beyond the Medicare population, and in person interpretation services. Partnering with JHM has been a value-add to provider recruitment for BMS, as there are mission-oriented clinicians interested in Johns Hopkins employment with access to its institutional benefits, integration with the educational mission, and differing clinical volume standards. Residency program recruitment statistics depicted a positive viewpoint from applicants and research metrics demonstrated promise, with 12 active ongoing projects at the site.
Challenges
Many challenges arose in the planning and execution of this collaboration. In Table 2 we document these by workstream.
Challenges in AMC-FQHC Implementation.
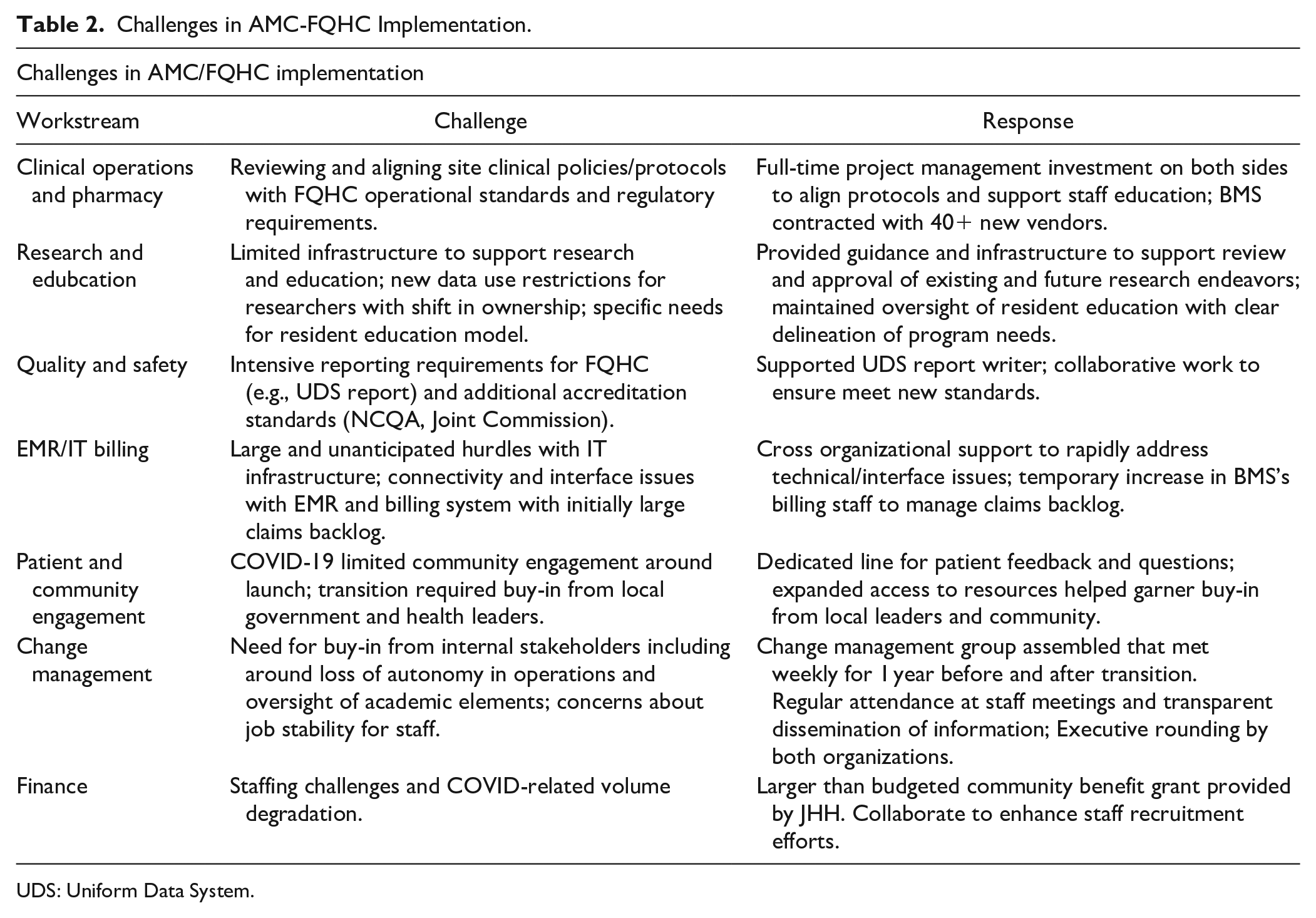
UDS: Uniform Data System.
Unresolved Questions and Lessons for the Field
Metrics related to the outcome of this collaboration are still evolving and remain significantly impacted by the pandemic given the clinic transitioned in June 2020. Access and meeting volume goals have remained a challenge primarily due to pandemic-era clinic staffing challenges. This has delayed new provider hires and had a prominent impact on the hiring of wraparound services, most notably behavioral health counselors. There were also significant increases in the self-pay, or uninsured, patient populations aligning with an increase in undocumented patients being seen at the site and across the broader health system after COVID. The uninsured population initially composed 10% of patients at this site, but grew to 15.7% of the patient population since this collaboration began. Grant funds were increased from initial estimates over the initial years of the collaboration to meet the increased financial pressures from changes in the payor mix.
Increasingly we are seeing such FQHC-AMC partnerships emerge across the nation to address shared challenges and commitments to local communities.3 -5 Long-standing collaborations such as the Center for Community Health Education, Research, and Service (CCHERS) 6 demonstrate the sustainability and comprehensiveness of these care models. Training opportunities are robust within a community-focused paradigm as well, with programs such as HRSA’s Teaching Health Center Graduate Medical Education Program (THCGME) 7 demonstrating the training potential within the community setting. Should other institutions seek to address care needs in their own community, it is essential to research the local primary care landscape to determine if an FQHC partnership could enhance resources or financial sustainability beyond what is currently in place. Additionally, early identification and addressing of potential barriers is critical. Proactive outreach to internal stakeholders and local healthcare and governmental officials can help garner critical support and assess stakeholder buy-in.
Through AMC and FQHC partnership, progress can be made toward providing financially sustainable primary care services in underserved areas. This collaboration combined expertise and made FQHC expansion more feasible through conversion of a previously JHM-owned site into an FQHC. FQHC expansion improves access to JHM’s extensive specialty network through geographic proximity, clinical relationships, and shared EMR, thus broadening the pool of affordable, specialized care for those in MUAs.
Innovative models can prepare for the unexpected by having a strong change management plan. Planning must begin early, and teams should meet frequently to ensure strong communication. Additionally, accountability must clearly be defined. Through preparation, we maintained support for key academic priorities and delivered on promises to the community through enhancement of key resources.
JHM continues to explore overall health outcomes and performance on various quality and experience metrics. This AMC-FQHC collaboration has been expanded to include an additional clinical site within Baltimore. Next steps include assessment of community experience, tracking outcomes of trainees, furthering research and educational opportunities, and determining best practices for other AMCs following similar strategies.
Footnotes
Author Contribution
All authors had a role in writing, editing, and reviewing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.