
Abstract
Health emergency outbreaks such as the COVID-19 pandemic make it challenging for healthcare systems to ration medical resources and patient care. Such disastrous events have been increasing over the past years and are becoming inevitable, necessitating the need for healthcare to be well-prepared and resilient to unpredictable rises in demand. Quantitative and qualitative based decision support systems increase the effectiveness of planning, alleviating uncertainties associated with the crisis. This study aims to understand how the COVID-19 pandemic has affected the performance of healthcare systems in different areas and to address the associated disruption. A cross-sectional online survey was conducted in the Kingdom of Saudi Arabia and the United Arab Emirates among healthcare workers who worked during the pandemic. The pandemic-related disruption and its psychometric properties were assessed using Structural Equations Modeling (SEM) with 5 latent factors: Staff Mental Health, Communication Level, Planning and Readiness, Healthcare Supply Chain, and Telehealth. Responses from highly qualified participants with many years of experience in hospital settings were collected and analyzed. Results show that the model satisfactorily fits the data with a CLI of 0.91 and TLI of 0.88. The model indicates that enhancing supply chain management, planning, telehealth usage, and communication level across the healthcare system can mitigate the disruption. However, the lack of mental health management for healthcare workers can significantly disrupt the quality of delivered care. Staff mental health and healthcare supply chain, respectively, are the highest contributors to varying degrees of disruption in healthcare delivery. This study provides a direction for more research focusing on determinants of healthcare efficiency. It also provides decision-makers insights into the main factors leading to disruptions in healthcare systems, allowing them to shape their outbreak response and better prepare for future health emergencies.
Keywords
Introduction
Healthcare (HC) is one of the largest and most complex sectors. It encounters challenges in providing consistent and adequate patient care services due to the continuous growth and aging of populations and accelerated rates of avoidable injuries and diseases. Potential pandemics and mass casualty events add to the complexity and strain HC systems worldwide, forcing governments to prepare and exercise complex plans. On January 30, 2020, the World Health Organization (WHO) declared COVID-19 a pandemic due to the severe health risk posed by this virus. 1 This pandemic spanned across all continents, making it an unprecedented health care crisis; to date, over 642 million confirmed cases and nearly 6.6 million deaths had been recorded worldwide. 2 Health systems, even the ones with the best infrastructure, are reeling under the burden of the disease and the increasing number of cases. The outbreak has significantly overwhelmed health systems and impacted the level of care for patients.
Most countries have responded promptly to the COVID-19 disease challenge by adopting considered and scientifically guided strategies for its containment. The response strategy involved implementing measures to reduce transmission risk (eg, social distancing, face masks, stay-at-home orders, and canceling public events). Specific measures were also implemented in medical settings, including prioritizing emergent care, rescheduling non-urgent appointments, delivering care remotely (Telehealth), and strictly isolating hospital wards dedicated to treating COVID-19 cases. The strategies and measures were deployed and used to manage the infection rate and avoid fatiguing limited hospital resources because of the absence of highly effective drugs, vaccines, and abundant medical resources.3,4
Technology in healthcare has been leveraged to combat this pandemic in multiple ways. Conscious efforts were taken to develop and adopt protocols that would lower infectious risk, reduce hospital burden, and reduce emergency medical care services by using artificial-intelligence-based predictors of survival and identifying the threshold to reduce medical resource burden. Examples include forecasting the spread of COVID-19 with an epidemiological Susceptible-Infected-Recovered model, 5 predicting bed capacity, ventilator availability, 6 or allocating resources. 7 These quantitative-based decision support systems establish a logical and comprehensible interface between the human user and data warehouse, allowing the transformation of raw data into timely and informed actions. 8 Moreover, telehealth technology has been useful during the outbreak, especially with those at greater risk of developing severe conditions of the COVID-19 disease (ie, patients with genetic diseases or elderly). Such technologies can facilitate optimal delivery of healthcare services to reduce cross-infection and transmission of the disease. 9
Despite increasingly enforced strict containment measures, health systems globally, especially at the beginning of the pandemic, faced the problem of predicting the number of infected cases, severity, and risk involved. Hence, challenges in estimating resource demand (eg, HCW, testing equipment, intensive care unit (ICU) beds, Personal Protective Equipment (PPE), and ventilators) were encountered. 10 As the demand for care suddenly and unexpectedly surges, even the facilities with large capacities are also prone to experiencing complicated decisions in resource planning. Rationing essential HC services and resources to cater to patients is a challenge for all HC systems. 11
The pandemic has further highlighted structural weaknesses in the healthcare supply chain (HSC) whose primary goal is to improve the quality and consistency of care delivered to patients. HSCs have often been considered different from the usual supply chain due to their high level of complexity, the presence of high-valuable medical materials, and the fact that they deal with human lives. 12 Most countries experienced difficulties and extended delays in restocking essential medical supplies due to forced lockdown and travel restrictions. 13 Maintaining the supply chain of medical products is not only paramount to cover the immediate medical response but will be fundamental to reducing disruption of the HC delivery system, which requires constant medicines, diagnostic tools, and vaccines for smooth functioning. 14
Moreover, the uncertainty associated with the pandemic and the ascending number of COVID-related deaths increase the fear of infection, overwhelming and burdening the mental health of HCW. Medical providers, especially, are exposed to susceptible cases while treating their patients. Prior to the COVID-19 vaccination control period, many HCW experienced feelings of inadequate support from their beloved ones while being isolated/quarantined. Working in these conditions put HCW at risk of severe psychological burden, affecting their health and wellbeing, as well as the care they provide to patients. 15
Communication and information transparency is the cornerstone of HC. Effective communication is critical for managing patient-centered care, both vertically and horizontally within the HC system. This includes engaging managers, HCW, and patients in decision making. An integral aspect of improving HC delivery is through “patient engagement” or “patient experience” (PE) activities. Engaging patients in decision-making (eg, via focus groups and evaluation) allows them to reflect on the provided care and address their health needs and personal preferences; hence, better outcomes. 16 However, there are insufficient research studies that evaluate the impact of PE on the quality of healthcare delivery. 17 Sharing valuable data and information across the system allows for sufficient flexibility to confront shifting pandemic conditions with proper planning of hospital capacity.
The purpose of this study is to assess the pandemic-related disruption on HC. Outbreaks have been increasing in the last years, threatening the HC sector and the quality of services. Existing disaster management in HC, globally, has failed to adequately respond to the COVID-19 pandemic. The association between the staff wellbeing, HSC, telehealth utilization, emergency preparedness, level of communication, and the resiliency of the healthcare system are often overlooked. An online survey questionnaire covering the above-mentioned areas was distributed among experienced HCW in the Kingdom of Saudi Arabia (KSA) and the United Arab Emirates (UAE). A 5 latent factors framework was developed using SEM based on the responses. Additionally, text mining from open-ended questions is also performed to analyze word frequencies reflecting common thoughts and opinions from the participants. This work provides a holistic approach to (1) gain more insight into the pandemic’s impact on HC systems, and (2) understand the correlational relationship between the discussed areas, allowing us to create resilient HC systems for the continuity of care during future outbreaks.
The remainder of the paper is organized as follows: a brief overview of the relevant literature is presented in Section 2. The proposed methodology is described in Section 3. The results and analysis are presented in Section 4. We discuss the implications of our study and present conclusions and directions for future research in Section 5.
Literature Review
Management and Planning of Healthcare Resources
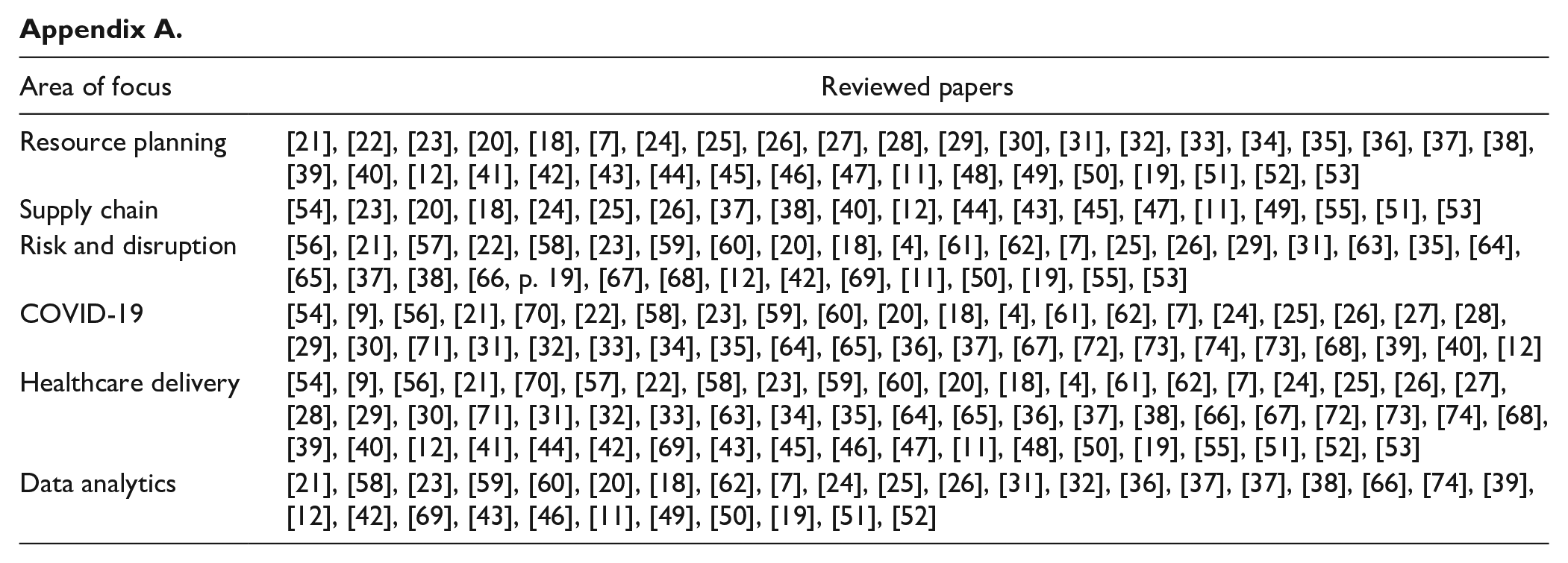
Effective emergency preparedness involves the early identification of shortages of medical resources and medical personnel. Intensive care units (ICU) beds, critical care staff, and ventilators are among the essential resources necessary to prepare for or contain an outbreak. In spatiotemporal research, the availability, shortages, and mismatches of HC workers, hospital beds, and ventilators during outbreaks had been correlated with statistical information on space and time, providing a greater understanding of effective distribution and allocation of the resources.11,18-20 Taking into account the spatial and temporal patterns of HC resources help in identifying the locations in which there are shortages and imbalances between the accessibility and patients’ demand. Yet, the area of supply chain in healthcare is insufficiently explored in the literature (see Appendix A). The reviewed papers were categorized into different areas which are Resource Planning, Supply Chain, Healthcare Delivery, Data Analytics, Risk and Disruption, and COVID-19. It is evident that more research should be conducted to understand the significant impact of resources management (ie, Supply Chain and Resource Planning) in healthcare delivery and disruption.
Emergency responsiveness relies on proper planning of hospital capacity; hence, effective communication and information systems across the supply chain (SC). 52 A successful integrated SC system involves the synchronization and sharing of valuable data (eg, visibility of the resources from suppliers to customers and vice versa) among the stakeholders. Factors such as shipment delays or travel bans during an outbreak can slow down the transport of supplies, influencing the quality of HC delivery. 75 Therefore, alternative mitigation strategies are encouraged to monitor hospitals’ inventory levels and empower responsiveness. Inventory management allows for efficient mitigation strategy through having a backup supplier for long-term disruptions, 12 or developing statistical forecasting methods. 51
Information visibility coupled with advanced analytical tools can generate innovative and proactive solutions to improve ongoing processes within the HSC, including inventory management and resource utilization and distribution. 43 Predictive analytics can support a better-integrated health system delivering continuous, coordinated, and comprehensive person-centered care to those who could benefit most. 76 Demand uncertainties are likely to happen during an outbreak, albeit data-based tools can improve stakeholders’ collaboration, real-time stock visibility and management, and effective handling of demand variability. While efforts to effectively treat and eradicate the coronavirus continues, so do the efforts of resource planning to support the provision of patient care in the event of a resurgence or future pandemic. Not controlling a disaster such as COVID-19 brings severe disruptions in SCs and the entire healthcare system and, thereby, irreparable losses will come into play. 77
Telehealth Technology
Global health has focused on slowing down the transmission of COVID-19 and reducing mortality associated with the pandemic by adapting strict strategies and policies. Some of the response strategies recommended by WHO include isolation of confirmed cases, and infection prevention and control measures to ensure the safety of frontliners in HC facilities. 1 Additional strategies for outpatient services were also adopted through providing mail delivery of medicine, telemedicine, virtual patient education, and monitoring. 54
Telehealth allows medical providers to deliver immediate diagnosis and consultations, and monitor and screen patients via different telehealth modalities such as: video-based virtual visits, telephonic delivery, and tech-enabled home medication. 9 In fact, a study has shown that sessions using telemedicine can take up to 10 more minutes of consultation compared to face-to-face visits that usually last less than 10 minutes per patient. 56 Telemedicine has also been useful for patients whose non-urgent visits were canceled or postponed. Pearlman et al, 21 modeled the number of new COVID-19 cases over time in relation to the total volume of hospital encounters and telemedicine visits. With the restrictions of limiting appointments to essential visits only, stay-at-home order, and increase of telemedicine visits, a significant decrease of COVID-19 cases was observed. The adoption of telemedicine reduces the exposure to infection and ensures the safety of patients and HC providers. Additionally, it reduces the need to use medical supplies, eliminating the burden on the SC. Nonetheless, some of the challenges for the successful provision of telehealth services include limited physical examination, lack of technological skills, information security, resource availability/accessibility, or technical issues. 78 A hybrid care delivery model that combines in-person visits and telemedicine is, in fact, encouraged in the future, although it needs further assessments and evaluation of the current telehealth model. 70
Employee Wellbeing
The COVID-19 pandemic surge has caused long-term and persistent psychological consequences among the HC workforces. Several recent studies reported that most frontline employees appeared to suffer from stress, depression, anxiety, and insomnia.79,80 The increasing demand to combat the pandemic required longer work shifts and minimized social and family support, quickly leading to burnout physically and psychologically.79,80
Zhang et al 81 surveyed HCW in China during the first outbreak, and found that health status, overtime working hours, maladaptive coping, fear of contagion and less family contact are independently associated with employees’ burnout. 81 Additionally, Holton et al 82 conducted a survey in an Australian hospital and reported severe symptoms of stress and depression among nurses and midwives compared to mild symptoms among doctors. 82 Kreh et al 83 interviewed HCW in Italian and Austrian hospitals during the first phase to study the psychological experiences and coping strategies. Interviewers stated that anxiety-related fear was exacerbated with feelings of guilt, frustration, and powerlessness in containing the virus. Moreover, new work routines, PPE availability, and patient-provider communication changes were the top main stressors during the pandemic. Despite major stressors in clinical settings, the interviewers pointed out the importance of teamwork, and connectedness among all staff in managing and coping with difficult situations. 83
The outcomes of not supporting the health and wellbeing of employees in healthcare could weaken and incapacitate employees from delivering to patients the quality of care. Implementation of timely psychological counseling and intervention for HCW are recommended to improve mental health and overall healthcare delivery. 84
Surveys on COVID-19 Impact on Healthcare
A thorough review of the literature focusing on work related to surveying the medical workforce during the pandemic shows that patient engagement and the effectiveness of telehealth were insufficiently investigated in research.
In a cross-sectional study in Jordan, Alhalaiqa et al 85 investigated the relationship between psychological problems and the resiliency level of frontline workers. They reported significant increased levels of stress and decreased levels of resilience with anxiety and depression. They also found that the level of resilience is low with inadequate PPE, and among older HCW who have many years of experience. 85 Depression and anxiety were also experienced by patients with ongoing treatments. Boer et al 86 surveyed asthma patients and found that many have avoided going to hospitals during the lockdown and delayed their medical care due to fear of COVID-19 infection, which was associated with increased anxiety and depression. Patient experience is, however, an entirely new and poorly explored area of research. Collecting such valuable information would help us in identifying gaps and opportunities to improve patient care. 87 With limited access to care, the implementation of telehealth modalities resulted in great satisfaction among caregivers and patients. A survey study prepared by Telehealth Work Group and answered by qualified HC professionals show that telehealth has improved patients’ health with enhanced timeliness of care, and has motivated HCW to use it in their practices as it increased satisfaction in their work. 88 Nevertheless, the literature lacks investigation in the effectiveness and performance of telehealth in delivering a quality care.
Reviewing the literature has showcased that resources management, employee wellbeing, and telehealth play essential roles in the quality of healthcare delivery, especially during health outbreaks. To the best of our knowledge, no existing work was found to include all the different areas of focus which are Staff Wellbeing, Patient Engagement, Resource Management, Telehealth, and Quality of HC Delivery, Moreover, most of the survey studies targeted only medical providers who were on the frontline against the pandemic, but more attention should be made to the other groups of employees in healthcare (ie, managers, support staff, patients, and medical students), as well as patients.
Methods
An extensive literature review was conducted to identify indicators of HC delivery effectiveness and answer the research questions of this work. Based on the literature and experts’ opinion, a survey was developed and evaluated by 5 HC professionals for improvement. The finalized version of the survey was deployed using SurveyMonkey, and distributed digitally to HC professional via Linkedin, Whatsapp, and Telegram platforms. Survey responses were later analyzed using mathematical tools and text mining.
Survey Design
An anonymous cross-sectional survey study, consisting of 8 categories, as illustrated in Figure 1, was conducted between October 1 and 27, 2021. The survey questionnaire was designed to address and gather information about different determinants that could influence the quality of HC delivery (eg, hospital preparedness and coping mechanisms of operational, tactical, and human resources). Upon experts’ revision of the questionnaire and institutional review board approval, a digital survey was distributed among HC professionals working in health facilities in KSA and UAE.
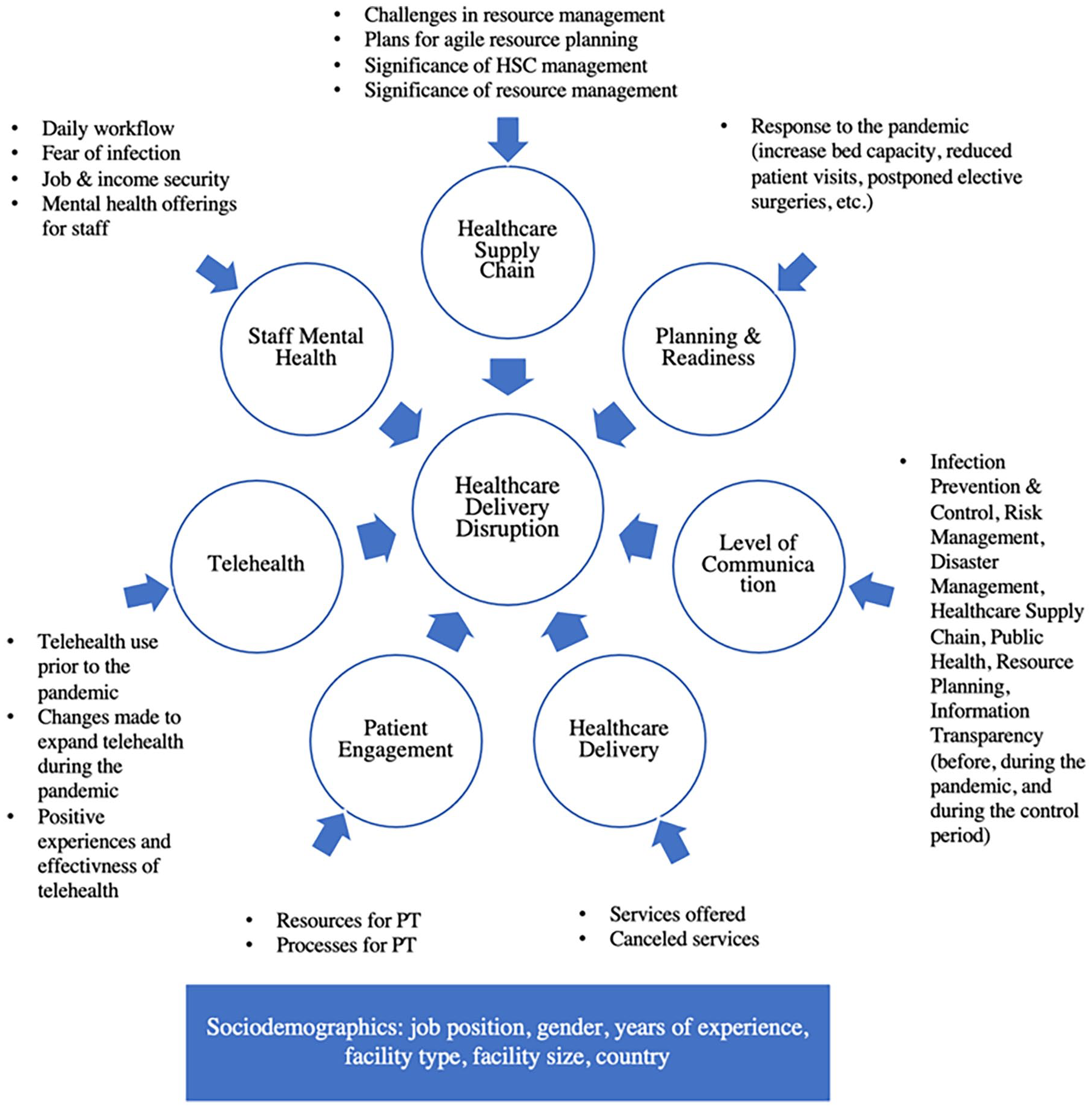
Survey categories and component.
Structural Equation Modeling
SEM is a causal inference approach that includes multiple statistical techniques. Confirmatory factor analysis (CFA), particularly, is a technique in SEM that links observed variables (OV) in the dataset (eg, responses) with unobserved/latent variables (LV) (eg, factors causing disruption), such that it confirms the underlying psychometric structure of a hypothesized model. 89 The desired outcome of SEM can be numeric estimates of the hypothesized relationship or logical implications implying how variables are related and unrelated to each other (ie, covariance-based analysis). 90 The closer the hypothesized model is in corresponding to the characteristics of the data observed, the greater the fit. Because LV are only a function of the OV, a scale must be set for each of those variables to estimate their variances. This can be done with the variance standardization method as it fixes the variance of each variable to 1 such that the factor loadings are freely estimated, allowing easier interpretation of correlations with relative size. 91 The correlation between OV can also be measured. Moreover, the outcome variable is regressed onto LV (OV, essentially).
Since this study investigates the causal effects between items, the null hypothesis, which states no existing relationship, must be rejected; hence, smaller p-value in the chi-square test is desired to prove dependency among the variables. 91 Other common goodness-of-fit measures in SEM include Tucker-Lewis Index (TLI) and Comparative Fit Index (CFI); these indices compare the model with a baseline model (with no covariances), and develop indices based on how much improvement is there in model-fitting. Therefore, values closer to 1 indicate that the model is saturated and fits the data perfectly. Moreover, Root Mean Square Error of Approximation (RMSEA) measures discrepancy or miss-fit; thus, values less than 0.05 correspond to a good fit.92,93 RStudio software was used to construct the SEM instrument. To visualize the covariance and regression relationship between the survey components, CFA, particularly, was carried out using lavaan package in RStudio to test the hypothesized model and confirm the known relationship (based on literature review and HCW opinion). Referring to Tables 1 and 2, the construct includes the average of questions corresponding to each of the following variables:
Five factors (ie, latent variables) describing Staff Mental Health (f1), Communication Level (f2), Planning (f3), HSC (f4), and Telehealth (f5).
The outcome variable (y) representing “Healthcare Disruption” as a function of the factors f1 to f5.
Sociodemographic characteristics.
SEM Variables With Their Respected Indicators/Sub-Questions.

Healthcare Planning & Management: HSC, Public Health, Resource Planning, Information Transparency.
Risk factors and management: Infection Prevention & Control, Risk Management, Disaster Management.
Sociodemographic Characteristics.
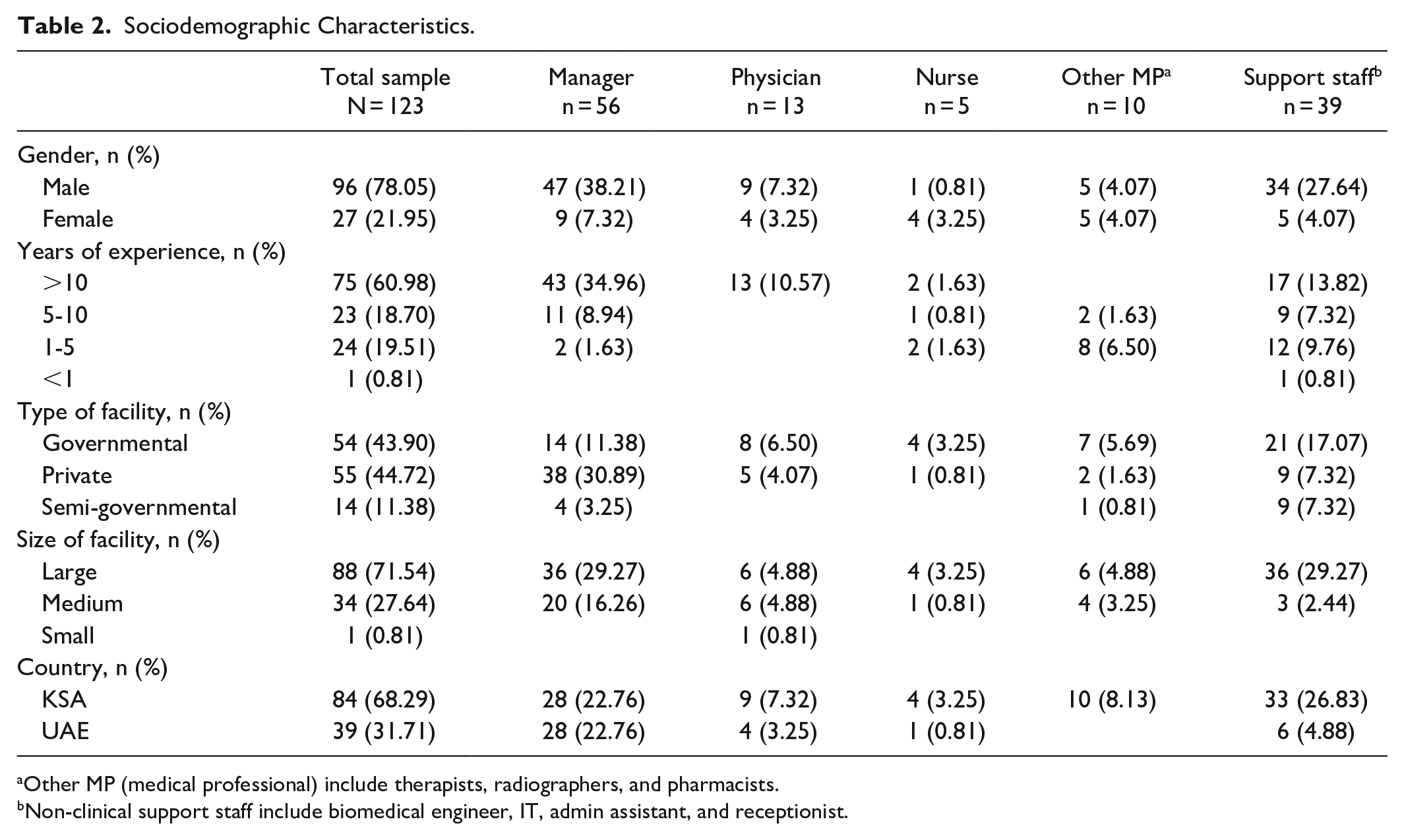
Other MP (medical professional) include therapists, radiographers, and pharmacists.
Non-clinical support staff include biomedical engineer, IT, admin assistant, and receptionist.
Text Mining With RapidMiner
The survey also included 2 open-ended questions: (1) “How did COVID-19 pandemic positively affect your facility?”, and (2) “What are your recommendations for better preparation and responses to future health outbreaks?”. Responses were analyzed with text mining techniques in RapidMiner software. Analysis of word occurrence frequency for each question was performed using built-in operators. The operators remove missing content, convert all entries to string attributes, and process the documents via sub-operators (eg, breaking the sentences, removing stop-words, eliminating suffixes, and grouping synonyms).
Results
Data Preparation
A total of 225 responses were collected from healthcare professionals, but only 123 responses with ~90% completion are included in the analysis. Missing values in the raw dataset were removed using RStudio. Table 2 shows distribution details of respondents’ job position, gender, years of experience, type, and size of the hospital facility. In this work, responses were collected from HCW working in KSA (68%) and UAE (31%) due to the similar infrastructure of the health systems in those countries.
Results Interpretation
Statistical analysis
Responding to the COVID-19
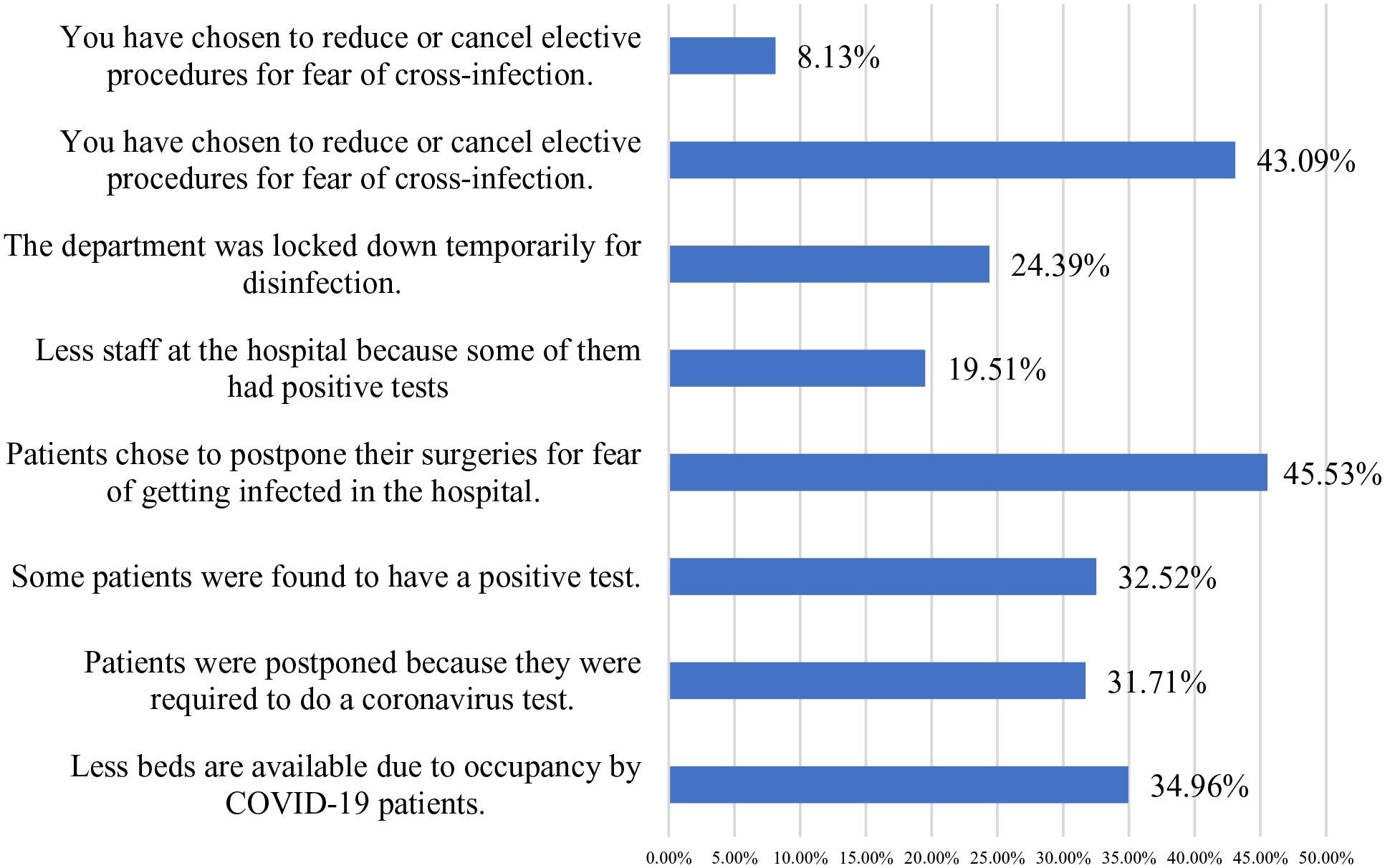
Response rate for the reasons behind canceling elective services during the outbreak.
Challenges encountered
Communication in healthcare

Very Good response rates to levels of communication before and after the peak of the pandemic.
Pandemic outbreaks can cause long-term propagating disruptions in health systems, and systems that are not resilient enough less likely to anticipate, adapt to, or mitigate disruptions, complicating resource allocation decisions. While the world is facing the urgency of the COVID-19 pandemic, policymakers must plan to respond to the outbreak while minimizing its collateral impact directly. 14 More than 38% strongly believe that mitigating pandemic disruptions can be achieved through having multiple suppliers (38.18%) with improved cooperation between the organizations (45.45%) and developing an agile and innovative culture in the SC (38.18%). Similarly, up to half of the respondents reported that developing risk management plans (50.90%) and implementing/enhancing the use of IT and analytics (49.09%) are significant in managing the HSC and reducing the associated disruptions.
Impacts on different specialties
The rise of healthcare demand and costs puts decision-makers under pressure to ensure efficient capacity management across the entire healthcare system. Many of the non-emergency procedures in dental practices were postponed at the beginning of the pandemic, and dentists faced problems providing PPE. 47
Figure 4 shows how the pandemic influenced healthcare services in different specialties due to high risk of COVID-19 infection. More than 50.41% of the respondents reported that their dental/oral services were postponed or canceled during the outbreak, and around 31.71% said dental/oral services were extensively disrupted. As part of the preventative measures recommended by WHO, elective general surgeries have been widely postponed to reduce cross-infection 1 ; this, however, resulted in greater impact even when services began to resume with the control period. Up to 34% reported cancellation of general surgeries, and 30% reported disruption in that specialty. The number of dermatology services offered also declined, as reported by 34% of the sample group, but 34.96% said they had virtual services for those departments. The most disrupted services were the ones offered in Emergency Department (47.97%), and ICU (39.84%). Many hospitals reduced the number of ED visits to contain the virus, and patients’ also feared to utilize ED services during the peak. 96 The ICU, in contrast, experienced a surge of critically ill patients as the number of confirmed COVID-19 cases increased. 97 Almost all hospitals experienced a shortage of ICU beds and resources that led to hard allocating choices. 98 Effective expansions of healthcare capacity and medical services need to be improved to ensure the continuity of care.
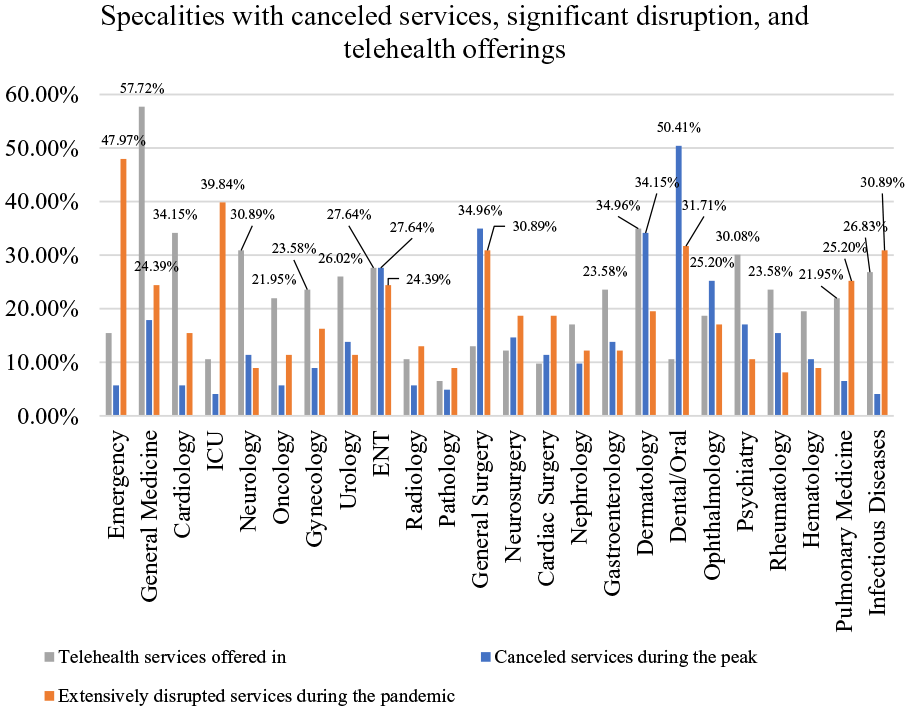
COVID-19 impact on different specialties.
Pandemic-related disruptions can be alleviated with telehealth offerings, especially with challenges related to lockdowns and resources shortages.9,56 Fortunately, respondents reported that their facility had telehealth offerings to provide consultations and services for General Medicine (57.72%), Dermatology (34.96%), Cardiology (34.15%), Neurology (30.89%), Psychiatry (30.08%), ENT (27.64%), Infectious Diseases (26.83%), and Urology (26.02%). In addition, 23.58% of participants said they offered Gynecology, Gastroenterology, and Rheumatology services through Telehealth, and 21.95% said they offered virtual services for Pulmonary Medicine and Oncology. However, telehealth systems need to be enhanced in the long run given the significant advantages of cost savings, patient convenience, and support for resources constraint. 99
SEM analysis
Evaluating model fit
Multiple SEM models with different combinations of factors and indicators were tested out, and the best model satisfying measurement fit and confirming the hypothesis was chosen. Based on model-of-fit indices, the model fit can be further improved by improving those indices. 100 The 5-factor model (with df = 289) has a value of 0.910 for CFI, and 0.876 for TLI. Having values of TLI and CFI closer to 1 means that this model fits the dataset almost perfectly (ie, a saturated model). 92
Although both of those indices are recommended to be above or equal to 0.9 for the best-fitting model, the P-value (χ2) is less than .001 and RMSEA is 0.046, which means that the results are significant in supporting the theory being investigated and that the model is a close-fit. Additionally, CFA models consider the ratio of χ2/df, and it is recommended to be less than 0.001. 101 This model has a ratio of ~0.0000346; hence, the model resulted in an acceptable fit.
Model parameter estimates
Parameter estimates in SEM represent the weight of loading among variables. The SEM model for this paper is presented in Supplemental Figure 6 with the variable of interest (y), the latent variables or factors (f1-f5) and their associated observed variables (indicators). The values of estimates for each correlation are presented, and greater loadings are illustrated in darker shades (ie, dark blue and dark red). Dotted lines indicate fixed parameters as seen in factors’ variances and covariances among sociodemographic items. The correlation estimates between a latent variable and an observed indicator are listed in Supplemental Figure 6. This shows that causal relationships do exist between the selected survey questions and the constructs (unobserved variables). The highest the parameter estimate, the greater the correlation.
Regression estimates are also shown in Supplemental Figure 6. From the rate of responses, the variable of interest is expected to carry out an average low value because most responses had low scores (negative impact on HC). Referring to Supplemental Figure 6, the observed variables for f2, f3, f4, and f5 consist of high scores (positive impact on HC), opposing the direction of y. This means that Communication Level, Planning and Readiness, Healthcare Supply Chain, and Telehealth are negatively correlated with Healthcare Delivery Disruption by estimates of −0.053, −0.096, −0.260, and −0.085, respectively. Therefore, improving the communication level, planning, HSC, and telehealth usage, reduce disruptions in the quality of care.
On the other hand, f1 consists of low scores, which goes linearly with y. Accordingly, staff mental health is positively correlated with healthcare delivery disruption; hence, increasing the burden effect on HCW mental state by .434, disrupts the delivery of care by ~.434. Regardless of the direction, the top highest contributors to varying Healthcare Delivery Disruption are Staff Mental Health (.434) and Healthcare Supply Chain (−2.260). In other words, the psychological wellbeing of HCW, and HSC significantly affect the quality of healthcare delivery.
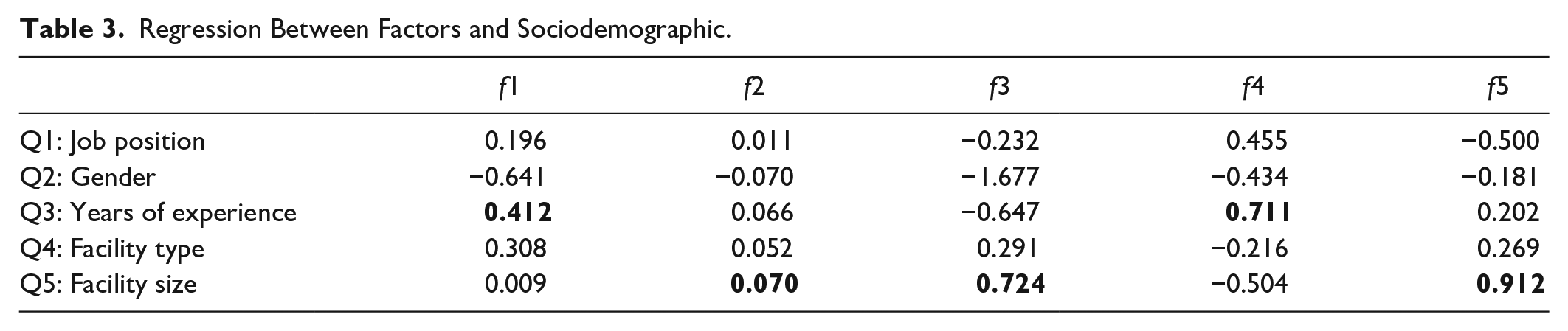
Sociodemographic characteristics were also regressed onto the latent variables to observe possible correlations (Table 3). According to the model results in Table 3, the size of the hospital setting is positively correlated with Telehealth (.912), Planning and Readiness (.724), and Communication Level (.070). Having a large capacity within the HC system allows for greater implementation of Telehealth, and greater resources for planning and communication. Additionally, responses to HSC were mostly answered by participants with higher experience in healthcare, explaining the high correlation value of .724.
Regression Between Factors and Sociodemographic.
The SEM model also measured covariances among the latent variables, as shown in Table 4. Mental health (f1) and HSC (f4) were found to have the strongest covariance relationship in the model with a value of .754. Many current survey studies, in fact, have been investigating the effect of supplies availability on the mental wellbeing of HCW. In a recent study, 85 a measurement scale that measures the resilience and ability of nurses to overcome challenges (ie, anxiety or depression) has been shown to be lower among the groups who had adequate PPE. Similarly, Planning and Readiness is strongly related to Telehealth by an estimated value of .359 and related to Communication Level by an estimated value of .110. WHO recommends that the risk planning process include the development of remote methods such as online consultations and teleworking for the continuity of health services. 102 Moreover, for proactive planning, it is imperative to maintain the highest levels of communication across the HC system.
Covariances Between Latent Variables.

Text analysis
To extract meaningful insights of the 2 open-ended questions asked in the survey, Figures 5 and 6 represent the percentage of word frequencies detected in the texts using RapidMiner. Eighty-seven participants responded to the first open-ended question, “How did COVID-19 pandemic positively affect your facility?”, and 16% of the responses reported that the pandemic had improved the management and planning in their facility. Other responses imply that this pandemic has positively affected their facility through prioritization of patient care and resource management, raising awareness and dealing with health emergency disasters, becoming more proactive and agile, improving the quality and infection control, enhancing teamwork and communication, and technologies such as the use of Telehealth and remote work.
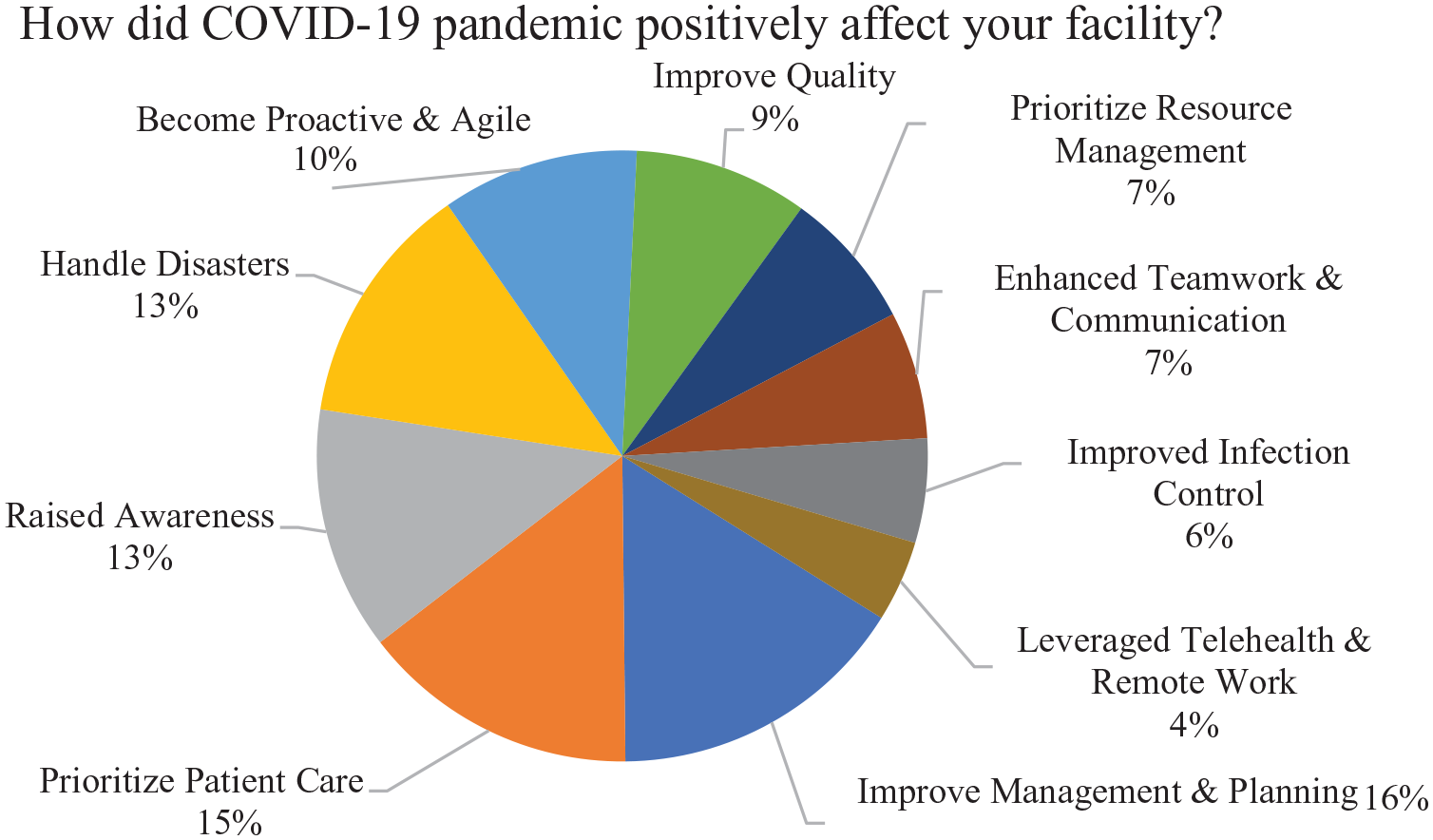
Total word occurrences (COVID-19 positive impact).
Total word occurrences (recommendations for future outbreaks).
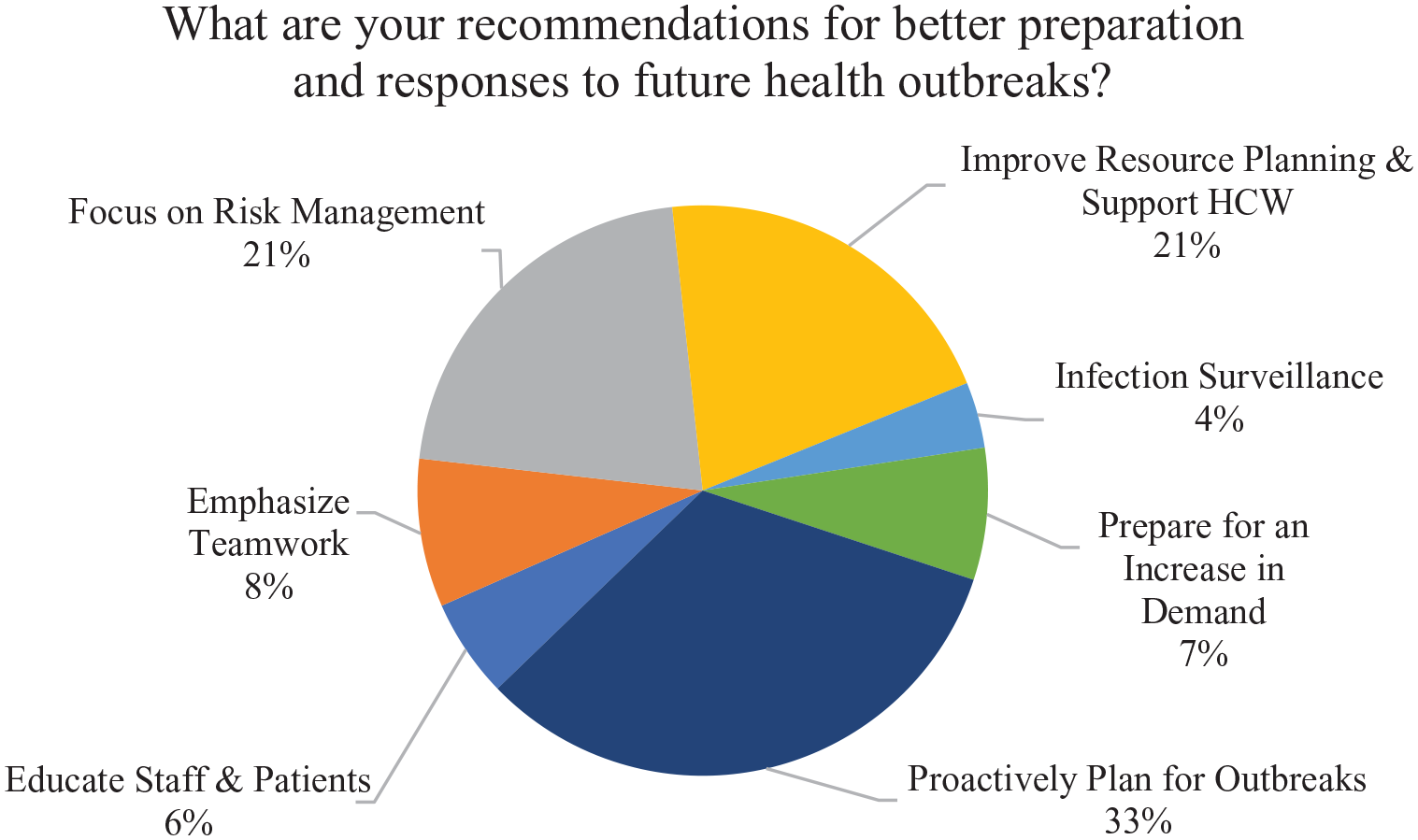
The second question “What are your recommendations for better preparation and responses to future health outbreak?” recorded 86 answers. The majority of responses (33% occurrences) emphasized the necessity of proactive planning for future outbreaks. Other recommendations included: improving resource planning and supporting HCW, preparing for an unprecedented increase in patient demand, strengthening risk management and infection surveillance, building a culture of teamwork, and educating and training all staff and patients about strategic response plans.
Views from participants regarding COVID-19 positive effects:
“Learn to handle challenges, work in a team environment, patient care experiences to new level.”
“Flexibility in working place, staff can work anywhere they want.”
“Our preparation for a pandemic is definitely better now. Our reaction time to certain medical conditions, which require mass activation and flexibility in process, has improved. Our strategic plans are inclusive of opportunities which will arise post the pandemic. Our infection control and risk management departments are more efficient and authoritative in their actions.”
“Improved the practice of infection control, high awareness of protocols, increased quality practice, risk management and establishment of disaster department.”
“Made us aware of our vulnerabilities in several areas in Supply Chain and workforce planning. It also opened the doors for a more agile healthcare model.”
Views from participants regarding recommendations for future outbreaks:
“Our biggest learning networking between hospitals for staff and material needs are of top priority. Scientific collaboration in terms of excellence in treatment protocols have to be shared more often than not between the elite doctor community with the smaller facilities as well. Using technology to upgrade our services should not be optional but mandatory from the health authorities.”
“Use more technology to improve the service, engage patient in such decision if there is any pandemic how we can reach and treat you, engage more staff in decisions and to innovate solutions for the future care.”
“More and more communication from authorities and hospitals to be part of command center communications and transparency from all stakeholders.”
“It was something new for everyone. Lockdowns stopping of elective surgeries. But it has impacted on the financial of the organization. We should plan this in future how to overcome these financial burdens by putting something behind to manage and overcome these financial crises.”
“Daily debrief and weekly steering of hospital readiness committee is a must. Proper resource planning is a must.”
Discussion and Conclusion
The massive, unprecedented disruption in HC caused by the COVID-19 outbreak has forced policymakers to rethink HC delivery and disaster preparedness. The poor performance of the HC systems globally, especially during the initial response to the pandemic, has showcased the vital roles of a resilient healthcare system and effective utilization of data and technology in preparation for health emergencies. Using SEM (specifically, CFA) and text mining, the goal of this paper was to assess the influence of the COVID-19 pandemic on the delivery of healthcare systems.
The developed SEM instrument was based on complex survey data (collected from HCW in KSA and UAE) covering the areas of staff psychological wellbeing, HSC, Telehealth, planning, level of communication, and HC delivery disruption. The 5-factor CFA model was found to be of a reasonably good fit for the hypothesized model, as all of the fit indices (CFI = 0.910, TLI = 0.876, P < .001, RMSEA = 0.046) are within acceptable values. From the model results, disruptions in HC delivery can be reduced by having effective communication level, emergency planning, telehealth utilization, and resilient HSC. However, the increase of psychological burden in HCW increases the disruption. Among those 5 factors, the factors that were highly correlated to HC delivery disruption were HSC (negatively) and mental health (positively).
The instrument needs more evidence of construct validity and reliability, as well as a larger sample size. With more dataset and relevant observed variables, measurement fit indices can be improved; the closer the CFI and TLI values to 1, the greater the user fit to a saturated or perfect fit. 100 Apart from improving the fit indices, a measurement model with less than 7 factors (each with +3 indicators), is recommended to have a minimum of n = 150 to ensure significant construct and convergent validity. 103 About 45% of the total survey takers did not complete the survey, thus only 123 responses were considered for analysis. Moreover, parameter estimates/loadings are greater when questions (observed variables) are perfectly matching the intended meaning of the factors (latent variables). Misinterpretation of the questions wording in the survey may have resulted in confusion, influencing the actual scores of latent variables.
Using text analysis, results show that positive impacts of the COVID-19 outbreak, as stated by the participants, include the improvement in their hospitals’ management in terms of emergency planning, and prioritizing patients and resources. A rise in technology utilization, awareness, and teamwork during the pandemic were also reported. Furthermore, the majority of the participants highlighted the importance of being proactive in withstanding future emergencies. This involves the strengthening of risk management, IP&C, and resource planning, as well as providing sufficient education/training to staff and patients regarding response plans.
The HC sector faces serious challenges in the coming years, as the population ages, chronic diseases prevail, and health issues will likely emerge. The integration and sharing of qualitative and quantitative data are crucial in creating efficiencies, as they allow us to continuously monitor the performance of health systems and evaluate the return on investment. The future of HC enterprise may become dependent on robust data resources and the use of advanced analytic techniques in favor of keeping pace with increasing demands in the health system. An effective response during challenging times, as recommended by Schmidt et al, 95 requires: the availability of technology (for surveillance and telemedicine), well-established surge capacity management and emergency plans (for managing and allocating resources including emergency responders), agile HSC, and strong public health infrastructure. Expanding partnerships and collaborations among health sectors and investing in HC systems aid the successful implementation of a robust and flexible care delivery model.
This proposed work with the promising SEM findings and insights from HCW can help the healthcare system to further study and validate the significant impact of the investigated areas on the quality of HC delivery. It also paves the way for developing predictive analytics to track potential disruptions, and to take the appropriate steps toward ensuring the continuity of care during future pandemics.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241260351 – Supplemental material for Assessing the Disruption Impact on Healthcare Delivery
Supplemental material, sj-docx-1-jpc-10.1177_21501319241260351 for Assessing the Disruption Impact on Healthcare Delivery by Maymunah Fatani, Abdulrahim Shamayleh and Hussam Alshraideh in Journal of Primary Care & Community Health
Footnotes
Appendix
| Area of focus | Reviewed papers |
|---|---|
| Resource planning | [21], [22], [23], [20], [18], [7], [24], [25], [26], [27], [28], [29], [30], [31], [32], [33], [34], [35], [36], [37], [38], [39], [40], [12], [41], [42], [43], [44], [45], [46], [47], [11], [48], [49], [50], [19], [51], [52], [53] |
| Supply chain | [54], [23], [20], [18], [24], [25], [26], [37], [38], [40], [12], [44], [43], [45], [47], [11], [49], [55], [51], [53] |
| Risk and disruption | [56], [21], [57], [22], [58], [23], [59], [60], [20], [18], [4], [61], [62], [7], [25], [26], [29], [31], [63], [35], [64], [65], [37], [38], [66, p. 19], [67], [68], [12], [42], [69], [11], [50], [19], [55], [53] |
| COVID-19 | [54], [9], [56], [21], [70], [22], [58], [23], [59], [60], [20], [18], [4], [61], [62], [7], [24], [25], [26], [27], [28], [29], [30], [71], [31], [32], [33], [34], [35], [64], [65], [36], [37], [67], [72], [73], [74], [73], [68], [39], [40], [12] |
| Healthcare delivery | [54], [9], [56], [21], [70], [57], [22], [58], [23], [59], [60], [20], [18], [4], [61], [62], [7], [24], [25], [26], [27], [28], [29], [30], [71], [31], [32], [33], [63], [34], [35], [64], [65], [36], [37], [38], [66], [67], [72], [73], [74], [68], [39], [40], [12], [41], [44], [42], [69], [43], [45], [46], [47], [11], [48], [50], [19], [55], [51], [52], [53] |
| Data analytics | [21], [58], [23], [59], [60], [20], [18], [62], [7], [24], [25], [26], [31], [32], [36], [37], [37], [38], [66], [74], [39], [12], [42], [69], [43], [46], [11], [49], [50], [19], [51], [52] |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by AMerican University of Sharjah under project ID FRG22-C-E02. The work in this paper was supported, in part, by the Open Access Program from the American University of Sharjah.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.